

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Along with the development of medical science, medical culture has evolved from empirical trial and error to an evidence-based model (12). With the aim of building on a secure scientific base, the clinical trial has become the gold standard for evaluating new treatment options (12), and data from such trials are compulsory worldwide for drug market access (3).
Although the United States have always been in the lead in terms of clinical research volume, some advances have been made in emerging countries, owing primarily to the growing interest of the pharmaceutical industry in globalization (4567). Estimates vary presumably due to consulting different registries; however, previous research has confirmed a clear migration of clinical trials to Asia, with the greatest absolute increase occurring in the period 2005 to 2012 (8). Approximately thirty thousand clinical trials conducted in Asian countries are registered in ClinicalTrials.gov, accounting for more than 17% of the total (9). It has been suggested that this shift to Asian countries is aimed at acquiring a larger patient pool to permit rapid enrollment, thereby saving time and money (6).
Due to concerted efforts by the government, clinical trial volume in Korea has increased over the last decade, with Seoul being cited as one of the most active cities for clinical trials (4). To stimulate this process, the Korean Ministry of Health and Welfare established KoNECT (Korea National Enterprise for Clinical Trial), and a clinical trial infrastructure for new drug development was built around this national enterprise (410).
Public awareness plays an essential role in shaping regulations, ethical standards, and the research environment (1112), making it important to promote awareness not only among patients but also in the public at large. Despite a probable increase of interest in clinical trials, the catastrophic stem cell scandal in 2005 (13) and the constant reports of fraud committed by pharmaceutical companies (14), may create a false picture of clinical trials that creates distrust and promotes an image of investigators and sponsors as exploitative, which could encourage opposition to clinical trials.
A few studies have been published addressing the awareness and perception of clinical trials in Korea (1516) yet none of the studies were conducted in the general population. Public awareness and advocacy campaigns have been shown to be effective tools for increasing public awareness and clinical trial participation (1718). The PARTAKE survey described here is an early-stage approach to assessing public awareness and perception.
The PARTAKE survey was previously administered to 175 individuals in India (12), and our study replicates the survey in the Korean population. Its aim was to assess the level of public awareness and perception of clinical trials among the Korean public at large, using a validated survey tool.
MATERIALS AND METHODS
Survey instrument
The validity of the survey instrument was assessed by various methods, including review of the literature and consultation with experts (12). The instrument consists of 40 multiple choice and open-ended questions. It was forward translated into Korean and independently checked for clarity and meaning by two national experts, who are both fluent in English and Korean. The translation was subsequently back-translated into English and was confirmed to be equivalent to the original version. Written instructions have been added to the questionnaire to ensure its uniform use. To minimize selection bias, every fifth passer-by was invited to interview, and if in cluster, person on the very right side was asked. It was administered face-to-face in December 2014, and the detailed procedures employed were identical to those of the survey conducted in India (12).
Subject selection
A proportional quota sampling method was used for subject enrollment; this is a standard tool for opinion polls, which allows subjects to be selected based on a range of demographic factors, and ensures that the sample interviewed is representative of the population of interest. The quota sampling was done using a predetermined proportion of mutually exclusive sets for age, sex and residence area. The proportion of subset, the quota, was determined by the demographic distribution of Seoul reported in the most recent census data (19).
Sample size calculation
The sample size was calculated from the single proportions sample size formula using PASS 12 (NCSS, Kaysville, UT, USA). Assuming fifty percent of the subjects understood the concept of clinical research, the sample size needed to achieve 5% precision and 95% confidence limits was computed. To compensate for potential non-responders, we planned to enroll a total of 400 subjects.
Statistical analysis
Socio-demographics are summarized using descriptive statistics. The association between socio-demographic characteristics and clinical research perceptions were evaluated using the χ
2 test, Fisher’s exact test or the independent t test. The distribution of responses between comparing groups was tested using χ
2 goodness of fit. To assess the associations between clinical research perceptions and willingness to participate, perception scores were calculated for selected questions using defined standards, by assigning 1 point for each appropriate response. Differences in levels of public awareness and perception between India and Korea were compared with the χ
2 or independent t test. There were no missing data. Statistical Software Package for Social Sciences (SPSS version 21.0; Chicago, IL, USA) was used for all statistical analyses, and the analysis was performed by an independent statistician.
Ethics statement
Ethical review and informed consent were exempted by the institutional review board of Asan Medical Centre (IRB approval number: 2014-1061). Data were collected only from individuals who provided verbal informed consent and agreed to proceed. Written consent was not obtained since the survey was anonymous in order to provide access to as wide a public as possible.
RESULTS
Subject characteristics
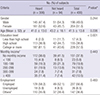
A total of 400 Seoul residents, aged between 20 and 69 years, with no previous experience of clinical trial participation responded to the survey. The validity of the survey was confirmed by the coherent responses to opposing questions. Of the respondents, 76.5% reported to have heard of clinical research. No meaningful differences between those who had heard and those who had not heard about clinical research were observed with respect to gender, age, monthly income and employment status, but disparities in educational level were apparent (Table 1).
Table 1
General characteristics of the participants
Knowledge and perceptions of clinical research
Perceptions of clinical research were evaluated using 26 questions that were designed to assess perceptions in four different categories. Each of the category is to see the perceptions of trust of the research entities, conduct of research, reasons for doing or participating in research and the value that research brings (Table 2). In the questions evaluating perceptions of the value of research, the distributions of responses to two of the five questions, V3 and V5, differed between the “heard” and the “not heard” group. The distributions of the responses to M1 and M2 were also discordant, whereas perceptions regarding the conduct of research were similar in the two groups. The distribution of response to all but one of the question appraising perceptions of trust in research entities also did not differ. The one exception was a question about confidentiality (T7).
Table 2
Clinical research knowledge and perception in those who have heard and not heard about clinical research

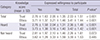
Trust perception scores were calculated based on the responses to T1, T2, T3, T4, T9 and C5, as these questions were considered to be directly related to trust in research entities such as the government, pharmaceutical companies, academic institutions and investigators, and their advocacy groups. The ethics perception score was based on responses to M3, C3, C4, T5, T6, T7, T8, and T9, since these related to the ethical standards that research entities should maintain. No remarkable differences in trust and ethics perception scores were found between the “heard” and “not heard” groups (Table 3).
Table 3
Difference between those who have heard and not heard about clinical research

Further analysis of willingness to participate revealed a positive association with both perception scores in the “heard” group but not in the “not heard” group (Table 4).
Table 4
Difference in trust and ethic perception scores between those who expressed willingness to participate and those who have not
Reasons for participation or refusal
No notable differences in the reasons given for clinical research participation were seen between the two groups (Fig. 1). The proportion of subjects who gave altruism, or treatment/medical benefits, as the reason for participation in clinical research was lower in the subjects not willing to participate than in those willing to participate, and financial gain, and being obliged to do so was higher among those not willing to participate. Treatment benefit was the single most influential reason for participation, followed by financial gain. The reasons for refusal were similar in the “heard” and “not heard” group, except for lack of knowledge (Fig. 2). The proportion of subjects who gave lack of time or lack of opportunity as the reason for refusal was lower among the “not willing” subjects while lack of trust, fear, and not caring were higher among these subjects. Thus, concerns about safety was the main reason for refusal, followed by fear and lack of trust.


Sources of clinical research information
The most trusted source of clinical research information was analysed. Academia was shown to be the single most trusted source, followed by medical doctors (Fig. 3).

Differences between India and Korea
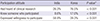
Compared to the Indian experience, a much higher percentage of the respondents stated that they had heard of clinical research or knew someone who had participated. Nevertheless the percentage of responders expressing willingness to participate was only 39.3%, significantly lower than in India (Table 5).
Table 5
Comparison between India and Korea on exposure to clinical trial and willingness to participate
DISCUSSION
The purpose of this survey was to evaluate levels of public awareness and perception of clinical research in the Korean public at large, focusing on non-participants in clinical trials. This is the first study to evaluate knowledge and perception about clinical research among Korean individuals without previous experience of clinical research participation, using a validated survey tool.
In general the survey participants had a positive view of clinical research (78.8%). The overwhelming majority of participants, greater than 76%, indicated that they had heard about clinical research. This figure agrees with an unpublished national report issued by the Korea Centers for Disease Control and Prevention (KCDC) in 2009, in which approximately 70% of the general public said that they had heard of clinical research (20). This speaks for the growing interest of the public in clinical research, as well as for the unique distribution of clinical research infrastructure in Korea, where most clinical research takes place in Seoul (21).
The proportion of subject expressed willingness to participate in clinical research was 39.3%, which is far below the rate in India (12). Although a number of explanations are possible, given that a large proportion of the subjects not willing to participate gave a lack of trust, and fear, as reasons for refusal, a lack of belief in clinical research entities may have been primarily responsible for this result. According to a survey of the general public and patients, endorsed by CISCRP (The Center for Information & Study on Clinical Research Participation), the top two ranked sources of clinical research information are the internet and media (22). It is well known that the media are a primary source of information about what happens in the world, especially in those areas where direct access to information is not feasible (23). Since Korea is a country with one of the highest internet and smart phone penetrations (24), the relatively low proportion of responders expressing willingness to participate may be partly attributed to how the internet and media shape public perceptions and attitudes.
Although head-to-head comparisons may not be appropriate due to the different measurements used, there seems to be some relation between clinical trial awareness and willingness to participate, since two similarly designed studies among Korean cancer patients led to the same conclusions as our study (1516). The study by Lee et al. (16) demonstrated that patients with previous experience of clinical trials expressed greater willingness to participate in future. Moreover the greater willingness to participate among patients who were aware of clinical trials in the study by Kim et al. (15) adds weight to the positive association between clinical trial awareness and willingness to participate. In line with this conclusion, we found that a higher percentage of the subjects in the “heard” group expressed a willingness to participate than in the “not heard” group.
To investigate how perception shapes behavior, we compared perception scores in those who expressed willingness to participate and those who did not. Both trust perception scores and ethics perception scores were shown to be related to willingness to participate. Surprisingly, these associations only existed in the “heard” group, and no notable correlation was observed in the “not heard” group. This raises the possibility that information about clinical research may not be regarded as meaningful unless the individual involved has already heard about clinical research.
Unlike India where altruism was the single most influential reason given for participation (12), treatment/medical benefit was the main reason for participation in clinical research in our study, and this is in agreement with studies performed in the patient population (1516). Concern over safety was the main reason for refusal, and in line with this, subjects who answered yes to “Researchers make sure research is safe for participants” tended to express willingness to participate in clinical research. A similar conclusion was suggested in a previous study by the KCDC (20), where a lack of trust in government, the pharmaceutical industry, and researchers were noted. These findings imply a need for public awareness and educational programs to reverse negative perceptions of clinical research.
This study has several limitations. The respondents were all Seoul residents, and may not be representative of the awareness and perception of the Korean public in general. The results might have been more reliable if we had assessed in-depth knowledge about clinical research. Also, the comparison with India should be treated with caution, due to differences in demographic characteristics.
The majority of participant had a positive view of clinical research, and a substantial proportion of the respondents indicated that they had heard of clinical research. The results suggest that the main features of clinical research are well understood among the Korean public in terms of the research purpose, value, and the voluntary nature of participation. However, there was substantial distrust of clinical research. Public awareness and educational programs addressing these negative perceptions and lack of knowledge could be an effective tool in enhancing public engaged in clinical research.
 XML Download
XML Download