

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hepatitis A virus (HAV) is one of the most common causes of acute hepatitis in the world, with 1.5 million cases each year (1). The disease prevalence of HAV is closely related to socioeconomic status and sanitation (123). Socioeconomic improvements and better sanitation have resulted in fewer children with long-term immunity through early-life exposure to non-immune status (45). High-income regions of the world, including the Republic of Korea, have very low HAV endemicity levels and a high proportion of susceptible adolescents and adults (6). In Korea, the seroprevalence of anti-HAV antibody, a marker of endemicity, was 11.7%-13.0% in individuals 15-29 yr of age, which have resulted in several outbreaks of hepatitis A among this age group (3789). Since HAV infection is usually asymptomatic in young children and the likelihood and severity of symptoms tends to increase with age from the late teens to twenties (1234578), prevention through vaccination programs is important for HAV control in these regions.
The first inactivated hepatitis A vaccine (HepA) was developed in 1992 (10) and there are currently several inactivated vaccines available worldwide, including Vaqta® (Merck & Co. Inc., West Point, PA, USA), Havrix® (GSK Biologicals, Rixensart, Belgium), Avaxim™ (Sanofi Pasteur, Lyon, France), and Epaxal® (Crucell Vaccines Inc., Leiden, the Netherlands) (2411). All of these vaccines have similar properties, are well-tolerated, are highly immunogenic, and offer effective protection (21213). However, to the best of our knowledge, there have been no comparative studies on the immunogenicity and safety of more than two types of HepAs. This study was performed to compare the immunogenicity of three different types of HepAs in adolescents with the recommended two-dose program. In addition, the persistence of immunogenicity prior to the second vaccination and the safety profiles of the vaccines were studied.
MATERIALS AND METHODS
Study design and participants
A comparative, open-label, randomized trial (NCT00483470) was conducted from May 2012 to October 2013 at Ewha Womans University Mokdong Hospital in Seoul, Korea. Healthy adolescents 13 to 19 yr of age were considered for inclusion. Participants were excluded if they met any of the following criteria: seropositive for anti-HAV antibodies; hypersensitivity to any vaccine component; previous vaccination with HepA; thrombocytopenia or other coagulation disorder; known or suspected immunological impairment; the administration of immunoglobulin or other blood products within 3-11 months, or the administration of immunosuppressive therapy within 30 days; a history of anaphylactic reaction to any vaccine; a history of a previous HAV infection; a current febrile illness (axillary temperature >37.5℃) or other acute illnesses.
Participants were randomly assigned to 1 of 3 treatment groups following a randomization sequence created using Stata 10.0 (StataCorp, College Station, TX, USA) statistical software with a 1:1:1 allocation using random block sizes of 3, 6, and 9.
Blood samples for anti-HAV antibody were obtained at each visit: enrollment (visit 1), one month after the first dose (visit 2), just prior to the second dose (6 to 12 months after the first dose; visit 3), and one month following the second dose (visit 4). Serum samples were stored at -70℃ until analyzed.
Vaccines and vaccination
Avaxim™ is a formaldehyde-inactivated liquid HepA adsorbed onto aluminum hydroxide (14). Avaxim™ 80U (Avaxim™ 80U pediatric) is designed for children aged 12 months to 15 yr while Avaxim™ 160U is designed for those above the age of 16 yr. Epaxal® is a formalin-inactivated liquid vaccine, which is attached to the virosomes (1516). Epaxal® 0.25 mL (Epaxal® junior) is for children aged 12 months to 16 yr and Epaxal® 0.5 mL is for those above 17 yr of age. Havrix® is formaldehyde-inactivated liquid vaccine adsorbed onto aluminum hydroxide (10). Havrix® 720 (Havrix junior) is for children aged 12 months to 18 yr and Havrix® 1440 is for those above 19 yr of age. All vaccines were stored at 2 to 8℃ until the time of vaccination.
Subjects were randomized to receive equal amounts of one of the three vaccine groups (Fig. 1). Each group received two doses of Avaxim™ (Vaccine A), Epaxal® (Vaccine B), or Havrix® (Vaccine C) 6 to 12 months apart (The mean duration of the interval between the first and second dose was 11.7±1.0 months). Subjects received either a pediatric dose (Avaxim™ 80U, Epaxal® 0.25, or Havrix® 720) or an adult dose (Avaxim™ 160U, Epaxal® 0.5 mL, or Havrix® 1440) according to their age. The vaccines were administered by intramuscular injection into the deltoid muscle.
Immunogenicity assessment
Total serum anti-HAV antibody levels were determined using an electrochemiluminescence immunoassay (Cobas 8000 e602, Roche, Mannheim, Germany) in the Seegene Medical Foundation, Seoul, Korea. The detection limit of quantification was 3-60 mIU/mL. Antibody levels >60 mIU/mL were tested again after appropriate dilution of the serum with phosphate buffered saline (PBS).
Seroconversion (or "seroprotection") was defined as achieving an anti-HAV antibody titer ≥20 mIU/mL after vaccination (517). The seroconversion rates of the three vaccine groups at each visit were studied. The geometric mean concentrations (GMCs) of anti-HAV antibody after vaccination were compared between the three vaccine groups. GMCs were also compared in the pediatric and adult dose subgroups, who received 2 doses of the vaccines in pediatric and adult doses, respectively.
Reactogenicity and safety assessment
All parents/guardians were provided with a digital thermometer and a diary card containing a list of adverse events and their grades, as well as instructions for recording concomitant medications, the use of any antipyretic agents, axillary temperatures, and details of local and systemic reactions/symptoms that might occur during the 5 days following each vaccination. Each subject was observed for a period of 30 min after vaccination to detect any immediate local and/or systemic reactions. Local (pain, redness, swelling at the injection site) and systemic (fever, headache, dizziness, myalgia, gastrointestinal disorders, poor oral intake, and irritability) events were recorded by parents/guardians on the diary cards for 5 days (Days 0-4) following each vaccine dose. Unsolicited adverse events (AEs) for one month (Days 0-30) following each vaccination as well as serious adverse events (SAEs) throughout the study periods were monitored.
The intensity of each symptom was graded on a scale from 0 to 3, ("0" signifies no symptoms; "1" signifies mild symptoms, without trouble in daily activities; "2" signifies moderate symptoms, with some trouble in daily activities; and "3" signifies severe symptoms, with symptoms preventing normal daily activity). Injection site reactions were considered related to the vaccination, while the causal relationship between all other AEs and the vaccination were assessed by investigators based on clinical judgment.
Statistical analysis
The immunogenicity analysis was per-protocol (PP) and only included participants who completed the study vaccine administration and blood collections as scheduled. The safety analysis was modified intention-to-treat (ITT) and included all subjects with at least one dose of vaccine for which safety data were available. A sample size of 50 subjects from each group was needed to estimate the seroconversion rate following the first dose of each vaccine with 95% confidence within a margin of error of 8% (based on the assumption of an estimated rate of 92% seroconversion). Antibody responses were assessed by calculating the GMCs with a 95% CI and seroconversion rates at visits 2, 3, and 4. Serum samples with total HAV antibody levels <3 mIU/mL were assigned a value of 1.5 mIU/mL for analysis purposes. The GMCs of each vaccine group at each visit were compared using analysis of variance (ANOVA) with the Bonferroni correction or the Student t-test. Differences in the proportions of patients with adverse events were compared using a chi-square test or Fisher's exact test with the Bonferroni adjustment. Reverse cumulative distribution curves (RCDCs) for anti-HAV antibody concentrations were constructed to illustrate the immune responses in the three vaccine groups at each visit. Statistical analysis was conducted using SPSS statistical software (version 18.0; SPSS Inc., Chicago, IL, USA).
Ethics statement
The study protocol was reviewed and approved by the institutional review board of the Ewha Womans University Mokdong Hospital (IRB No. 12-07B-07). The study was conducted in accordance with good clinical practices (national regulations and ICH E6) and the principles of the Helsinki Declaration. Written and informed consent was obtained from all subjects and their parents/legal guardians following a detailed explanation of the study.
RESULTS
Study population
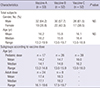
A total of 157 participants were randomized into three groups (53 in the Vaccine A [Avaxim™] group, 52 in the Vaccine B [Epaxal®] group, and 52 in the Vaccine C [Havrix®] group). The demographic characteristics of the subjects in each group are shown in Table 1. Among the total participants, 15 were excluded due to study ineligibility. A total of 136 subjects were in the population evaluated for immunogenicity (50 in the Vaccine A group [17 pediatric/pediatric dose recipients, 9 pediatric/adult dose recipients, and 24 adult/adult dose recipients], 43 in the Vaccine B group [26 pediatric/pediatric dose recipients, 9 pediatric/adult dose recipients, and 8 adult/adult dose recipients], and 43 in the Vaccine C group [39 pediatric/pediatric dose recipients, 4 pediatric/adult dose recipients]) (Fig. 1). A total of 141 subjects (51 in the Vaccine A group, 47 in the Vaccine B group, and 44 in the Vaccine C group) were included in the safety population for the first vaccination, 138 subjects (50 in the Vaccine A group, 45 in the Vaccine B group, and 43 in the Vaccine C group) were included in the safety population for the second vaccination.
Immunogenicity
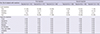
The anti-HAV GMC levels and seroconversion rates of the three groups at each visit are summarized in Table 2. At visit 2 (one month after the first dose of vaccine), the seroconversion rates of the Vaccine A, Vaccine B, and Vaccine C groups were 98%, 95%, and 93%, respectively, differences that were not statistically significant. At visit 3 (6 to 12 months after the first dose), all subjects in all three groups showed 100% seroprotection, which was maintained to visit 4 (one month after the second dose of vaccine).
Fig. 2 shows a comparison of the immunogenicity of the three HepAs at each visit. At visits 2, 3, and 4, anti-HAV GMCs were significantly higher in the Vaccine A group than in the Vaccine B group (visits 2, 3, and 4: P<0.001, P=0.001, and P<0.001, respectively) and the Vaccine C groups (visits 2, 3, and 4: P<0.001, P<0.001, and P<0.001, respectively). In the pediatric dose subgroups, anti-HAV GMCs were also significantly higher in the Vaccine A subgroup than in the other subgroups at Visit 2 (Vaccine A subgroup vs. Vaccine B subgroup: P=0.018, Vaccine A subgroup vs. Vaccine C subgroup: P=0.003) and Visit 4 (Vaccine A subgroup vs. Vaccine B subgroup: P<0.001, Vaccine A subgroup vs. Vaccine C subgroup: P<0.001). In the adult dose subgroups, anti-HAV GMC was significantly higher in the Vaccine A subgroup than in the Vaccine B subgroup at Visit 4 (P=0.001). Analyses in the adult dose subgroups were performed only between the Vaccine A and Vaccine B subgroups since there were no subjects who received 2 adult doses of vaccine in the Vaccine C group.
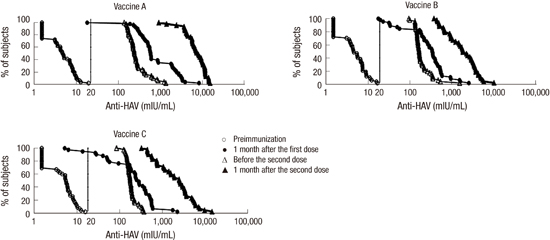
The RCDCs in Fig. 3 show that the curves after the first and second doses of vaccination shifted to the right compared to those before each vaccination in all three vaccine groups. This distribution indicated that the anti-HAV concentration increased with repeated vaccination.
Reactogenicity and safety
No subjects in any of the groups had immediate AEs in the 30 min after vaccination or vaccine-related SAEs after each vaccination. Local and systemic AEs after immunization are shown in Table 3. The three vaccines were well-tolerated, with a similar incidence and type of post-vaccination reactions, with the exception of a higher frequency of redness and swelling after the second injection (P=0.018 and P=0.027, respectively) in the Vaccine B group as compared with the Vaccine A group. Pain was the most common AE in all vaccine groups. Local and systemic AEs were mostly mild-to-moderate in intensity and resolved within 5 days. All reported AEs resolved without complications and there were no study withdrawals due to adverse events or deaths during the study period.
DISCUSSION
This study demonstrated that the three HepAs showed good immunogenic responses and were well-tolerated in adolescents, but that there may be different quantitative immune responses depending on the type of vaccine. To the best of our knowledge, this is the first study comparing the immunogenicity and safety of three types of HepAs. Previous studies (41618192021), which mostly compared two vaccine groups, reported that the vaccines that were studied were immunogenic and safe. In accordance with previous studies, our results showed that the seroprotection rates were ≥90% one month after the first dose and 100% after the second dose in all vaccine groups. Moreover, the seroprotective antibody levels were maintained throughout the study period.
Despite good immunogenic responses in all study vaccines, there seemed to be kinetic differences in antibody production after vaccination based on the type of vaccine. In our results, anti-HAV GMCs were significantly higher in the Avaxim™ group than in the other two groups at all visits after vaccination. Similar tendencies were also noted in the GMCs of both the pediatric and adult dose subgroups. These results are in agreement with those of previous studies (2223), which reported that the antibody concentrations in response to Avaxim™ were higher than with other target vaccines. Conflicting results have been reported in several studies that have compared the immunogenicity of Epaxal® and Havrix® in children. Epaxal® 0.25 showed superior immunogenicity than Havrix® 720 in some studies (2425), although the converse has been demonstrated in other studies (16). In our study, the anti-HAV GMCs of the Epaxal® and Havrix® vaccine groups (both the overall group and the pediatric dose subgroup) were comparable, with no statistical differences. Unfortunately, there have been few studies that have compared the immunogenicity between Avaxim™ and Epaxal® in either pediatric or adult doses; hence it was difficult to compare our results with those of previous studies.
With respect to safety, all three vaccines showed very good safety in the present study. Solicited local and systemic reactions were mostly mild and transient. Injection site pain was the most common symptom, similar to what has been reported by other investigators (241618). Although redness and swelling at the injection site were reported significantly more frequently in the Epaxal® group as compared with the Avaxim™ group after the booster vaccination in our study, there were no statistically significant differences in the other solicited AEs among the three vaccine groups. In previous studies, despite subtle differences in the AEs between different vaccines, the study vaccines overall were well-tolerated. One previous study reported that injection site pain tended to occur more frequently and with greater intensity in subjects vaccinated with the alum-absorbed vaccine (24). However, our results indicated that the pain reaction in all vaccines were similar in incidence, without significant differences based on the type of adjuvant. This suggests that local reactions, including pain, are not significantly related to the adsorbents in the vaccines.
In recent seroepidemiologic data of hepatitis A in Korea (7), there has been a significant change in the seroprevalence patterns over the past 30 yr. The most susceptible group has shifted from children less than 10 yr of age to individuals 10-29 yr of age. These changes are related with improvements in hygiene and the introduction of HepA. However, these seroprevalence patterns also reflect the possibility of disease outbreak in individuals 10-29 yr of age, so prevention through the vaccination of adolescents should be emphasized. Our results support the recommendation of administering HepA in adolescents to prevent hepatitis A, which can result in serious morbidity in this age group.
This study has several limitations. First, there were a limited number of subjects per study vaccine. Therefore, we should be careful in interpreting the results. Second, all of the subjects were Korean, so possible racial/ethnic factors in the immune response to the vaccines should be considered when interpreting these study results. Despite these shortcomings, our data should aid in the understanding of the immunogenicity and safety of HepAs in adolescents.
In conclusion, the three HepAs studied were highly immunogenic and well-tolerated in adolescents, although there may be differences in the kinetics of antibody production after immunization depending on the type of vaccine used. Thus, they can be recommended for routine vaccination in countries with a high proportion of susceptible adolescents, including Korea.




 XML Download
XML Download