

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
A Middle East Respiratory Syndrome-Coronavirus (MERS-CoV) outbreak was reported in Korea in 2015, with high mortality (37 [19.9%] deaths in total 186 MERS-CoV patients from May to November, 2015, from the Korea Centers for Disease Control and Prevention, http://www.cdc.go.kr). Several cases of MERS-CoV infection showed renal function impairment (1,2) since MERS-CoV was isolated from a Saudi Arabian man who died of progressive respiratory and renal failure (3). Some of those patients required renal replacement therapy. In addition, the MERS-CoV virus was detected in urine samples from a MERS-CoV patient (4). MERS-CoV may include kidney tropism, and dipeptidyl peptidase 4 (DPP 4) was identified as a functional receptor for MERS-CoV (5).
There are high levels of messenger RNA and protein expression of DPP 4 in kidneys and lungs (6), and DPP 4 on the surfaces of human nonciliated bronchial epithelial cells is thought to be a functional receptor for MERS-CoV (5). DPP 4 is one of the major renal brush border membrane proteins (7). In addition, DPP 4 is present in glomerular podocytes and capillaries (8).
No studies have reported the renal pathogenesis of MERS-CoV based on renal pathology findings, in spite of some evidences of kidney tropism in MERS-CoV. We report a case of a MERS-CoV survivor who underwent a kidney biopsy.
CASE DESCRIPTION
A 68-year old man was transferred to our center presenting with 5 days of coughing, shortness of breath, and general weakness on May 20, 2015. The patient was relatively healthy, except for well- controlled hypertension. He returned to Korea after visiting Bahrain and Saudi Arabia for approximately 3 weeks and developed fever, myalgia, and general weakness 1 week after returning home. He visited a primary hospital, and computed tomography of his chest revealed ground glass opacity in the right upper lobe. He was transferred to a tertiary hospital after 4 days of ineffective treatment in the primary hospital; additional pneumonic infiltration in the left lower lobe was observed. His symptoms worsened, and MERS-CoV polymerase chain reaction was confirmed to be positive. The patient was admitted to our hospital, which is equipped with negative pressure isolation wards.
The patient complained of myalgia, dry cough, dyspnea, and nausea-vomiting at the time of admission. His vital signs were as follows: blood pressure, 135/72 mmHg; heart rate, 85 /minutes; respiration rate, 20 /minutes; and peak body temperature, 38.6°C. The peripheral capillary oxygen saturation (SpO2) monitor showed 96% with 2.5 L/minute of oxygen via nasal cannula. The results of the laboratory tests were as follows: WBC, 3,400 /μL (segmented neutrophils 80.4%, lymphocytes 14.5%, monocytes 4.8%); hemoglobin, 13.7 g/dL; platelets, 160,000/μL; AST/ALT, 176/97 unit/L; albumin, 2.5 g/dL; and isotope dilution mass spectrometry (IDMS) traceable serum creatinine (SCr), 1.0 mg/dL. A dipstick test showed albumin and blood (negative/negative). We found multiple pneumonic infiltrations in the right upper and middle lobes and in the left lower lobe on a chest radiography.
The patient was treated with 180 μg of pegylated interferon-alpha on hospital day (HOD) 1 and 1,800 mg of ribavirin (600 mg every 8 hours) daily from HOD 3 to HOD 7. Anti-viral treatment was discontinued thereafter because of sustained fever and thrombocytopenia (lowest platelet count was 56,000/μL).
The patient was placed on a mechanical ventilator on HOD 4, which was accompanied by the progression of multiple pneumonia infiltrations. The patient underwent a tracheostomy on HOD 23 and was weaned from the mechanical ventilator on HOD 39. The blood and urine cultures were negative, and the sputum cultures identified multiple drug resistant Acinetobacter baumannii (MDR AB), methicillin resistant Staphylococcus aureus (MRSA), Pseudomonas aeruginosa, and Enterobacter aerogenes. We prescribed antibiotics, including vancomycin (from HOD 12 to HOD 21), tigecycline (from HOD 21 to HOD 34), and colistimethate (from HOD 24 to HOD 32), according to the isolated microorganisms and antibiotics susceptibility results. The MERS-CoV polymerase chain reaction results from sputum specimens became negative on HOD 37. In addition, the tests of urine and stool specimens obtained on HOD 37, which were performed to ensure the absence of MERS-CoV, were negative.
The microalbumin to creatinine (ACR) and protein to creatinine (PCR) ratios from randomly collected urine on HOD 7 were 113.6 and 1,327.3 mg/g creatinine (Cr), respectively. Urinary protein excretion steadily increased for an ACR of 538.4 mg/g Cr and a PCR of 3,025.8 mg/g Cr on HOD 32. The IDMS traceable SCr level increased to 3.0 mg/dL on HOD 41. The IDMS traceable SCr level was still 1.7 mg/dL on HOD 55 and the ACR and PCR were 31.5 mg/g Cr and 1,075.6 mg/g Cr (Fig. 1). We performed the kidney biopsy on HOD 55.
Fig. 1
The progression of renal function, albumin, and urinary protein excretion. (A, B) The IDMS traceable serum creatinine and IDMS-MDRD estimated glomerular filtration rate. (C) The progression of serum albumin level. (D, E) The microalbumin to creatinine ratio and protein to creatinine ratio from randomly collected urine. The polymerase chain reaction of Middle East Respiratory Syndrome-Coronavirus from the respiratory tract specimens was negative on hospital day 37; the patient underwent a kidney biopsy on hospital day 55. IDMS, isotope dilution mass spectrometry; HOD, hospital day; MDRD, modification of diet in renal disease.

Light microscopy and electron microscopy kidney tissues
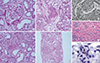
We performed the standard light microscopic and electron microscopic tests, except for immunofluorescence test due to fear of the possible virus transmission. We assessed 4-μm formalin fixed and paraffin-embedded (FFPE) tissue sections with hematoxylin eosin (H&E) staining. There was no glomerular pathology, and acute tubular necrosis was the main finding on light microscopy. In addition, we found proteinaceous cast formation and acute tubulointerstitial nephritis (Fig. 2). No electron dense deposits were observed with electron microscopy.
Fig. 2
Light microscopic findings of kidney tissues (H&E staining) (17,18). (A) Glomerular pathology was not observed. (B) Acute tubular necrosis showing denuded tubular epithelial cells. (C) Some tubules showed protenaceous cast formation. (D) Acute tubulointerstitial nephritis showing numerous inflammatory cells in tubules and the interstitium (A, B, C: magnification ☓ 200, D: magnification ☓ 40). (E) Proximal tubules with vacuolar degenerative alterations (magnification ☓ 400) (17). (F) Moderate necrosis and detachment of tubular epithelium (magnification ☓ 100) (18). (G) Viral antigen detected in the glomerular macrophage (arrow) (magnification ☓ 1000) (18).
Additionally, we performed in situ hybridization and confocal microscopy to confirm the presence of viral particles.
In situ hybridization of kidney tissues
The in situ detection of MERS-CoV was performed manually using a RNAscope kit (Advanced Cell Diagnostics, Hayward, CA, USA) according to the manufacturer’s instructions. Briefly, 4-μm FFPE tissue sections were pretreated by heating and protease application prior to hybridization with a target probe to the MERS-CoV (MERS-CoV isolate England/2/2013 complete genome: 431631, Advanced Cell Diagnostics). Positive staining was indicated by the presence of brown punctuate dots in the nucleus and/or cytoplasm. MERS-CoV expression was scored using the instructions for the RNAscope FFPE Assay Kit.
Confocal microscopy
Confocal microscopy was performed with an LSM510 META confocal microscope (Carl Zeiss, Jena, Germany). For the immunofluorescence assays, FFPE sections were cut into 4-μm thick sections. Xylene and ethanol were used for deparaffinization and rehydration. The sections were stained with anti-goat DPP 4 polyclonal antibody (R&D Systems, Minneapolis, MN, USA), mouse anti-mouse aquaporin-1 (AQP-1) antibody (Abcam, Cambridge, UK), and sera from MERS-CoV patients (patient’s serum 9 weeks after symptom onset and the serum from a convalescent plasma donor; 1:2,000 dilution) as primary antibodies in a blocking reagent overnight at 4°C. Alex Fluor 555-conjugated anti-goat, Alex Fluor 647-conjugated anti-mouse (Molecular Probes, Eugene, OR, USA), and Alex Fluor 488-conjugated human IgG (Molecular Probes) were used as secondary antibodies. The sections were washed and incubated for an additional 5 minutes with 4´6-diamidino-2-phenylindole (DAPI) (Molecular Probes) for counterstaining. For the negative controls, the primary antibodies were omitted.
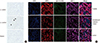
We could not verify viral particles in the sections of in situ hybridization (Fig. 3A). No evidence of MERS-CoV (human IgG) co-stained with DPP 4 was observed with confocal microscopy (Fig. 3B).
Fig. 3
The detection of Middle East Respiratory Syndrome-Coronavirus: in situ hybridization and confocal microscopy. (A) Middle East Respiratory Syndrome-Coronavirus (MERS-CoV) was not evident in the in-situ hybridization method (magnification ☓ 200). The first and the second rows indicate negative and positive control (black arrow). The third row shows results from patients. There was no brown punctuate dot in the nucleus and/or cytoplasm. (B) The kidney tissue samples were co-stained for MERS-CoV (human IgG; green) and dipeptidyl peptidase 4 (DPP 4; red). DPP 4 was primarily stained in proximal tubules (aquaporin-1; violet). The first and second rows indicate the reaction using patient serum 9 weeks after symptom onset and the serum from a convalescent plasma donor. The third row is the negative control.
The IDMS traceable SCr level was 0.9 mg/dL (the estimated glomerular filtration rate was 83.9 mL/minutes/1.73 m2) on HOD 125. A urine dipstick test was negative for albumin and 2+ blood at that time, and the ACR and PCR were 5.8 and 105.6 mg/g Cr, respectively.
DISCUSSION
The first case of MERS-CoV infection had progressive renal dysfunction. And some patients with MERS-CoV infection who presented with severe pneumonia and acute respiratory distress syndrome showed acute kidney injury (AKI) thereafter (1,2,9–11).
Kidney involvement in human coronavirus cases was observed in the Severe Acute Respiratory Syndrome-Coronavirus (SARS-CoV) epidemic in the early 2000. A study reported that SARS-CoV infection showed 6.7% of acute renal impairment and 84.6% of proteinuria on dipstick tests (12). Another study detected SARS-CoV in the distal convoluted tubules of the kidney (13). Polymerase chain reaction fragments of coronavirus were detected in urine from 21%–50% of SARS patients. These findings suggested a possibility of kidney tropism in coronavirus cases (14). In addition, there were some reports about MERS-CoV RNA in blood and urine samples. A case showed that MERS-CoV was present in the urine after renal failure on 14th day after the onset of illness (10). And another case showed that viral RNA in urine was positive from the 20th to the 30th day after the onset of illness accompanied with positive RNA in the blood from the 13th to the 30th day (4).
The organ tropism of human coronavirus is primarily determined by the ability of the receptor binding protein to bind a cell surface receptor (5). DPP 4 was identified as a functional receptor for MERS-CoV (5). DPP 4 is a widely expressed serine peptidase that exists on the surface of various cell types, and the renal expression levels of its messenger RNA and protein are high (6,15). DPP 4 is one of the major renal brush border membrane proteins (7), and it is present in glomerular podocytes and capillaries, as well (8). DPP 4 was previously co-stained with a MERS-CoV infected human kidney cell line (16).
We performed a kidney biopsy to evaluate for persistent proteinuria 8 weeks after the onset of symptoms; however, we failed to reveal viral particles in compatible ultrastructures. MERS-CoV polymerase chain reaction from urine, which was performed 6 weeks after the onset of symptoms to ensure the absence of the virus from various specimens, was negative. There are several reports about the AKI in H1N1 infected patients. And pathophysiologic mechanism of AKI in H1N1 infected patients are multifactorial including hyperperfusion, renal vasoconstriction, rhabdomyolysis in the setting of severe inflammatory response syndrome. In addition, a report showed viral particles in the glomerulus macrophage cytoplasm and it might be an evidence of circulating virus (17,18). The kidney injury in this case may be related to antibiotics, such as colistimethate and tigecycline as high doses of the latter were used to treat MDR AB and MRSA. Acute tubulointerstitial nephritis supports this rationale. However, the interpretation of these results was limited by autolysis of the tissues, and direct renal involvement by MERS-CoV could not be ruled out. In addition, we suggest that the renal pathological changes associated with MERS-CoV may be caused indirectly by a systemic toxic reaction resulting from respiratory failure or a harmful immune response and cytokine reaction induced by viral infection, as well as directly by the cytopathic effect mediated by virus replication.
SARS-CoV patients developed AKI at a median duration of 20 days from the onset of infection, which was compatible with the late viremic or the hyperimmune response phase of the infection (19). The polymerase chain reaction of coronavirus fragments was detected in urine between the second and third weeks of viral infection (14). One report showed that the MERS-CoV polymerase chain reaction was positive after 3 weeks in the blood (4). 26.7% of the patients in our MERS-CoV cohort (8 patients in a total of 30 patients) showed AKI, and the median time of AKI occurrence was 16 days from the onset of symptoms. The mean urinary PCR was highest approximately 4 weeks after the symptom onset (20). In this case, urinary protein excretion started to increase in 2 weeks after the onset of symptoms and steadily increased till 5 weeks. And the highest SCr was observed at 5 weeks after symptom onset. The elapsed time from symptom onset to the evidence of kidney injury is compatible with previous reports. We performed urinary MERS-CoV polymerase chain reaction and kidney biopsy too late (6 and 8 weeks after the onset of symptoms) than previous reports because of the general condition of the patient and the fear of in-hospital virus transmission. Direct involvement of the kidneys by MERS-CoV still could not be ruled out.
Although a few reports showed viral RNA in blood and urine samples, the relationship between the virus renal tropism and the physiopathology of the renal injury is not clear. And the independent renal viral replication and/or active urinary secretion of the virus remain unsolved. We can only say that localized MERS-CoV infection i.e., viral RNA detection in pharyngeal and tracheal swabs without systemic dissemination, results in favorable outcome. And viral dissemination through blood and urine under the impaired cytokine response leads to worse or fatal outcome (4). In the future, the viremic status and urinary virus excretion of the patient should be investigated especially in severe cases, and a timely kidney biopsy should be performed, with thorough precautions, to reveal the direct effects of MERS-CoV with respect complications. It could be helpful to monitor virus status in blood and urine samples from 2 weeks after the onset of illness.
 XML Download
XML Download