

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The development of diagnostic organ imaging has resulted in increased detection rates of renal cell carcinoma, downward staging of tumors to stage 1, and a decrease in the sizes of tumors detected. Partial nephrectomy (PN) has similar oncologic outcome (1) but has been associated with better conservation of renal function than radical nephrectomy (RN) (2). Thus, American Urological Association guidelines recommend PN as the standard treatment for T1a tumors, but there are still many methods of PN that could be considered.
Further developments in minimally invasive techniques and surgical apparatuses have resulted in laparoscopic PN (LPN) becoming an alternative to open PN (OPN), since LPN is associated with reduced surgical morbidity rates and similar intermediate-term cancer survival (3). LPN, however, demands advanced surgical skills, has a gradual learning curve, and requires perseverance, all of which limit its widespread use (4).
The advent of robotic surgical systems has helped reduce the technical challenges posed by LPN and made the learning curve more rapid, without negatively affecting perioperative outcomes (567). But some studies have indicated that, robot-assisted partial nephrectomy (RAPN) tend to have a longer ischemic time, although RAPN was regarded as a suitable alternative to OPN (8910). Unfortunately, comparative studies until now about renal function were mainly focused on total glomerular filtration rate (GFR), not split renal function. Of course, result of these studies is important, but more than 5 percent of renal cell carcinoma (RCC) patients can be suffered by cancer of contralateral kidney (11). In view of that point, comparison of renal function of operated kidney according to surgical methods may have significant implications.
This study was designed to compare long term post-operational renal function change in patients undergoing RAPN and OPN. Since the choice of operation has been affected by the intricacy of the tumor, propensity score matched cohorts were compared.
MATERIALS AND METHODS
Between 2007 and 2013, 418 patients underwent PN at our institution. Among them, patients who underwent two operations on the same kidney and with Von Hippel-Lindau disease, a horseshoe kidney, or a ruptured angiomyolipoma were excluded (n = 15). From these, a cohort of 403 patients (including 114 who underwent RAPN and 289 who underwent OPN) were selected and included in this study. To reduce the differences of patient characteristics between the two surgical methods, patients were matched by propensity score on patient age and tumor size, depth, and location. The nephrometry score was categorized as low, 4–6; intermediate, 7–9; or high, 10–12 (12). Among 114 RAPN patients, 84 patients underwent Tc-99m diethylenetriaminepentaacetic acid (DTPA) scintigraphy 3 months, 1, and 2 years after surgery, and 84 OPN patients were propensity matched 1:1 with RAPN patients.
The selection of operational method was based on discussions with patients, while taking into consideration tumor mass characteristics, patient comorbidities, and costs. In Korea, national insurance covers only OPN, making RAPN more than twice as expensive as OPN. Data collected retrospectively from patient records included age, sex, operation method, body mass index (BMI), pre- and post-operative GFR, tumor size and location, comorbidities (including diabetes mellitus and hypertension), R.E.N.A.L. nephrometry score (including radius, exophytic property, nearness to the sinus, anteriority, and location relative to the polar lines of the tumor), perioperative variables (including operation time, ischemic time, and hospital days), complication (according to Clavien-Dindo classification, grade 3 or 4 defined as severe complication) (13), and pathology results. Preoperative DTPA scintigraphy was performed not earlier than 3 months before surgery and postoperative renal function was measured 3 months after surgery. Subsequent DTPA scintigraphy was generally performed annually.
All RAPNs were performed with the da Vinci Surgical System using a transperitoneal approach and the 4-arm technique. The camera port was placed 6 cm above the umbilicus at the lateral position and the assistant 12 mm port was placed near the cranial side of the umbilicus. Three 8 mm working ports were located on the side of the abdomen undergoing surgery. Only the renal artery was clamped with bulldog clamps, without thermoregulatory manipulation. During the operation, pneumoperitoneum pressure was maintained at 12 mmHg. OPN was performed using a flank and retroperitoneal approach, with the patient mainly in the lateral position. We used the same bulldog clamps for clamping the renal artery and used ice for cooling the kidney during excision of the mass. Clamping time was the time from when the bulldog clamps were applied to the renal artery to the time they were removed, and was reported to the operator every 5 minutes by the scrub nurse. Exposed calyces, bleeding foci, and parenchymal defects were sutured horizontally with hemostats using an interrupted (in RAPN) and continuous (in OPN) suture maneuver. An ultrasound probe was used to determine the cutting plane in patients with endophytic tumor.
Kidney function was evaluated by performing DTPA renal scintigraphy. Patients were maintained on usual hydration and were asked to drink 300–500 mL of water 30 minutes before scanning. After a 1 scout view was obtained, 5 mCi of 99mTc-DTPA was injected, with 80 images captured during the next 20 minutes. If excretion was limited, 80 post voiding images were obtained additionally after micturition. The Gates’ method was used to determinate glomerular filtration rate and the Taylor method was used to correct attenuation. Low energy all-purpose (LEAP) collimator and Syngo MI Apps 2008A program (Siemens, Munich, Germany) were used.
Categorical variables were reported as frequency and proportions, and compared using Student’s t tests. Continuous variables were reported as mean and standard deviation, and compared using Mann-Whitney U tests. All tests were two-sided, with significance defined as P < 0.05. Multivariate regression analysis was performed to identify factors affecting postoperative deterioration of renal function. All statistical analyses were performed using SPSS ver. 18.0 software (IBM Co., Armonk, NY, USA).
RESULTS
Table 1 shows the demographic and clinical characteristics of the initial cohort of 403 patients prior to propensity matching. Of these 403 patients, 114 (28.3%) underwent RAPN and 289 (71.7%) underwent OPN. Patients undergoing RAPN were significantly more likely to have exophytic tumors (P < 0.001) and lower nephrometry scores (P = 0.005). In addition, ischemic time was longer in patients who underwent RAPN (23.9 minutes vs. 19.8 minutes, P < 0.001), but hospital stay was shorter (7.1 days vs. 8.7 days, P < 0.001) and the overall complication rate was lower (21.9% vs. 35.8%, P = 0.004). Histologic type of tumor was similar in the two groups (P = 0.223). Follow-up duration after operation was similar in both groups (34.7 months vs. 35.1 months, P = 0.883) and GFR decline at DTPA was also similar (2.0 mL/min/1.73 m2 vs. 2.4 mL/min/1.73 m2, P = 0.774). In Fig. 1, split renal functions of patient are compared, showing no difference between the two operational methods.
Table 1
Clinical/pathological characteristics of the entire patient cohort

RAPN, robot-assisted partial nephrectomy; OPN, open partial nephrectomy; SD, standard deviation; R.E.N.A.L, radius, exophytic property, nearness to the sinus, anteriority, and location relative to the polar lines of the tumor; RCC, renal cell carcinoma; GFR, glomerular filtration rate; DTPA, diethylenetriaminepentaacetic acid.
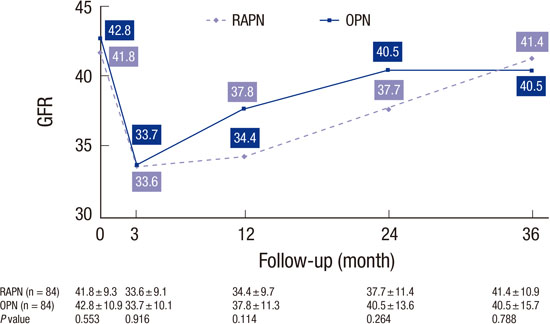
The demographic and clinical characteristics of the matched cohort are shown in Table 2. Unlike before matching, there were no significant group differences in the rates of exophytic tumors (P = 0.818) or nephrometry scores (P = 0.527). The propensity matched RAPN and OPN groups were similar in age, mass size, preoperative GFR of solitary renal units (41.8 mL/min/1.73 m2 vs. 42.8 mL/min/1.73 m2, P = 0.553), and renal function impairment (1.9 mL/min/1.73 m2 vs. 1.5 mL/min/1.73 m2, P = 0.806). Renal ischemic time (24.4 minutes vs. 17.8 minutes, P < 0.001) and operation time (216.9 minutes vs. 196.9 minutes, P < 0.001) were significantly longer in the RAPN group, but the hospital stay was overall significantly shorter (7.1 days vs. 8.4 days, P < 0.001) in the RAPN group. Complication rates did not differ significantly between the two groups (14.3% vs. 23.8%, P = 0.116). In the RAPN group, two patients required transfusion and one required angioembolization. In the OPN group, six patients required transfusion, one experienced wound dehiscence, and one required angioembolization. The RAPN group showed similar split renal function (33.6 mL/min/1.73 m2 vs. 33.7 mL/min/1.73 m2, P = 0.916) at 3 months and low split renal function at 1 year (34.4 mL/min/1.73 m2 vs. 37.8 mL/min/1.73 m2, P = 0.114) and 2 years (37.7 mL/min/1.73 m2 vs. 40.5 mL/min/1.73 m2, P = 0.264) after the operation, but showed no significant difference compared with OPN (Fig. 2). At 3 years after PN, both groups showed similar split renal function again (41.4 mL/min/1.73 m2 vs. 40.5 mL/min/1.73 m2, P = 0.788).
Table 2
Clinical/pathological characteristics of the two groups following propensity score matching

RAPN, robot-assisted partial nephrectomy; OPN, open partial nephrectomy; SD, standard deviation; R.E.N.A.L, radius, exophytic property, nearness to the sinus, anteriority, and location relative to the polar lines of the tumor; RCC, renal cell carcinoma; GFR, glomerular filtration rate; DTPA, diethylenetriaminepentaacetic acid.
Factors affecting the change in GFR were analyzed by univariate and multivariable analysis (Table 3). Univariate analysis of patient characteristics showed that preoperative renal unit function (β = -0.21, P = 0.014), and nephrometry score (β = -1.16, P = 0.025) correlated with postoperative renal function impairment. Multivariate analysis showed that greater preoperative renal unit function (β = -0.24, P = 0.011) and nephrometry score (β = -1.14, P = 0.041) were correlated with reduced GFR.
Table 3
Multivariate analysis for predictive factors of GFR reduction after partial nephrectomy
GFR, glomerular filtration rate; CI, confidence interval; DTPA, diethylenetriaminepentaacetic acid; R.E.N.A.L, radius, exophytic property, nearness to the sinus, anteriority, and location relative to the polar lines of the tumor; RAPN, robot assisted partial nephrectomy; OPN, open partial nephrectomy.
DISCUSSION
PN is the gold standard for the management of small renal masses, but the surgical method varies. RAPN has now begun to be an alternative option to OPN because robot can offer a three-dimensional view of the operating field and fully flexible wristed-instrument motion, and overcome the learning curve for LPN (14). Several previous studies have compared RAPN with OPN and support the trend of increased use of RAPN (15161718).
However, most of these studies analyzed the functional outcomes using the serum creatinine level, an indicator of total renal function and the Modification of Diet in Renal Disease (MDRD) equation, which is used to calculate estimated GFR, can be affected by age and ethnic group (19). Furthermore, estimated GFR calculated from creatinine level has only a limited role in patients with a GFR > 60 mL/min/1.73 m2 (20), who accounted for 89% of the patients in our cohort.
Studies of split renal function after PN have also been reported, and these can be divided into two groups: studies of patients with a single kidney, and studies using renal scintigraphy such as mercaptoacetyltriglycine (MAG3) or DTPA scintigraphy. The former studies included many variations of nephron conserving operations, such as OPN (21), LPN (22), and RAPN (23), and proved that PN was feasible in single kidney patients. However, these studies failed to analyze the impact of the surgical method on functional outcome. In addition, there is a tendency to apply more lenient indications to prevent the complete loss of renal function and dialysis (23), these studies revealed a relatively long renal ischemic time compared with that of the typical population, including the population reported in the present study. Furthermore, the function of the contralateral kidney increases to compensate for PN (24), which is something that cannot occur in solitary kidney patients. Therefore, it is hard to apply these studies to RCC patients with normal contralateral kidney.
MAG3 renal scintigraphy has also been used to analyze solitary renal function after PN in several studies (25262728), but revealed similar issues to those found in single kidney studies, such as lack of analysis of the operational method. MAG3, the most widely-used method in current practice, has several distinctive advantages over DTPA, especially for neonates and patients with suspected urinary obstruction. However, because the results are shown as relative values, operated kidney function could be affected by contralateral kidney function. For example, deterioration of renal function of the contralateral kidney due to renal stone may result in overestimation of operated-side renal function.
In this study, we not only analyzed the impact of the surgical method on functional outcomes using DTPA renal scintigraphy, but also analyzed other factors that can affect renal function (Table 3). As shown by several studies, greater preoperative GFR and nephrometry scores show significant correlation with deterioration of renal function (293031); however, the fact that there is no relationship between functional outcome and ischemic time can be difficult to understand at first glance. In fact, there was a significant difference in ischemic time between the RAPN cohort and the OPN cohort after propensity matching (Table 2). To fully address this issue, several studies have reported that irreversible renal damage to the healthy contralateral kidney may be avoided by limiting ischemia time to less than 30 or 40 minutes (323334), and 16.7% of patients who underwent RAPN had ischemia times longer than 30 minutes. Other studies have also argued that ischemia time has less of an effect on renal function over the long-term, although this opinion is controversial (293035). Thus, we interpret our data to indicate that the longer ischemia times of RAPN patients could have created a tendency toward lower renal function at 1 year and 2 years after surgery, but that renal function recovered at 3 years after the operation.
This study had several limitations. First, it was not a randomized controlled trial; however we matched patients by propensity score matching to minimize bias. Second, the potential effects of the RAPN learning curve should not be ignored. Although all operations were performed by a single surgeon, the proficiency of the surgeon in the two methods differed at the beginning of the study. However, the change in GFR between RAPN patients in the first half of the study and those in the second half was similar. Furthermore, the results of this study may help alleviate the hesitation surgeons might have in performing robotic surgery. Finally, the average follow-up period of patients was 3 years but about half of the patients had shorter follow-up period than 3 years.
In conclusion, long term postoperative reduction in operated renal function was similar between patients who underwent RAPN and those who underwent OPN, even when DTPA renal scintigraphy was used to determine GFR. RAPN showed similar functional outcome, despite its relatively longer ischemic time. Studies with larger groups are warranted to confirm results of the present study.
 XML Download
XML Download