

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Streptococcus pneumoniae is a major cause of pneumonia, meningitis, and bacteremia, and causing considerable morbidity and mortality (1). S. pneumoniae accounts for more deaths worldwide than any other single pathogen, and the World Health Organization estimates that 1.6 million die of disease due to S. pneumoniae each year (2). S. pneumoniae has a capsular polysaccharide, which is the major virulence factor in invasive pneumococcal disease (IPD). The chemical composition of capsular polysaccharide varies among strains, resulting in the generation of multiple pneumococcal serotypes. Each serotype shows distinct serological and immunological responses (34), and 94 serotypes have been identified to date (56).
The epidemiology of pneumococcal serotypes is constantly changing due to natural fluctuations (6) and the selective pressure from antibiotic and vaccine use (78910). A number of multivalent pneumococcal vaccines have been developed to reduce the burden of disease caused by specific pneumococcal serotypes (1112). In Korea, PCV7 (include serotype 4, 6B, 9V, 14, 18C, 19F, 23F) was licensed for use in infants in November 2003, and PCV10 (include PCV7 serotypes plus serotype 1, 5, 7F) and PCV13 (include PCV10 serotypes plus serotype 3, 6A, 19A) replaced it in March 2010, whereas 23-valent pneumococcal polysaccharide vaccine (PPSV23) was introduced as a national immunization program for 65 years of age or older since November 2013. Therefore, monitoring of serotype distribution and antibiotic susceptibility is necessary for national strategy for prevention and treatment of IPD (13). The aim of this study was to provide serotype and antibiotic resistance data on invasive pneumococcal isolates from adult patients.
MATERIALS AND METHODS
Isolates
We collected all isolates of S. pneumoniae from blood or cerebrospinal fluid at the Seoul National University Hospital from January 1997 to December 2012. Clinical features of the patients, including demographic characteristics and treatment outcomes, were collected by reviewing the medical records. Primary site of infection was classified according to the patient’s clinical findings; pneumonia was defined as the presence of respiratory symptoms, new infiltrates on chest radiography, and isolation of S. pneumoniae from blood culture; meningitis was defined as the presence of cerebrospinal fluid pleocytosis and isolation of S. pneumoniae from blood or cerebrospinal fluid culture; primary bacteremia was defined as isolation of S. pneumoniae from blood culture without any primary foci of infections.
In Korea, PCV7 was licensed for use in infants in November 2003, and PCV10 and PCV13 replaced it in March 2010. Therefore, the 16-year study period was divided into the three study periods of 1997-2003, 2004-2010, and 2011-2012.
Non-vaccine serotypes were defined as the serotypes that were not included in PCV13 or in PPSV23.
Serotype determination and antibiotic susceptibility testing
Pneumococcal serotype was determined by the Quellung reaction. Pneumococcal capsular anti-sera were obtained from Statens Serum Institute (Copenhagen, Denmark), and the check-board method was used for interpretation of the results.
Minimal inhibitory concentrations (MICs) of antibiotics against all the pneumococcal isolates were determined using E-test strips (AB Biodisk, Solna, Sweden). Antibiotic susceptibility was defined as susceptible, intermediate, and resistant, according to the breakpoints recommended by Clinical and Laboratory Standard Institute (2013) (14); for penicillin, non-susceptible isolates were defined as minimum inhibitory concentration ≥ 0.12 µg/mL for meningitis, and MIC ≥ 4 µg/mL for non-meningitis. For ceftriaxone, non-susceptible isolates were defined as cefotaxime MIC ≥ 1 µg/mL for meningitis, and MIC ≥ 2 µg/mL for non-meningitis.
RESULTS
Baseline characteristics and demographic findings
A total of 331 S. pneumoniae were isolated from blood or cerebrospinal fluid during 1997-2012 at our institution. Among these, 48 isolates were not stored, and 11 isolates were not identified as S. pneumoniae by optochin test. After exclusion of these isolates, a total of 272 isolates from 272 patients with IPD were included in the study. Of these isolates, 98.5% (268/272) were isolated from blood culture, 1.5% (4/272) from cerebrospinal fluid culture.
Of the 272 patients, 24.6% (67/272) were 16-49 years of age, 40.1% (109/272) were 50-64 years of age, and 35.3% (96/272) were 65 years of age or older. Seventy-nine isolates were collected during the study period of 1997-2003, 158 isolates during 2004-2010, and 35 isolates during 2011-2012.
Clinical characteristics of invasive pneumococcal diseases
Clinical characteristics of the 272 patients with IPD are shown in Table 1. The most common primary site of infection was pneumonia (52.6%, 143/272), followed by primary bacteremia (21.3%, 58/272) and meningitis (10.3%, 28/272). Sixty-nine (25.4%) patients died within 30 days after the onset of IPD. Thirty-day all-cause mortality rate was 32.9% in pneumonia, 22.4% in primary bacteremia, and 14.3% in meningitis.
Table 1
Baseline characteristics of 272 patients with invasive pneumococcal diseases
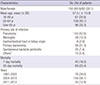
SD, standard deviation.
*Other sites of infection: pyogenic spondylitis, 4; surgical site infection, 3; burn wound infection, 2; brain abscess, 2; sacroilitis, 1; parotitidis, 1; endophthalmitis, 1; toxic epidermal necrolysis wound infection, 1.
![]()
Distribution of pneumococcal serotypes
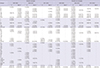
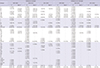
The serotype distribution of 272 invasive pneumococcal isolates is shown in Table 2. Overall, the most common serotype was serotype 19F (8.5%, 23/272), followed by serotype 3 (8.1%, 22/272), and serotype 23F (7.0%, 19/272). The PCV7 serotypes accounted for 36.4% (99/272), the PCV13 serotypes for 60.3% (164/272), the PPSV23 serotypes for 75.4% (205/272), and non-vaccine serotypes for 24.6% (67/272) of the 272 isolates. Serotype 19F was frequently isolated on 50-64 years of age (12/109, 11.0%) and 65 years of age or older (8/96, 8.3%), but relatively scarce in 16-49 years of age (3/67, 4.5%). On the other hand, serotype 23F was more frequent in 16-49 years of age (5/67, 7.5%) and 50-64 years of age (8/109, 7.3%). Of 143 isolates from patients with pneumonia, serotype 14 was the most prevalent, accounting for 9.7% (14/143), followed by serotypes 3 (8.4%, 12/143) and 23F (7.7%, 11/143). Among the 28 isolates from patients with meningitis, serotype 19F was the most common (21.4%, 6/28), and serotypes 3, 6B, and 19A were found in three cases each (Table 3). Among the 69 patients who died within 30 days, serotype 19F accounted for eight (11.6%) cases, serotype 3 for seven (10.1%) cases, and serotype 14 and 35B were found in six (8.7%) cases each.
Table 2
Serotype/serogroup distribution of 272 invasive pneumococcal isolates according to age group and study periods

PCV7, 7-valent pneumococcal conjugate vaccine; PCV13, 13-valent pneumococcal conjugate vaccine; PPSV, 23-valent pneumococcal polysaccharide vaccine; NONT, non-typable; NVT, non-vaccine type.
*Serotypes that were included exclusively in PCV13; †Serotypes included in PCV13; ‡Serotypes that were included exclusively in PPSV23; §Serotypes included in PPSV23.
![]()
Table 3
Distribution of serotype/serogroup of 272 invasive pneumococcal isolates according to primary site of infection and study periods

PCV7, 7-valent pneumococcal conjugate vaccine; PCV13, 13-valent pneumococcal conjugate vaccine; PPSV, 23-valent pneumococcal polysaccharide vaccine; NONT, non-typable; NVT, non-vaccine type.
*Serotypes that were included exclusively in PCV13; †Serotypes included in PCV13; ‡Serotypes that were included exclusively in PPSV23; §Serotypes included in PPSV23.
![]()
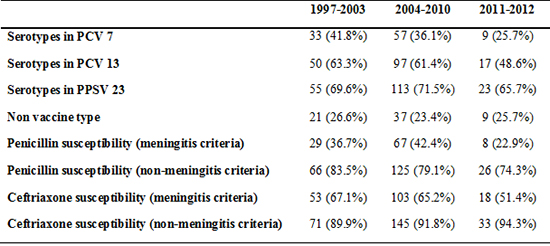
Between the period 1997-2003 and 2004-2010, the proportion of PCV 7 serotypes were decreased but not statistically significant (41.8% vs. 36.1%, P = 0.394). The change of proportion of PCV 7 serotypes were also not significant in each age group. In patients 16-49 years of age, the proportion of the PCV13 serotypes decreased from 60.9% (14/23) in 1997-2003 to 33.3% (2/6) in 2011-2012 (P = 0.342). In contrast, the proportion of non-vaccine serotypes increased from 21.7% (5/23) in 1997-2003, to 50.0% (3/6) in 2011-2012. In patients 50-64 years of age, non-vaccine type was decreased from 34.4% in 1997-2003 to 16.7% in 2011-2012 (P = 0.142), whereas PPSV23 serotypes were increased from 6.3% in 1997-2003 to 33.3% in 2011-2012 (P = 0.027). In patients 65 years of age or older, the proportion of the PCV13 serotypes also decreased from 70.8% (17/24) in 1997-2003, to 52.9% (9/17) in 2011-2012 (P = 0.249). In contrast, the proportion of non-vaccine serotypes was 20.8% (5/24) in 1997-2003, and 23.5% (4/17) in 2011-2012 (P = 0.841) in patients 65 years of age or older. Overall, non-PCV13 serotypes accounted for 39.7% (108/272), and non-vaccine serotypes accounted for 24.6% (67/272).
Antimicrobial susceptibility
Antimicrobial susceptibilities are shown in Table 4. Of the 272 invasive pneumococcal isolates, 79.8% (217/272) were susceptible, 17.6% (48/272) were intermediate, and 2.6% (7/272) were resistant to penicillin by non-meningitis breakpoint, whereas 91.5% (249/272) were susceptible, 7.7% (21/272) were intermediate, and 0.7% (2/272) were resistant to ceftriaxone by non-meningitis breakpoint.
Table 4
Susceptibility to penicillin among 272 invasive pneumococcal isolates according to the serotypes and period of isolation
S, susceptible; Non-S, Non susceptible, PCV7, 7-valent pneumococcal conjugate vaccine; PCV13, 13-valent pneumococcal conjugate vaccine; PPSV, 23-valent pneumococcal polysaccharide vaccine; NONT, non-typable; NVT, non-vaccine type.
*Serotypes included in PCV13; †Serotypes included in PPSV23.
![]()
Of the 108 isolates of non-PCV13 serotypes, 5.6% (6/108) were non-susceptible to penicillin, whereas 0.9% (1/108) was non-susceptible to ceftriaxone by non-meningitis breakpoint.
Penicillin non-susceptible (i.e. resistant plus intermediate) rate was 16.5% (13/79) for the study period of 1997 to 2003, 20.9% (33/158) for the study period of 2004 to 2010, and 25.7% (9/35) for the study period of 2011 to 2012 (P = 0.467). On the other hand, ceftriaxone non-susceptible rate was 10.1% (8/79), 8.2% (13/158), and 5.7% (2/35) for the same study periods, respectively (P = 0.429).
Among the isolates of non-vaccine serotypes, 4.5% were non-susceptible to penicillin, but all were susceptible to ceftriaxone. The proportion of penicillin non-susceptible isolates was over 80% for serotypes 6B, 9V, 14, 19F, 23F, 6A, 19A, 11A, and 35B (Table 5).
Table 5
Susceptibility to ceftriaxone among 272 invasive pneumococcal isolates according to the serotypes and period of isolation
S, susceptible; Non-S, Non susceptible, PCV7, 7-valent pneumococcal conjugate vaccine; PCV13, 13-valent pneumococcal conjugate vaccine; PPSV, 23-valent pneumococcal polysaccharide vaccine; NONT, non-typable; NVT, non-vaccine type.
*Serotypes included in PCV13; †Serotypes included in PPSV23.
![]()
DISCUSSION
We analyzed the serotype distribution of pneumococcal isolates from adult patients with IPD in Korea. The most common serotype was 19F, followed by serotypes 3 and 23F. After the license of PCV7 for use in infants in 2003, proportion of the PCV serotypes decreased in adult patients from 63.3% in 1997-2003 to 48.6% in 2011-2012. As the PCV13 has not been used until recently and PPSV23 immunization rate was low in the elderly in Korea (0.8% and 15.4% in 2010 and 2012 respectively) (1516), and that in children has been increasing from 40.3% in 2005 to 74.3% in 2010 (17), it seems that pneumococcal vaccination in children might result in the changes of serotype distribution in the adult population.
Lee et al. (18) also reported serotype distribution of invasive pneumococci isolated from 1996 to 2008 in Korea. In their study, 116 isolates were collected from patients 65 years of age or older, and the most prevalent serotypes were serotype 3 (16.4%, 19/116), serotype 19F (10.3%, 12/116), and serotype 11A (9.5%, 11/116). They also showed modest decrease in the proportion of the PCV 7 serotypes in patients 65 years of age or older, from 40.9% of the pneumococci isolated in 1996-1999, to 33.3% in 2007-2008.
Our data suggest that serotype distribution may differ among age groups, and it can be influenced by vaccine usage. Following introduction of pneumococcal vaccine, the incidence of S. pneumoniae infection by the vaccine serotypes is expected to decrease. Serotype replacement of nasopharyngeal colonizers after introduction of pneumococcal vaccines has been investigated extensively (19). However, studies on serotype replacement in IPD showed inconsistent results; some studies reported serotype replacement to non-vaccine serotypes (20212223), while others did not (2425). A recent study assessed the influence of PCV7 vaccination in the pediatric population in Korea (26); the frequency of the PCV7 serotypes decreased, while that of the PCV13 serotypes increased, after introduction of the optional use of PCV7 vaccine (10). However, in our study, influence of PCV7 was not shown between period 1997-2003 and 2004-2010. It is probably because that the effect of introduction of certain vaccine is turned up a few years later, due to vaccine coverage rate and difference in direct versus indirect effect in different age group (27). These delay in serotype change according to age group was also shown in other country (28). In the USA, after introduction of PCV13, the incidence of the PCV13 serotypes decreased, while that of non-PCV13 serotypes increased (9). In our study, the proportion of the PCV13 serotypes decreased since introduction of the PCV13 vaccine in patients younger than 50 years of age, whereas this trend was not seen in patients 50 years of age and older. Because PCV13 coverage rate in children is slowly starting increasing after introduction of national immunization program (67% in 2011, 76% in 2012, and 83% in 2013) (29), the changing trend of PCV13 serotype would be changing few years after. Moreover, the frequencies of IPD by the PPSV23 serotypes differed between the two adult age groups. The reason for the differences between the two age groups is unclear.
In our study, 36% of all isolates were non-susceptible to penicillin, whereas 45.7% of the isolates of the PCV13 serotypes were non-susceptible to penicillin. Serotypes 19F, 19A, and 23F, which were frequently isolated, showed higher rate of non-susceptible to penicillin and ceftriaxone than did the other serotypes. This high non-susceptibility in isolates of these serotypes was reported previously in a pediatric (10) and an adult (30) population in Korea. Other studies from Asian countries also showed similar results (313233). The difference in antibiotic resistance rate might be due to the regional difference in the distribution of serotypes. However, same serotypes showed marked difference in antibiotic susceptibility among different countries (34), and therefore differences in serotype distribution itself cannot explain the differences in antibiotic resistance rates. As the serotypes with high rate of non-susceptible to penicillin, such as 19F, 19A and 23F, are prevalent in Korea, pneumococcal vaccination may play an important role in preventing antibiotic-resistant IPD.
Proportions of non-vaccine serotypes were highly variable among studies, ranging from 1.7% to 22.8% (183536373839). Our study showed that non-vaccine serotypes accounted for 24.6% of all invasive isolates. This high proportion of non-vaccine serotypes is in line with the result of a study from Korea, reporting 22.8% (10). Among these non-vaccine serotypes, serotype 15A, 15C, 35B, and serogroup 13/28 were most prevalent, accounting for half of the non-vaccine type isolates, and also showed high rates of antibiotic resistance. In a previous study of an adult population in Korea, serotypes 15A, 13, 15C, and 35B were the most common non-vaccine serotypes (18), and the results were in line with ours. In contrast to high proportion of non-vaccine serotypes in Korea, the proportion of non-PCV13 serotypes was similar to those reported from other countries, such as Japan, Ireland, Spain, and Southeast Asia (3536373839).
There were a few limitations to our study. First, pneumococcal vaccination history was not available for most of our patients. However, because the pneumococcal vaccination rate is very low among Korean adults until 2010 (16), most of them presumably had not been vaccinated against S. pneumoniae. Second, the pneumococcal isolates were collected from a single center, and therefore our results may not be extrapolated to a general population. As our institute is a university-affiliated referral hospital, our study population might include more immunocompromised patients than that in other studies. Third, the third period (2011-2012) was too short to find the variation of serotype change after introduction of PCV13. It needs at least five years to find the changing patterns, if we consider the time lag of PCV introduction and serotype changes. Therefore, further studies should be performed after sufficient periods after introduction of PCV13 to find the effect of this vaccine.
In conclusion, we investigated serotype distribution of invasive pneumococcal isolates from adult patients. Pneumococci with serotypes of the PCV13 showed a decreasing trend over the study period of 1997 to 2012. More than 20% of invasive pneumococci were non-vaccine type. These findings should be considered in future national policy on prevention and control of invasive pneumococcal disease.
 XML Download
XML Download