

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Primary Sjögren’s syndrome (pSS) is a systemic autoimmune disease characterized by lymphocytic infiltration of the exocrine glands, which results in dry mouth (xerostomia) and eyes (xerophthalmia) (1). The prevalence of pSS in Korea has not been reported. Worldwide, it varies according to the race and age of the subject population ranging from 0.03%-2.7% (2). The major manifestation of pSS is sicca symptom, but extraglandular manifestations such as interstitial lung disease (3), myelopathy (4), and renal involvement (56) have been reported. Diagnosis of pSS is made according to ECCG criteria (7), or American College of Rheumatology classification criteria (8). Despite advances in the understanding of pathogenesis of the disease, current treatment mainly targets for alleviating sicca symptoms with lack of targeted therapy.
Although oral dryness does not always correlate with systemic disease activity, the degree of xerostomia needs to be determined because it affects the quality of life of patients and can be managed with medications such as pilocarpine. Salivary flow rate (SFR), both resting and stimulated, is commonly determined as an objective tool to evaluate dryness. Nevertheless, only a weak association was observed between subjective dryness and SFR (9). Therefore, xerostomia is often evaluated by using the visual analogue scale (VAS) or questionnaires such as the xerostomia inventory (XI) and sicca symptom inventory.
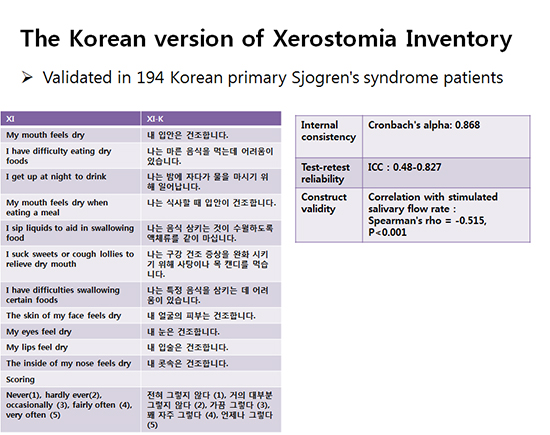
The XI is a set of questions consisting of 11 items that address xerostomia symptoms in daily activities (10). The original English version of the XI was developed by Murray Thompson, an Australian dentist, in order to evaluate oral dryness. It performed well in various populations, including pSS patients (11) and aged populations (10). XI was translated into Spanish (12) and Portuguese (13), and its condensed version was translated into Chinese (14). For establishing a large prospective cohort of pSS in Korea, the XI was translated into Korean and a validation process was carried out.
Here, we describe the process of developing a validated Korean version of the XI (XI-K) to evaluate the degree of xerostomia in pSS patients. For this purpose, the internal consistency and reliability of the questionnaire was evaluated in patients from the Korean pSS registry (Korean Initiative of Sjögren’s Syndrome [KISS]).
MATERIALS AND METHODS
Study population
All of the patients with pSS in this study were participants registered in the KISS registry. The KISS was founded in 2013 with the aims of establishing a nationwide prospective cohort that contains overall clinical data and samples from patients with pSS and developing diagnostic and treatment tools for pSS. All data were collected and managed with the use of the Clinical Research and Trial Management System (Korea National Institutes of Health, Korea Centers for Disease Control and Prevention). Recruitment began in October 2013 in Seoul St. Mary’s Hospital, a tertiary care university hospital and referral center in Seoul, Korea. By July 2015, the database included 224 pSS patients from Seoul St. Mary’s hospital. Patients were diagnosed with pSS according to the American-European Consensus Group criteria for pSS (7) or the 2012 American College of Rheumatology criteria (8). Among the patients, 194 who completed the XI questionnaire were analyzed in this study. Resting SFR was obtained for 166 patients; and stimulated SFR, in 137 patients. Sixty-four patients were asked to answer the XI-K questionnaire again 2 weeks after the first round in order to investigate test-retest reliability.
The XI questionnaire
The XI questionnaire consists of the following 11 items: “My mouth feels dry,” “I have difficulty eating dry foods,” “I get up at night to drink,” “My mouth feels dry when eating a meal,” “I sip liquids to aid in swallowing food,” “I suck sweets or cough lollies to relieve dry mouth,” “I have difficulties swallowing certain foods,” “The skin of my face feels dry,” “My eyes feel dry,” “My lips feel dry,” “The inside of my nose feels dry.” The study participants were asked to indicate which 1 of 5 response options best described their symptoms over the preceding 2 weeks. The response options were “never” (score 1), “hardly ever” (score 2), “occasionally” (score 3), “fairly often” (score 4), or “very often” (score 5). The sum of 11 scale scores makes the final score, which can range from 11 to 55 (Table 1). Higher scores depict greater severity in oral dryness.

Translation into Korean and cultural adaptation
The forward translation into Korean was performed by two independent rheumatologists whose native language was Korean. The two forward translations were compared, and one common version was developed by an expert panel that consisted of three rheumatologists. The common forward translation version was translated back into English by two independent translators whose native language was English. The two back-translations were discussed again by the expert panel and reviewed against the original XI. Finally, the pre-final version of the XI-K was developed (Table 1).
Statistical analyses
Internal consistency
Internal consistency of the XI-K was assessed by calculating Cronbach’s alpha. Inter-item correlations were calculated, and correlations of each item and the total score (item-total correlation) were examined. We also investigated whether Cronbach’s alpha was improved by removal of any item.
Test-retest reliability
After a 2-week interval, each patient was asked to answer the XI-K questionnaire again. Prescribed medications were kept unchanged during the 2 weeks. The procedure was identical to the first administration. The test-retest reliability of the XI-K total score and score for each question was determined by calculating ICCs (model: two-way randomization; type: absolute agreement) and 95% confidence intervals (CI). ICCs were interpreted as follows: ICC < 0.40 = poor reliability; ICC ≥ 0.40 but ≤ 0.75 = fair to good reliability; and ICC > 0.75 = excellent reliability.
Construct validity
To determine the construct validity of the XI-K questionnaire, aspects of the convergent validity were considered. Total XI-K scores were compared with the function of resting, stimulated, and differential (stimulated minus resting) SFRs, and a Spearman correlation analysis was performed.
RESULTS
Translation into Korean
The translation process went well without any difficulties. None of the patients complained of any difficulties in answering the XI-K questionnaire.
Characteristics of the subjects
All of the patients enrolled in our registry were patients with pSS, meeting the 2012 American College of Rheumatology classification or 2002 American-European Consensus Group criteria for pSS. Among the 194 patients, 193 were women, and the median age was 53 (14) years (Table 2). The resting and stimulated SFRs were 0.02 (0.06) and 0.5 (0.9) mL/min, respectively. The median total XI score of the subjects was 36 (13).
Internal consistency
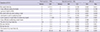
Cronbach’s alpha for the 11 questions was 0.868, showing good internal consistency, as values higher than 0.80 are considered desirable (15). The mean inter-item correlation coefficient was 0.37, and the average item-total correlation coefficient was 0.654. In addition, Cronbach’s alpha was obtained after the item was removed, indicating that internal consistency did not improve significantly even after any item removal (Table 3).
Table 3
Item-total correlations and Cronbach’s alpha when the item was removed

Test-retest reliability
To test the reliability of the inventory, ICC analysis was performed with values obtained at 2-week intervals. The ICC analysis result demonstrated that the test-retest reliability was good, with the ICC ranging from 0.48 to 0.812 (Table 4).
Table 4
Mean scores and standard deviations of both administrations of the XI-K questionnaire and intraclass correlation coefficients
Construct validity
To demonstrate construct validity, the correlation between the total XI-K scores and the resting, stimulated, and differential (stimulated minus resting) SFRs was evaluated. The results showed that Spearman’s rho was −0.447 for resting SFR, −0.515 for stimulated SFR, and −0.482 for differential SFR (P < 0.001; Fig. 1). The construct validity of the XI was originally evaluated by using the single standard question, “How often does your mouth feel dry?”, with the following response options: never, occasionally, frequently, and always (1016). The question was also administered in our study subjects. Spearman’s correlation coefficient was 0.772 (P < 0.001). We also checked the correlation between XI score and simple VAS score for dryness. The results showed that Spearman’s rho was 0.492 (P < 0.001), which showed a moderate positive correlation.
Fig. 1
Spearman’s correlation between the Xerostomia inventory (XI) total scores and salivary flow rate (SFR)s. The correlations between XI total scores and the resting (A), stimulated (B), and differential (stimulated minus resting) (C) SFRs were analyzed. The dotted lines depict 95% confidence intervals.

DISCUSSION
The present study demonstrated the process of developing a Korean version of the XI. The XI-K questionnaire was administered to a well-characterized pSS cohort in Korea and showed excellent reliability in terms of internal consistency, test-retest reliability, and construct validity.
The XI was originally developed to evaluate xerostomia in the Austrian elderly (10). Later, it was applied to patients who received radiotherapy for head and neck cancer (16) and diabetic patients (17). It was also used in pSS patients whose sicca symptoms needed to be evaluated (1118). As mentioned, the Portuguese and Spanish versions of the XI were already developed and validated in pSS populations. We also verified that the performance of the XI was excellent in Korean pSS patients, reflecting the degree of oral dryness appropriately.
To evaluate construct validity, we investigated the correlation between XI score and SFR. We observed only a weak association between the SFRs and subjective symptoms. However, the lack of an objective standard led us to use SFR as standard. Indeed, the SFRs correlated well with the XI total scores. The best correlation was observed with the stimulated SFRs. This may result from the fact that 4 items in the XI deal with hyposalivation during food ingestion, which is more related to stimulated SFR rather than resting SFR. XI total score also correlated well with the original standard question and simple VAS score for dryness, as mentioned. Therefore, the construct validity of XI-K could be considered good. Of note, the negative correlation between the VAS scores for dryness and SFRs was weaker than that between the XI-K scores and SFRs, supporting the appropriateness of using the relatively lengthy XI-K questionnaire rather than the simple VAS of dryness to evaluate subjective severity of xerostomia in pSS patients.
Our study has several limitations. First, not all of the patients answered the second round-questionnaire, and test-retest reliability was tested in a relatively small number of subjects. Second, the subjects in our study only included pSS patients, and whether the tool will work well in non-PSS populations with sicca symptoms remains unclear. On the other hand, the strength of the present study is that our data were based on a relatively large number of pSS subjects enrolled in a prospective cohort.
In conclusion, the Korean version of the XI is a reliable tool to estimate the severity of xerostomia in pSS patients.
 XML Download
XML Download