

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Loss of work due to illness is an important health concern worldwide (1). However, illness is often unavoidable in an occupational setting. Hence, a successful return to work (RTW) after suffering from disease is important for a sustainable working life (2). In Korea, matters regarding the RTW of occupationally injured patients have gained public attention since 2001 and policies to promote the RTW of injured patients began to be established in 2005 (3). Therefore, the RTW rate from occupational injury dramatically increased from 49.9% in 2007 to 70.4% in 2011 (4). However, in Korea, studies on RTW after occupational injury have been limited.
RTW is affected by various factors such as the disease itself and its severity, as well as other physical, psychological, and social factors such as the disability benefit system, labor market conditions, and the employing company (345). These factors have complicated interactions with social support systems including the insurance and health care systems (6). A systematic review found strong evidence that the healthcare system could significantly reduce disability duration and facilitate a RTW (7). Professionals in the healthcare system should play various roles at different points in related social systems. The hospital, including health care professionals, should act as a gateway to the benefits system by providing care, treatment, rehabilitation, and advice to both patients and employers for a successful RTW (8).
The quality aims of hospitals differ between general hospitals and workers’ compensation hospitals (9). For example, rehabilitation of working capabilities is more important in a workers’ compensation hospital, while symptomatic relief of the disease is the more important goal in a general hospital. Furthermore, the main goal of a workers’ compensation hospital is a successful RTW after illness, while that of a general hospital is improvement in a patient’s quality of life. Few studies have investigated whether hospital qualities that focus on workers’ compensation relate to a successful RTW. Hence, we planned to investigate the association between RTW and hospital qualities that focus on workers’ compensation (10).
RTWs from injury are also related to clinical factors, including injury severity, and individual factors such as age, sex, and occupation. However, there is a lack of evidence regarding whether the quality aspects of a hospital are related to a successful RTW after controlling for clinical and individual factors. Hence, the aim of our study was to examine the association between the hospital quality of the workers’ compensation system and RTW of injured patients after controlling for age, sex, injury severity, occupation, factory size, city, and hospital type. Furthermore, because the successful RTW could be a gold standard of quality for workers’ compensation hospital, we hope our investigation also might give insight about the validation of quality score for workers’ compensation hospital.
MATERIALS AND METHODS
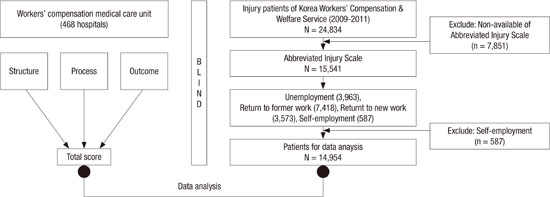
The RTW data of injured workers were constructed from 2 datasets. One included the data of 23,392 injured patients who had closed claims from 2009 to 2011 at the Korea Workers’ Compensation & Welfare Service (COMWEL). The other included RTW data from the Korea Employment Information Services (KEIS) electronic database. KEIS conducted telephone interviews with all participants to elucidate current economic activity status. Using economic activity status, RTW statuses were classified as “unemployment,” “return to former work,” “return to new work,” and “self-employment.” Return to former or new work was categorized as a RTW, and unemployment was categorized as a non-RTW. Among the 23,392 injured patients, we excluded 587 patients classified in the “self-employment” group because it is difficult to define a successful RTW. The Abbreviated Injury Scales (AISs) of the participants were calculated. Next, 7,851 participants with missing AIS data were excluded. Finally, 14,954 patients (10,991 in the RTW group and 3,963 in the non-RTW group) were included in the data analysis (Fig. 1).

Regarding the quality aspects of hospitals focused on workers’ compensation, educated staff conducted a survey from October 2013 to December 2013 at hospitals (n = 485) registered with COMWEL. COMWEL manages the workers’ compensation insurance program in Korea. Evaluations of COMWEL-contracted hospitals have been performed since 2008 (1), and there is an assessment tool to reflect the characteristics of the worker’s compensation medical care system (10). All staffs were educated in a standardized survey process, and 3 staff members including a COMWEL employee, physician, and nurse took the surveys at each hospital. Briefly, the statuses of the infrastructure, staff, and equipment were assessed as the structure quality of the hospital. Diagnoses, treatment, rehabilitation, follow-up activity, and clinical notes made by health care professionals were assessed as the process quality of the hospital. For the outcome quality of the hospital, the rate of closed claims, degree of workers’ compensation system utilization, and patient and health care professional hospital satisfaction were assessed (Fig. 2). The score of each quality aspect and their sum (total score) were calculated (10). The injured patients’ data and RTW statuses were de-identified prior to all data collection to assess hospital quality. If workers had experienced one or more hospitals, the hospital was allotted when the workers closed the claims of workers’ compensation insurance.

The χ2 test was used to examine differences in the basic characteristics of the injured patients according to RTW status. P values for trends were calculated using the Cochran-Armitage test. Because the proportion of successful RTW was more than 70%, we used log-binomial regression model to calculate the risk ratio (RR) and 95% confidence interval (95% CI) (1011). P < 0.05 was considered statistically significant.
RESULTS
The proportion of patients with a successful RTW was 75.0% among men and 65.1% among women (Table 1). There was an inverse relationship between patient age and RTW (P for trend < 0.001). The rate of RTW was 81.8% for ages 31–40 years, while 52.1% were aged above 60 years (P < 0.001). Severe and critical injuries showed the lowest rate of RTW (63.1%), while minor injuries showed the highest rate of RTW (77.2%) (P < 0.001). Non-manual workers experienced higher RTW rates than manual workers (81.0% vs. 70.6%, respectively). Smaller factories showed lower RTW rates than larger factories (67.6% in < 5, 75.0% in < 30, 77.4% in < 50, 78.4% in ≥ 50 workers factory size, P < 0.001, P for trend < 0.001). The RTW rate in non-megalopolis areas (75.7%) was higher than that in megalopolis areas (70.9%) (P < 0.001).
Table 1
Basic characteristics of study population according to return to work

![]()
Regarding the hospital types to which the injured patients were admitted, secondary hospitals (75.3%) showed the highest rate of RTW while primary hospitals (70.2%) showed the lowest rate of RTW (P < 0.001) (Table 2). The total hospital quality score had a positive relationship with the RTW rate; the rate of RTW was 69.4%, 73.1%, 76.5%, and 75.0% in the 1st, 2nd, 3rd, and 4th quartiles, respectively (P for trend < 0.001). There was no significant P value for trend in the association between the structure score and RTW rate. The RTW rate increased with the quartile level of the process score; the value in the 1st quartile of the process score was 69.9% while that in the 4th quartile was 76.1% (P < 0.001, P for trend < 0.001). The RTW rates according to increasing quartiles of the outcome score were 69.7%, 71.6%, 75.6%, and 77.0% in the 1st, 2nd, 3rd, and 4th quartiles, respectively (P < 0.001, P for trend < 0.001).
Table 2
Hospital characteristics according to return to work
*Relative risk (95% confidence interval), age and sex adjusted risk ratio (95% confidence interval).
![]()
The risk of a RTW in the 4th quartile of the total hospital quality aspect score was higher than that in the 1st quartile (RR, 1.07; 95% CI, 1.04–1.10) after controlling for age and sex. The adjusted RR (95% CI) for RTW in the 2nd, 3rd, and 4th quartiles was 1.05 (1.03–1.08), 1.05 (1.02–1.08), and 1.07 (1.04–1.10), respectively, compared to the 1st quartile process score. The adjusted RR (95% CI) for RTW in the 2nd, 3rd, and 4th quartiles was 1.02 (1.01–1.05), 1.08 (1.05–1.11), and 1.09 (1.06–1.12), respectively, compared to the 1st quartile outcome score.
These relationships remained significant after further adjustment for injury severity, occupation, factory size, city type, and hospital type. The RR (95% CI) for the total score was 1.04 (1.02–1.06), 1.06 (1.04–1.09), and 1.07 (1.05–1.10) in the 2nd, 3rd, and 4th quartiles, respectively, compared to the 1st quartile. The RR (95% CI) in the 2nd, 3rd, and 4th quartiles was 1.05 (1.02–1.07), 1.05 (1.02–1.08), and 1.06 (1.04–1.09) for the process score; and 1.02 (1.01–1.04), 1.05 (1.03–1.07), and 1.06 (1.04–1.09) for the outcome score compared to the 1st quartile score, respectively (Fig. 3).
 | Fig. 3Return to work and hospital quality score after adjusting age, gender, injury severity, occupation, factory size, city and hospital type.
Q, quartile.
|
The odds of return to former work also increased in the 4th quartile total, structure, and outcome scores compared to 1st quartile scores of the same, and the OR (95% CI) for the 4th quartile was 1.09 (1.06–1.12) for the total score, 1.09 (1.05–1.13) for the structure score, and 1.09 (1.05–1.13) for the outcome score (Fig. 4).

DISCUSSION
The present study demonstrated a significant relationship between the rate of RTW and the incremental total hospital quality score as well as for the process and outcome scores, and increments in the quality score related to the rate of RTW were associated in a dose-dependent manner. These important relationships were still significant after controlling for age, sex, injury severity, occupation, factory size, city, and hospital type.
Most industrial countries face increasing life expectancies with decreasing birth rates, and social concerns to increase labor force participation with sustainable working lives are urgently needed (12). Furthermore, because almost 75% of workers hope to resume their work even after being out of work because of illness (13), an investigation of successful RTWs was warranted. In the current study, the rate of RTW was 75.7%, even among seriously injured patients (AIS score = 3) (Table 1), which could represent the willingness of workers to RTW as described above. Hence, our study investigating the association between hospital quality and the rate of RTW is important in such an aging society.
A successful RTW requires rehabilitation sufficient to resume working capabilities, and working capabilities should be assessed in the workplace beyond the hospital environment. Hence, various ongoing efforts to support injured patients, even after discharge from the hospital, are needed. These ongoing efforts could be established through the cooperation of medical staff, workers, and employers, as well as insurers. On the contrary, if there are no ongoing efforts, successful RTWs have failed regardless of working capabilities for usual work demands (14). Hence, we assessed the follow-up activity of the medical staff in the process score and usability of the insurance system in the outcome score. The medical staff should record symptom progression notes as well as the achievement of working capabilities for the process score, and should be educated in risk factors for re-injury for the outcome score (10). For example, in a patient who suffered from work-related upper extremity disorders, pain as well as strength and range of motion of the upper extremity were recorded in the progress score. For the outcome score, medical staff should provide information regarding risk factors such as repetition, awkward postures, excessive force, inadequate work and rest cycles, and vibration (15). The process and outcome hospital quality scores were related to RTW in a dose-dependent manner in the current study.
The quality aspects of the hospital could be assessed by 3 components including structure, process, and outcome (16). The quality aspects of hospitals were organized by hospital buildings, equipment, and various medical and non-medical staff, which were referred to as structure. The way structure assists therapies and other practices represents the process. The hospital-defined target or goal as a result of the process is the outcome. However, there are some differences between general patient care and occupationally injured patient care, and improving the quality of the hospital also differed between general and workers’ compensation patients (9). For example, hospitals should provide medical expertise in the general medical care system, and provide knowledge of the relationship between job and work-related diseases in the workers’ compensation medical care system. Communication with workers, employers, and insurance officers is more important in the workers’ compensation medical care system.
The Korean Government, Ministry of Employment and Labor (MOEL) undertook the research about the quality of workers’ compensation hospital, and MOEL published the standard criteria for designation of workers’ compensation hospital (17). The criteria only reflected for prior approval for designation, but did not guarantee the quality of hospital regarding workers’ compensation. For example, that law consisted of structural criteria about medical personnel, medical facility and regional accessibility. The quality controls of that hospital were depended on COMWEL: COMWEL managed workers’ compensation insurance program in Korea. There are nine COMWEL owned hospitals, 1,554 contract hospitals and 2,822 contract clinics in Korea. However, there were no specific evaluation tools for quality aspect of worker’s compensation medical care system in Korea. Hence, COMWEL created an assessment tool to reflect the characteristics of the worker’s compensation medical care system (10). We used this assessment tool for measuring quality score in current study. Although, this tool did not get validation through other previous study, our result, the dose response relationship between hospital quality score and RTW suggest quality evaluation can get external validation. Nevertheless, validation study was needed to elucidate the exact meaning of quality evaluation system.
In the current study, the process and outcome scores for hospital quality were significantly related to the rate of RTW, but structure was not. For structure, infrastructure, staff, and equipment were assessed by questionnaire. Medical and other hospital staff have roles in the coordination of communication among workers, employers, and the insurance system, and the activities of these staff are related to a successful RTW (18). However, the scoring criteria for structure mainly represented the quantity or number of staff and equipment. The real quality of staff and equipment are more closely linked to the process score, because the process score represents the activity of the staff and usability of the equipment for successful treatment and rehabilitation. Furthermore, the satisfaction levels of the medical staff were scored as outcome quality. Hence, our current results suggest that quality has a stronger relationship with RTW status than quantity alone.
Manual workers showed lower RTW rates than non-manual workers after injury in the current study. This is simply explained by physical health being a more essential component of labor for manual workers than for non-manual workers. However, the morbidity of the injuries and musculoskeletal diseases in manual workers were higher than that in non-manual workers in Korea (19). Elderly workers and workers in small-sized factories were in the high risk group for injury, and those in this group showed a lower rate of RTW compared to others in the current study. Hence, more sincere concerns for lower socio-economic groups are needed to prevent the loss of working life and to improve the rate of RTW.
There are several limitations to the current study. Although we covered all work-related injured patients who registered in COMWEL and followed-up RTW status using national KEIS data and telephone interviews, some articles suggested that problems related to under-registered work-related patients existed (19). There were temporal mismatch between time of quality evaluation and rate of RTW in hospital. Hence, although we used blind method to match the quality of hospital and rate of RTW, there was possibility for overestimated quality score of hospital. Hence, careful considerations are needed for generalizations of our current results. Because of the lack of information about workplace duties, we could not control the interaction between the anatomical injury site and rate of RTW. When a polishing worker experiences an injury to an upper extremity, the rate of RTW to former work is not easily compared to a worker with a lower extremity injury. Chronic disease status as well as health behavior are related to sustainable work ability; however, we have no information regarding these factors. Hence, a further comprehensive study design is needed to elucidate RTWs and hospital quality scores.
In summary, our blinded study design showed that the total, process, and outcome quality scores were related to the rate of RTW in a dose-dependent manner, even after controlling for age, sex, injury severity, occupation, factory size, city, and hospital type. Hence, increments in hospital quality focused on the workers’ compensation system are needed to improve the rate of RTW for injured patients.
 XML Download
XML Download