

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The Republic of Korea (ROK) has adopted a military conscription system, unlike many other nations. Therefore, all healthy young men have a duty to serve in the military, and each year, more than 250,000 people join the army in Korea (1). During the term of military service, some soldiers unfortunately suffer extensive damage from serious disease or injuries, regardless of proper management. In these cases, medical would be contemplated. Medical retirement can cause not only personal damage but also military and social problems, including increased medical costs and decreased productivity of families who care for or assist patients. This problem is particularly serious because most members of the armed forces are young men under 30 years old.
In a previous report, we investigated the clinical characteristics of ocular trauma in hospitalized patients in the Armed Forces Capital Hospital in Korea. Among 2,207 patients who were hospitalized at the department of ophthalmology over 10 years (from January 2001 to December 2010), just 790 patients (35.8%) had experienced ocular trauma (2). Although trauma is usually thought to be closely related to military medicine, these data suggested that non-traumatic mechanisms (64.2%) accounted for a substantial proportion of ocular disease in military medicine.
Many soldiers with medical problems are compassionately discharged from military service. However, epidemiologic studies about medical retirement in the ROK Army have not been paid attention to by conventional medicine, and the literature is consequently sparse. Investigation into the epidemiologic characteristics of medical retirement could lead to practical guidelines, including essential items for large-scale physical examinations for conscription. In addition, this draft screening could reduce the individual disbenefit and social opportunity costs.
The purpose of this study was to investigate the epidemiologic characteristics of medical retirement from the ROK Army due to visual impairment. In particular, we focused on young patients with non-traumatic visual impairment.
MATERIALS AND METHODS
This study employed a retrospective cohort design. Patients who were permitted by the physical evaluation board to retire from the ROK Army due to visual impairment were included from six armed forces hospitals in Korea (the Armed Forces Capital, the Armed Forces Chuncheon, the Armed Forces Gangneung, the Armed Forces Daejeon, the Armed Forces Busan, and the Armed Forces Cheongpyeong) over 5 years between January 2010 and December 2014.
For security reasons, we cannot disclose exact details of the ophthalmologic criteria for medical retirement, but they are briefly and generally described here. Patients were retired if they met any of the following conditions: 1) Best-corrected visual acuity is lower than 20/200 in one eye, or 40/200 in the better eye, 2) Glaucoma with a glaucomatous visual field defect is confirmed by standard automated perimetry in at least three examinations two weeks apart, and by the presence of corresponding structural damage in the optic disc or retinal nerve fiber layer, 3) Glaucoma surgery including filtering or glaucoma drainage-device surgery (only laser treatment is excluded), 4) Non-glaucomatous visual field defect larger than 1/4 in central 30 degree, 5) Diplopia and oculomotor dysfunction lasting six months or longer, 6) Bilateral pseudophakic eyes, 7) An area of retinal degeneration is over half of the total retina, 8) Duration of retinal detachment longer than three months in spite of treatment, 9) Bilateral surgery of retinal detachment (simple laser retinopexy or intravitreal gas injection is excluded), 10) Penetrating keratoplasty, and 11) Ophthalmologic malignancy.
Patients were grouped based on chart review by the presence of trauma, and we collected demographic and clinical data including age, gender, best-corrected visual acuity, bilaterality, etiology of the ophthalmologic disease, ocular surgery, and military rank. The etiology of ophthalmologic disease was classified into five categories according to the anatomy of the eye as follows: ocular surface, lens, retina, optic nerve and extraocular visual pathway, and extraocular muscle and orbit. Each anatomical category was subdivided into the type of disease as necessary.
Differences in demographic and clinical characteristics between patients with trauma and without trauma were assessed using the independent t-test and the chi-square test. The probability level for statistical significance was set at 5%. Data were recorded and analyzed using SPSS for Windows, version 20.0 (SPSS Inc., Chicago, IL, USA).
Ethics statement
The institutional review board at the Armed Forces Medical Command, Seongnam, Korea reviewed and approved the study protocol and exempted the informed consent for this study (IRB No. AFMC-14-IRB-036). We performed all procedures in accordance with the tenets of the World Medical Association’s Declaration of Helsinki.
RESULTS
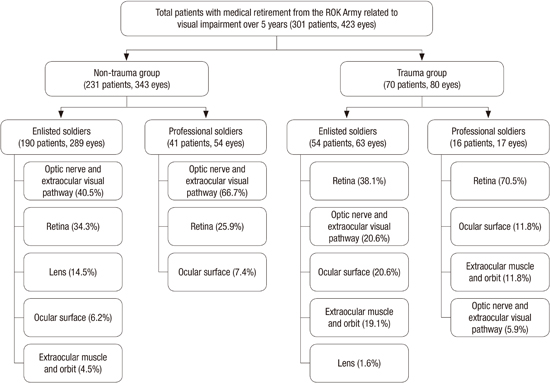
Three hundred and one patients retired from the ROK Army due to visual impairment over the past five years, and a total 423 eyes were compatible with the ophthalmologic criteria for medical retirement. Almost all patients were male, with only two females included; one was a 24-year-old trauma patient with a globe rupture and the other was a 43-year-old non-trauma patient with bilateral normal tension glaucoma. The majority of retired patients came from the Armed Forces Capital Hospital (264 eyes from 185 patients), followed by the Armed Forces Chuncheon, the Armed Forces Gangneung, the Armed Forces Daejeon, the Armed Forces Busan, and then the Armed Forces Cheongpyeong Hospital (Fig. 1).
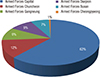 | Fig. 1Diagrams showing the distribution of patients grouped by hospital. Proportion of patients met the ophthalmologic criteria for medical retirement from the ROK Army.
|
A summary of all patients with medical retirements due to visual impairment from the ROK Army is shown in Fig. 2. The mean patient age was 24.5 ± 9.6 years (range, 18-57 years). More than three-quarters of patients (231/301, 76.7%) had non-traumatic impairment, and most patients (244/301, 81.1%) were enlisted soldiers that were significantly younger (21.0 ± 2.4, range of 18-32 years) than professional soldiers (39.2 ± 14.0, range of 19-57 years). The distribution of the age groups and the etiology of ophthalmologic disease for military retirement are presented in Fig. 3 and 4, respectively. Most patients (86.7%) were under the age of 30, and the number of patients was highest in the youngest group (age, 18-20 years). The three most common etiologies were disease of the optic nerve and extraocular visual pathway, followed by retinal disease and then trauma.


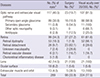
Table 1 presents the demographic data and ocular characteristics from the trauma and non-trauma groups. Non-traumatic mechanisms caused medical retirement due to visual impairment in 343 eyes (81.1%), and these patients were significantly older than those in the trauma group. The ratio of enlisted soldiers to occupational soldiers was not different between the two groups. The eyes in the non-trauma group had better best-corrected visual acuity and a higher proportion of patients with a visual acuity over 20/200 than those in the trauma group (P < 0.001). Anatomical category distributions differed significantly between the trauma and non-trauma groups (P < 0.05). In the non-trauma group, disease in the optic nerve and extraocular visual pathway was the most common cause (44.6%) of visual impairment, followed by disease of the retina, lens, ocular surface, and extraocular muscle and orbit. On the contrary, retinal disease was the most common cause (45.0%) of visual impairment in the trauma group, followed by disease of the optic nerve and extraocular visual pathway, ocular surface, extraocular muscle and orbit disease, and lens. The rate of ocular surgery was higher in trauma group (P < 0.001).
Table 1
Demographic and ocular characteristics in patients with and without trauma
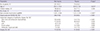
*Chi-square test except age and best corrected visual acuity; †Percentage in all subjects; ‡Student’s t-test; §Percentage in the non-trauma or trauma group. MAR, minimum angle of resolution.
![]()
Table 2 compares demographic and ocular characteristics between enlisted soldiers and professional soldiers in the non-trauma group. Enlisted soldiers were significantly younger (21.0 ± 2.6 years, range of 18-32 years) than professional soldiers (43.6 ± 12.7 years, range of 19-57 years) and had a higher rate of impairment (289/343, 84.3%). Enlisted soldiers had better best-corrected visual acuity and a higher proportion of them had a visual acuity over 20/200 compared to the professional soldiers group (P < 0.01). Disease of the optic nerve and extraocular visual pathway was the most common cause of retirement in both enlisted and professional soldiers. Among professional soldiers, 66.7% of patients had disease of the optic nerve and extraocular visual pathway, and there were no cases of lens or extraocular muscle and orbit disease.
Table 2
Comparison of demographic and ocular characteristics between enlisted soldiers and professional soldiers in 231 eyes without trauma

*Chi-square test except age and best corrected visual acuity; †Percentage in all subjects without trauma; ‡Student’s t-test; §Percentage in the enlisted or occupational soldiers group. MAR, minimum angle of resolution.
![]()
Anatomical categories were subdivided into type of disease in the eyes of enlisted men without trauma (Table 3). The optic nerve and extraocular visual pathway category was divided into primary open angle glaucoma (POAG), secondary glaucoma, optic neuropathy, and amblyopia. POAG was the most common single disease type in this category and in all enlisted men without trauma. There were no cases of primary angle closure glaucoma. Uveitis and surgery induced glaucoma, particularly photorefractive laser surgery and phakic intraocular lens surgery, and pseudophakia was included in secondary glaucoma. Genetic and compressive mechanisms were included in other optic neuropathies. The retinal category was divided into retinal dystrophy, retinal detachment, unknown maculopathy, retinal vascular disease, and chorioretinal inflammatory disease. The most common cause of retinal dystrophy was retinitis pigmentosa (44/53, 83.0%). Idiopathic or myopic choroidal neovascularization was included in unknown maculopathies. All cases in the lens category were bilateral congenital cataract. These patients underwent surgery and had a final visual acuity over 20/200. Corneal opacity due to infection was the leading cause of dysfunction in the ocular surface category (6/18, 33.3%), and we included keratoconus and other non-infectious corneal opacities associated with photorefractive surgery, dystrophy, and systemic disease. Diplopia (12/13, 92.3%) and one case of orbital tumor were included in the extraocular muscle and orbit category.
Table 3
Type of ophthalmologic disease in 289 eyes of 190 enlisted soldiers without trauma
*Percentage in all eyes of enlisted soldiers without trauma; †Percentage in each types of ophthalmologic disease.
![]()
Except the lens category, a high percentage of subjects had surgery in the retinal detachment category (82.1%). The proportion of patients with a visual acuity over 20/200 was higher in the glaucoma (98.9% in POAG and 100% in secondary glaucoma), extraocular muscle and orbit (100%), and retinal dystrophy (98.1%) categories.
DISCUSSION
In this study, we investigated the epidemiologic characteristics of medical retirement from the ROK Army due to visual impairment. Most patients (86.7%) were under the age of 30 and the three most common etiologies were disease in the optic nerve or extraocular visual pathway, retinal disease, and trauma. Contrary to the general concepts that trauma could be closely related to the military medicine, non-traumatic causes accounted for 81.1% (343/423 eyes) of medical retirements due to visual impairment. In the non-trauma group, disease in the optic nerve and extraocular visual pathway was the most common cause; in particular, POAG accounted for 30.8% of retirements despite young patient age. To the best of our knowledge, this is the first study to provide information about medical retirement from the ROK Army due to visual impairment.
Young patients have a much higher risk of ocular trauma because they are exposed to more frequent physical activity and military exercises. The mean age was significantly younger in the trauma group than in the non-trauma group. All but three trauma patients were under 30 years old, which could be due to the age imbalance related to the age of conscription. Similar results can be found in our previous report, which indicated that 90.6% of patients who were hospitalized due to ocular trauma were under 30 years old (2). Retinal disease was the most common injury. The trauma group had worse best-corrected visual acuity and a lower proportion of patients with a visual acuity of 20/200, even though they had more surgeries. These findings are consistent with previous studies showing that posterior wound location predicted poor visual outcome (234). Poor visual outcomes in the trauma group regardless of surgery reminds us that prevention is the best cure for trauma.
Interestingly, 81.1% of medical retirements due to visual impairment stemmed from non-traumatic causes, even though patients were young; this was surprising because health-related non-traumatic diseases tend to increase with age. Disease of the optic nerve and extraocular visual pathway was the most common anatomical category, and in particular, POAG was the most common single disease type of visual impairment in patients without trauma. Retinal disease, which mostly comprised dystrophy and detachment, was the second most common cause of medical retirement. Lens disease, which consisted of bilateral congenital cataract, was the third most common disease category.
Diseases that have a high prevalence rate at a young age should be screened for more effectively and specifically, and we focus on the military rank of the patients. Professional soldiers volunteer for military service as a job. They must pass a physical-fitness test for their duty and therefore undergo physical examinations and can receive evaluations for specific diseases. In contrast, enlisted soldiers have an obligation to serve in the military and are screened with a simple large-scale physical examination for the draft. Moreover, the enlisted soldiers group is significantly younger than the professional soldiers group. Therefore, identifying characteristics of medically retired enlisted soldiers is an important task.
In enlisted soldiers without trauma, POAG, retinal dystrophy, congenital cataract, and retinal detachment were the four most common single disease types that caused medical retirement from the ROK Army due to visual impairment. Therefore, a systematic screening system for detection of POAG and retinal dystrophy should be developed. Disease processes of POAG and retinal dystrophy are usually slow and gradual and have a progressive and irreversible course. Over 98% of patients with POAG and retinal dystrophy had a visual acuity over 20/200. Therefore, it is almost impossible to detect these diseases with a conventional vision test. In fact, POAG is usually asymptomatic until the later stages of the disease and is characterized by typical optic nerve head damage or glaucomatous visual field defect. In addition, most retinal dystrophy in our study was retinitis pigmentosa (83.0% of retinal dystrophy), which is characterized by difficulty with night vision and loss of peripheral visual fields. Therefore, fundus examination of the optic disc and retinal dystrophy, along with the visual field test, could be useful for ocular screening in addition to the conventional vision test.
There is little information available on the epidemiology of glaucoma patients under 40. Most patients are over 40 years old, based on population-based studies of epidemiology in glaucoma, including the Namil study in central Republic of Korea (5678910111213141516). In general, the prevalence and incidence of glaucoma consistently increases with age, and glaucoma in young patients is regarded as juvenile-onset open angle glaucoma, which is an early onset form of open angle glaucoma. This disease usually begins between the ages of 4 and 35, often with a strong hereditary factor, and is characterized by extremely high intraocular pressure (IOP) with subsequent damage to the optic nerve and visual field (17). Furthermore, this disease responds poorly to drug or laser treatment and often requires multiple surgical interventions (18).
However, clinical features in our glaucoma patients differ from those of patients with typical juvenile-onset open angle glaucoma. About half of all POAG patients (47 eyes, 50.5%) visited the ophthalmologic clinic due to symptoms associated with increased mean IOP (36.02 ± 14.01 mmHg), such as ocular pain, blurred vision, colored halos around lights, and frontal headache. However, the other half (46 eyes, 49.5%) were diagnosed incidentally with normal mean IOP (15.46 ± 2.72 mmHg) and had no symptoms related to IOP. Although the detailed data for glaucoma patients in our study are not shown, we plan to provide information about the characteristics of young male glaucoma patients in Korea in a future study.
The third most common disease causing medical retirement in enlisted soldiers without trauma was lens disease, and all of these cases involved bilateral congenital cataracts. We suspect that these congenital cataracts were mild enough that the lens opacity did not interfere with vision, and surgical correction might be unnecessary, because all of these cases were diagnosed incidentally during medical examinations for other ocular problems. The criterion of the ‘bilateral pseudophakic eyes’ is essential in terms of accommodative disorder in young ages, however, unnecessary operation could be performed for the purpose of evading military service, and it is a politically and socially sensitive issue. Therefore, this criterion needs to be reassessed with definite limitations and considerations such as preoperative visual status, causative disease, and quality of life regarding the loss of accommodation. Retinal detachment was the fourth most common disease, but screening for this is difficult and less useful, as disease onset is usually abrupt and visual outcomes may improve after treatment. The relatively high rate of surgery in patients with retinal detachment might represent an active trial for the treatment of the disease.
Our study is limited, as an epidemiologic study could not include the whole population due to different principles at each armed forces hospital. Therefore, we could not calculate the accurate prevalence and incidence of medical retirement from the ROK Army. However, we believe that our results represent the general population because most military patients with advanced disease are treated at the Armed Forces Capital Hospital, as it is the only tertiary hospital in the medical system of the ROK Army. In fact, the Armed Forces Capital Hospital has treated more patients and eyes than all of the five other armed forces hospitals put together, as shown in Fig. 1. According to the Annual report of statistics on national defense (1), 46,025 people were admitted to all armed forces hospital in 2013, and patients of six hospitals in this study were accounted for up to sixty percent of them. From this statistics we deduced that 100 patients retired from the Korean Army due to visual impairment annually, and the incidence of medical retirement due to visual impairment was around 0.02% considering that 630,000 soldiers are in the military services (19).
In conclusion, the majority of patients who retired from the ROK Army due to visual impairment were young and retired due to non-traumatic impairment. The two most common types of disease were POAG and retinal dystrophy. It is highly likely that the visual field test and fundus examination would be more effective than the conventional vision test if used as a large-scale screening for the draft. This could prevent aggravation of diseases due to strenuous physical activity and also reduce needless waste of personal time and social opportunity costs.
 XML Download
XML Download