

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Childbearing is an important issue in women with systemic lupus erythematosus (SLE), as the disease predominantly affects women in their reproductive years. Although the outcome of SLE pregnancy has been improved over the past few decades (12), childbearing is still a significant burden for women with SLE. Maternal mortality is 20-folds higher in women with SLE, and they are also at high risk of developing serious medical and obstetric complications during pregnancy (3456). Childbearing may be compromised by several factors in women with SLE. Disease-related factors such as active disease, lupus nephritis, high dose corticosteroid therapy, and previous use of cyclophosphamide are well known factors associated with poor pregnancy outcomes and decreased fertility compromising childbearing in SLE patients (7891011). In addition to disease-related factors, childbearing may be interrupted by the personal decisions not to have children. However, there is a paucity of data regarding decisions affecting childbearing in women with SLE. Only one previous study from the United States analyzed the effects of childbearing decisions on family size of women with SLE (12). This study delineated that concerns about child health and personal welfare resulted in smaller family size among SLE women.
Decisions on childbearing can be influenced by a myriad of demographic, social and health related factors (13). Therefore, the society women belong to may significantly influence women’s decision on childbearing. Studies from different regions of the world would help physicians to better guide and manage SLE patients with different social background who wish to have children and experience the enjoyment of family life. The purpose of our study was to investigate the influence of personal decisions on family size of Korean patients with SLE, and factors that affect the decisions. To the best of our knowledge, this is the first study investigating the impact of childbearing decisions on family size in the ethnically homogenous population of Korean women with SLE.
MATERIALS AND METHODS
Subjects
All female patients attending the rheumatology clinic of 6 tertiary hospitals participating in the Network for Lupus Clinical Research in South Korea who fulfilled 1997 American College of Rheumatology criteria for SLE (14) were invited to participate in this case-control study. Participating hospitals were located throughout Korea including Seoul, Gyeonggi-do, Gyeongsang-do, and Jeolla-do regions including both urban and rural areas. Patients were eligible for the study if they were women between ages of 18-45, who are/were married or living with a partner. One hundred twelve patients were recruited between February 2010 and April 2012. During the same period, 135 age-matched healthy women who are/were married or living with a partner who visited the participating hospital for routine obstetric checkup were recruited for controls.
Data collection
Socio-demographics and clinical data regarding SLE disease history and laboratory data were collected through a survey using a standardized questionnaire and medical record review. We obtained demographic information including age, marital status, educational attainment, occupation, income, tobacco smoking, alcohol consumption, area of residence and the number of pregnancies and live births from medical record review. Women’s and husband’s family size and reproductive and gynecologic history, including menstruation history, past gynecologic problems, sexual interest, and use of contraceptives were obtained using the questionnaire. Childbearing decisions, whether they decided to have or not to have children were questioned, and if they had made a decision on childbearing, the reasons for making such decision, and also who was the most influential person in making such a decision were also questioned.
Statistical analysis
All continuous parameters were checked by the Shapiro-Wilk test for normality and presented accordingly. Normally distributed data were presented as means ± standard deviation, and not normally distributed data as median with inter-quartile range to describe socio-demographics and the childbearing histories. To compare the characteristics between SLE groups with healthy controls, Student’s t-test was used if normally distributed, and Mann-Whitney test otherwise. For categorical variables, chi-square test was used. To ascertain the effect of SLE diagnosis on pregnancies, we compared the number of pregnancies and live births before and after diagnosis using analysis with the Kruskal-Wallis test. The impact of socio-demographic factors affecting childbearing decisions was determined using a multivariate logistic regression. Statistical analyses were performed using SAS software (version 8.2; SAS Institute, Cary, NC, USA), and a two-tailed P-values < 0.05 were considered statistically significant.
RESULTS
Characteristics of the study subjects
SLE patients and healthy controls were all ethnically Koreans and demographically similar coming from both urban and rural areas. Socio-demographics and clinical characteristics of study subjects are presented in Table 1. At the time of study, the median age of SLE subjects were one year higher than that of controls (37 versus [vs] 36, P < 0.001). SLE patients had lower educational levels and family income and higher rates of smoking compared with controls. Of note, women with SLE came from smaller families compared with the controls. SLE patients had the median disease duration of 6 years. In about half of the patients, SLE was diagnosed before childbearing was finished.
Table 1
Characteristics of the subjects

Values are given as number (%) of subjects, unless otherwise indicated; SLE, systemic lupus erythematosus; IQR, inter-quartile range.
![]()
Menstrual, sexual, and gynecologic history was also assessed and compared between SLE women and healthy controls (Table 2). Menstrual abnormalities were significantly more common in SLE patients compared with the controls (38.3% vs. 9.0%, P < 0.001), accounting for more than one-third of the patients. In addition, more women with SLE reported decreased sexual interest compared with controls (43.8% vs. 30.6%, P = 0.035). There was no difference between the two groups in relation to history regarding menopause, infertility treatment, hysterectomy, oophorectomy, and sexually transmitted disease. Of note, use of contraceptive methods was lower in lupus women than in controls (41.0% vs. 56.7%, P = 0.016).
Table 2
History related to reproductive health

Values are given as number (%) of subjects, unless otherwise indicated; SLE, systemic lupus erythematosus.
![]()
Childbearing history and family size
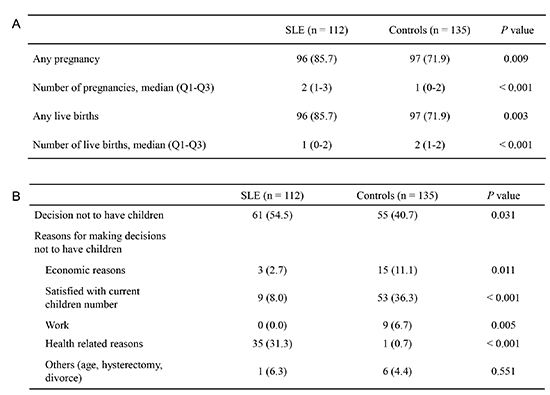
More women with SLE reported at least one pregnancy (85.7% vs. 71.9%, P = 0.009) and at least one live birth (85.7% vs. 71.9%, P = 0.003) compared with controls (Table 3). Although women with SLE had a significantly higher median number of pregnancies (2 vs. 1, P < 0.001), median number of live births was significantly lower in women with SLE (1 vs. 2, P < 0.001). When childbearing history in relation to the time of SLE diagnosis was assessed, women diagnosed with SLE before the first child was born had significantly fewer pregnancies (P = 0.035) and children (P < 0.001) than women diagnosed after the last child was born, suggesting that the disease bearing had a significant impact on childbearing in SLE patients (data not shown).
Table 3
Childbearing history and family size

Values are given as number (%) of subjects, unless otherwise indicated; SLE, systemic lupus erythematosus; Q, quartile.
![]()
Childbearing decisions and factors influencing the decisions
When questions about childbearing decisions were inquired, significantly more women with SLE made decision not to have children compared with controls (54.5% vs. 40.7%, P = 0.031). However, there was no significant difference among SLE women with and without lupus nephritis who made the decision not to have children (data not shown). Among the SLE group, health-related reasons primarily affected their decision not to have children, whereas satisfaction with current children number was a major cause of the decision among the controls (Table 4).
Table 4
Childbearing decisions
Values are given as number (%) of subjects, unless otherwise indicated; SLE, systemic lupus erythematosus.
![]()
Next, we examined socio-demographic and reproductive health related factors which might influence women's decisions to avoid childbearing in patients with SLE (Table 5). In univariate analysis, women coming from larger family size were less likely to make the decision not to have children in SLE women. However, after adjusting for socio-demographics (age, education, income, family size, smoking, drinking, and presence of influential person) and gynecologic characteristics (sexual interest and menstruation pattern) in a multivariate analysis, socio-demographic and reproductive health related factors commonly influencing the decision to limit childbearing did not influence the decision in SLE women. Among controls, large family size and alcohol drinking were significantly related with the intension to limit childbearing (data not shown).
Table 5
Socio-demographic and reproductive health related factors influencing decisions not to have children in patients with SLE
Values shown are odds ratio (OR) and 95% confidence interval (CI); SLE, systemic lupus erythematosus.
*Adjusted for age, education, income, and family size, smoking, drinking, presence of influential person, sexual interest and menstruation pattern.
![]()
DISCUSSION
In this study, we observed that Korean women with SLE have substantially smaller family size compared with the healthy controls, and the disease had a significant impact on the family size. In addition, approximately half of women with SLE made a decision not to have children because of the health-related concerns, and this also contributed significantly to smaller family size in SLE women.
Women with SLE were reported to have fewer children on average than the normal population (151617). In a population-based study, a lower mean number of births was observed in women with connective tissue diseases including SLE, compared with healthy controls (1.7 vs. 2.2) (15). Approximately 20% of pregnancies in women with SLE will end in a miscarriage, compared with 9% in the general population (1218). The risk of stillbirth has also been shown to be elevated with more than 3-fold increase compared with the general population (1920) Women with SLE are at greater risk of pregnancy loss, and the excess risk exists both before and after diagnosis of SLE (34521). However, live births were substantially lower after SLE diagnosis, suggesting that the disease have significant impact on family size (16). These findings are similar to that observed in the present study. The average number of live births was lower in our lupus women than in controls (1.2 vs. 1.6). Women diagnosed with SLE prior to the birth of their first child had significantly fewer pregnancies and children than women diagnosed after the last child was born. It was reported that non-white women with SLE tend to retain propensity to have more than two children, but we found that Korean women with SLE had less than two children as in white women with SLE (18). This may be related to low birth rate in Korea. According to 2012 statistics, birth rate was 1.3 for every Korean woman (22).
Although fertility might be impaired in women with SLE by several factors such as immunological pathophysiology, autoantibodies, disease activity, therapies or hormonal dysfunction, women with SLE appear to have normal rates of fertility (19232425). In a case-control study, 77% of SLE women and 69% of controls had at least one pregnancy (2). Mean numbers of pregnancies reported were between 2.0 to 2.6 comparable to normal population (215). Similarly, the majority (85.7%) of our women with SLE reported at least one pregnancy, and the mean number of pregnancies was 2.4 in accordance with previous studies, although menstrual irregularities and decreased sexual interest were common problems among our women with SLE. However, we found that the mean number of pregnancies was significantly higher in Korean women with SLE than in controls (2.4 vs. 1.4, P < 0.001). This may be related to lower rate of contraceptive use among lupus women than controls found in our study as others (26). Given the risks associated with pregnancies in patients with SLE, contraception counselling should be more actively employed by the rheumatologists in Korea.
Multiple factors are known to limit the number of children born to women with SLE. Disease-related factors such as hypertension, the presence of antiphospholipid antibodies or anti-Ro antibodies, active lupus nephritis and high disease activity have been recognized as risk factors for pregnancy loss in SLE patients (2027). Among these factors, fetal prognosis depends strongly on disease activity (2). Moderate to severe lupus activity during pregnancy leads to a decrease in live births, with almost one-quarter of these pregnancies resulting in fetal loss (7). Prior hospitalization for SLE is also associated with decreased live births, suggesting that active disease increases the risk of fetal loss (16). Disease-related factors affecting pregnancy outcomes in Korean patients with SLE are not different from those reported previously. In agreement with previous studies, presence of antiphospholipid antibodies, lupus nephritis, and active disease were associated with adverse pregnancy outcomes in Korean patient with SLE (61011).
Apart from disease-related factors, the decisions not to have children may also contribute to lower birth rates in women with SLE. A prior study has demonstrated that of women interested in having children, 55% with RA and 64% with SLE had fewer children than originally desired (12). Concerns about child health and personal welfare significantly contributed to their decisions not to have children. Disease-related concerns included concerns in regards to the practical and physical limitations imposed by the disease, side effects of the medications they are on, genetic risks of transmitting the disease to the offspring, and child health and care concerns. Similar observations were reported in RA patients (28). Women’s choices to limit family sizes influenced lower birth rate among women with RA. We also found that significantly more women with SLE made decisions not to have children compared with the controls (54.5% vs. 40.7%), and disease-related concerns mainly affected their decision. Above this, various socio-behavioral factors such as race/ethnicity, marital status, income, education, and family background could influence the childbearing decisions. White women with SLE were reported to have fewer children than controls, whereas non-white lupus women showed a tendency to have larger families (18). In another study of lupus women, Black race/ethnicity and being married or living common-law were associated with increased live births, whereas Asian women had relative decreased live births versus the general population (17). In our study, conventional socio-demographic factors such as income, education, family size, smoking, and drinking did not have any influence on childbearing decisions in our women with SLE. Among controls, smaller woman’s family size and alcohol drinking were related with the intension to limit childbearing. Despite lower income of lupus women, however, economic reasons did not influence their decision not to have children.
Our study suggests that disease-related concerns rather than socio-behavioral factors may primarily affect the decision to limit family size in Korean women with SLE. Interrupted childbearing or involuntary childlessness is a traumatic event for women and can be a cause of severe emotional distress which persists for a long period of time. A recent analysis of large population-based National Survey of Fertility Barriers confirms that women who are involuntarily childless have higher rates of depression and lower life satisfaction than women who have not experienced infertility. Women who experienced pregnancy loss and were still childless had the most severe impact on their mental health (29). Similar emotional distress was found among women with interrupted childbearing in long-term female cancer survivors (30). It is also possible that women with SLE who often encounter the disease during reproductive years would experience such emotional distress and interfere with their happiness and fulfillment in life when they involuntarily have fewer children than planned. Since most lupus women and even those with the most disabling rheumatic disease expressed a desire to have children (3132), management of pregnancy in SLE should be optimized to reduce the risk of physical as well as emotional distress.
The present study is has some limitations. One is the lack of detailed clinical data on maternal and fetal complications at the time of conception and during pregnancy. Since this study was a retrospective analysis using data collected via a survey and medical record review, we could not assess SLE disease activity including clinical manifestations and laboratory data. However, focus of our analysis was mainly on analyzing the impact of SLE on family size and childbearing decisions rather than the pregnancy outcomes. Second, recall bias may have influenced the women’s reports of their childbearing decisions. Nonetheless, any such misclassification would be expected to be little since the recall time was relatively short. The main strength of our study lies in the analysis of family size and childbearing decisions among an ethnically homogeneous population of SLE women in Korea, who might have different social values compared with previous studies. This is the first, multicenter, case-control study assessing these issues in Korean women with SLE. Our study showed that disease-related concerns had significant impact on family size of women suffering from SLE. Our study also highlights the importance of pregnancy planning, risk assessment, multidisciplinary and tailored management, and education in women with SLE who desire children.
 XML Download
XML Download