

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Erectile dysfunction (ED) is defined as the inability to achieve and maintain an erection sufficient to permit satisfactory sexual intercourse. It has been estimated to affect 20 to 30 million men in the United States (1). Since aging is one of the main risk factors for ED, most men will be afflicted by this condition during their lifetime (23). ED can be classified as psychogenic, neurogenic, hormonal, arterial, cavernosal, or drug-induced. However, vasculogenic factors (arterial and cavernosal) are mostly related with aging.
In spite of a previously introduced arteriogenic ED model, there are few studies of atherosclerosis- or hyperlipidemia-induced ED models (4). Reasons for this may be that too much time is required to cause pelvic atherosclerosis by feeding cholesterol to rats and that it is difficult to model ED solely by atherosclerosis. Another reason is that rats are known to be cholesterol resistant, which is the traditional method of developing atherosclerosis (5).
Considering the points mentioned above, endothelial injury is essential to creating an atherosclerosis-induced vasculogenic ED model because it can enhance the process of atherosclerosis (6). Therefore, in our study we examined a chronic pelvic ischemia (CPI) model, which is based on both endothelial injury and a hypercholesterol diet. The CPI model has been validated in several previous studies as reported by Nomiya et al. (78).
Omega-3 fatty acids are limited in our diet, with the main sources being fish and plants. Long chain omega-3 fatty acids, docosahexaenoic acid and eicosapentaenoic acid, have well-described beneficial effects on cardiovascular disease, diabetes mellitus, lipid profiles, and other inflammatory diseases in humans (9). Suggested potential mechanisms for their protective effects are lowering oxidative stress, reducing the secretion of pro-inflammatory cytokines, and attenuation of atherosclerotic plaques (910).
There have been few studies regarding the action of omega-3 fatty acids on erectile function. The aim of this study was to investigate whether the omega-3 fatty acids helps to improve erectile function in an atherosclerosis-induced ED rat model.
MATERIALS AND METHODS
Animal groups and experimental design
Specific pathogen-free male Sprague-Dawley rats (250–280 g) were obtained from the Hanlim Inc. (Osan, Korea). Upon arrival, animals were randomized and housed three per cage. The animals were 8 weeks of age and were acclimated for at least 2 weeks. They were all kept under 12 hours light-dark cycles at room temperature (22°C ± 2°C), and had free access to a standard diet and water. The rats were randomly assigned to different experimental groups: 1) the Control group that underwent a sham operation and received a regular diet and water; 2) the Pathologic group that underwent endothelial injury of the iliac arteries and was provided a 2% cholesterol diet (Research Diets, New Brunswick, NJ, USA) for 4 weeks; and 3) the Treatment group, after establishment of the CPI model, that was provided a high-fat diet for 4 weeks and then treated with omega-3 fatty acids ([DHA] ethyl ester > 98% and [EPA] ethyl ester > 98%, Cayman Chemical, Ann Arbor, MI, USA) with a regular diet for 2 weeks. Omega-3 fatty acids (200 mg/kg; DHA: 100 mg/kg/day + EPA: 100 mg/kg/day) were offered every day by oral gavage.
Chronic pelvic ischemia model
Animals were anesthetized by inhalation of 2.5%-3.5% isoflurane. An inguinal incision was made and, through dissection into the iliac fossa, the femoral artery and superficial epigastric artery were isolated. A 2Fr Fogarty catheter (Edwards Lifesciences, Irvine, CA, USA) was passed into the femoral artery through a small incision and up to the common iliac artery. To induce endothelial injury, the balloon of the catheter was inflated with 0.2 mL of air and was pulled down to the femoral artery. This maneuver was repeated 10 times. The same procedure was performed on the contralateral side. In the control group sham operation, only an inguinal incision and iliac artery exposure, with subsequent skin closure, was performed.
Measurement of intracavernous pressure
Under anesthesia, polyethylene tubing (PE-50) was inserted into the left carotid artery in order to record blood pressure. A 22-gauge angiocatheter was connected to PE-50 tubing filled with heparinized saline (50 U heparin/mL) and inserted into the left corpus cavernosum for intracavernous pressure (ICP) measurement. After confirming the location of the major pelvic ganglion, which was placed on the lateral aspect of the prostate, electrostimulation was performed twice on each cavernous nerve. Stimulation was performed at 5 V and 20 Hz, at more than 5-minute intervals, with bipolar hook electrodes using an electronic stimulator (Grass SD9, Grass Instrument, Quincy, MA, USA). The major indices for evaluating erectile function were maximum ICP and the ICP/mean arterial pressure (MAP) ratio. ICP and blood pressure were monitored using PowerLab™ (AD Instruments, Colorado Springs, CO, USA).
Quantitative western blots
Penile homogenates of frozen tissue (100 mg) were obtained using T-PER and protease inhibitors (3 µM leupeptin, 1 µM pepstatin A, 1 mM phenyl methyl sulfonyl fluoride) and centrifuged at 100,000 × g for 10 minutes. Protein concentration was determined with the Bradford method (Bradford solution: Sigma, Saint Louis, MO, USA) and 40 µg of all samples were loaded. Equal amounts of supernatant protein (30 µg) were run on 7.5% or 10% (ACTA2) polyacrylamide gels and submitted to western blot immunodetection using the following primary antibodies: HIF-1α, eNOS, TGF-β1 (TBST buffer 1:200; Santa Cruz Biotechnology, Santa Cruz, CA, USA; overnight), actin (2.5% skim milk 1:3,000; Cell Signaling, MA, USA; 1 hour, room temperature), and the following secondary antibodies: HIF-1α, eNOS, TGF-β1 anti-rabbit (1:30,000; Sigma). Band intensities were determined with densitometry and were corrected on the basis of the respective intensities of a housekeeping protein, glyceraldehyde-3-phosphate dehydrogenase (GAPDH), upon reprobing.
Statistical analysis
Continuous variables were analyzed using one-way ANOVA and expressed as the mean ± standard deviation (SD). A Kruskal-Wallis test was used to analyze non-parametric variables. All analyses were performed using SPSS software (Version 20.0, SPSS Inc., Chicago, IL, USA). A P value < 0.05 was considered statistically significant.
RESULTS
No rats died during the CPI-model or sham operations. Feeding of omega-3 fatty acids did not cause any side effects or other unusual signs. Body and tissue weight was not significantly different between the three groups.
Erectile response to cavernous electrostimulation
The results of cavernosal pressure measurement are shown in Table 1. In vivo erectile function (maximal ICP, ICP/MAP, and slope values) was measured. In the Control group, these values were 70.06 ± 2.31, 0.52 ± 0.05, and 2.93 ± 1.17, respectively. In the Treatment group, the maximal ICP value showed significant improvement compared to in the Pathologic group (38.62 ± 6.53 vs. 31.29 ± 4.35; P = 0.028). We evaluated the ICP/MAP value in order to adjust for blood pressure. For ICP/MAP results, the Treatment group also showed improvement relative to the Pathologic group (0.28 ± 0.08 vs 0.18 ± 0.03; P = 0.028). We determined that there was significant difference between the two groups in the slope parameters (1.34 ± 0.19 vs 0.84 ± 0.13; P = 0.029).
Table 1
Comparative analysis of intracavernous pressure measurements in response to cavernous nerve electrostimulation
Western blot of cavernous tissue
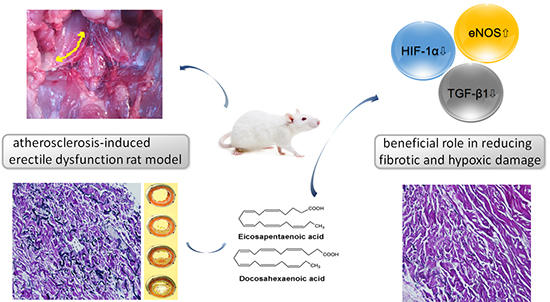
We performed a western blot on cavernous tissue and analyzed the results by using densitometry, which is a semi-quantitative method. The ratio divided as α-SMA are shown in Fig. 1. HIF-1α levels for the treatment group were lower than in the pathologic group (0.49 ± 0.24 vs. 0.95 ± 0.23, respectively). As expected, the lowest value was found in the control group. TGF-β1 level was highest in the pathologic group (0.48 ± 0.23). TGF-β1 was 0.42 ± 0.23 in the treatment group and 0.25 ± 0.09 in the control group. Expression of eNOS was higher in the treatment group than in the pathologic group (0.58 ± 0.24 vs 0.48 ± 0.10, respectively). The results revealed that systemically administered omega-3 fatty acids ameliorated the cavernosal molecular environment as shown by the decreased expression of TGF-β1 and HIF-1α, and overexpression of eNOS in the treatment group relative to the pathologic group.
Fig. 1
The protein expression of the experimental groups analyzed using western blotting. TGF-β1, transforming growth factor β1; HIF-1α, hypoxia induced factor 1α; eNOS, endothelial nitric oxide synthase. Alpha-smooth muscle actin (α-SMA) served as a control for the loading.
*P < 0.05, statistically significant difference between the pathologic group and omega-3 fatty acids treated group.

DISCUSSION
Our results, together with previous studies, suggest that by lowering oxidative stress and reducing the degree of cavernosal fibrosis, omega-3 fatty acids may protect from erectile dysfunction in a rat model of CPI. First, the end point for assessing erectile function is measurement of increased ICP and ICP/MAP using in vivo studies (1112). Second, the beneficial effect of the treatment was shown by a decreased in vitro expression of TGF-β1 and HIF-1α in our study when comparing the treatment group compared to the pathologic group.
We used a CPI model, which was made by inducing endothelial injury and applying a hypercholesterol diet. There are two mechanisms involved in establishing our pelvic ischemia model. One is impaired arterial inflow followed by secondary cavernosal dysfunction due to hypoxia, which have been proposed as possible mechanisms of atherosclerotic ED. It is known that TGF-β1 has an important role in this process. Another mechanism is the effect of endothelial injury, which represents a change in nitric oxide synthase (NOS). Nitric oxide (NO) is formed by NOS and affects erectile function owing to its role in smooth muscle relaxation. Several studies have shown that smooth muscle relaxation is induced by endothelial NOS and neuronal NOS, which is secreted from nonadrenergic noncholinergic nerves. When there is a problem in the metabolism of NO, impaired smooth muscle relaxation and hypoxic effects, due to platelet aggregation, appear (13).
ED is associated with a loss of smooth muscle cells, and an increase in fibrosis has been repeatedly reported in the corporal tissue of patients with ED (1415). The percentage of smooth muscle cells steadily decreases with age. Corporal tissue demonstrated excessive deposits of collagen fibers, which results in corporal fibrosis. These changes can also occur in the tunica media of the penile arteries (16).
Changes in elastic fibers or collagen types can result in mechanical alterations of the penis, which reduce its elasticity and compliance. In addition to these changes, postmortem studies have revealed that aging is associated with increasing degrees of atherosclerotic vascular alterations in the arterial bed of the penis. The exact pathophysiologic mechanism of ischemia-induced fibrosis of the corpus cavernosum is not clearly understood. However, in vitro studies have suggested that it is likely caused by hypoxia-induced overexpression of TGF-β1 (17).
TGF-β1 is a pleiotropic cytokine that has been shown to increase collagen synthesis in corpus cavernosum smooth muscle cells in vitro. Under ischemic conditions, TGF-β1 induces its own mRNA, leading to a further increase in TGF-β1 synthesis, which results in the development of severe fibrosis (17). In humans, a correlation between oxygen tension in the penis and the percentage of smooth muscle fibers has been demonstrated. The number of muscular fibers is therefore dependent on good oxygenation of the penis (18).
Ultimately, cavernosal fibrosis will result in corporal veno-occlusive dysfunction (CVOD), which is mainly due to failure of the corporal smooth muscle mass to achieve sufficient relaxation. This relaxation is necessary for passive veno-occlusion of the subtunical veins to occur. Therefore, any process that decreases the content or function of corporal smooth muscle, or ultimately causes corporal fibrosis, will increase the likelihood of the development of CVOD.
There is significant evidence that omega-3 fatty acids supplementation is beneficial in diseases involving ischemic injury (1920). Omega-3 fatty acid supplementation is reported to elevate superoxide dismutase and catalase activity in various organs such as the kidney, liver, and intestine (21). Several studies have also shown a decreased level of MDA with omega-3 fatty acids supplementation, after ischemic injury (22). These findings coincide with our results, which showed that TGF-β1 and HIF-1α concentrations in CPI rats given a daily administration of 200 mg/kg of omega-3 fatty acids were significantly lower than in the untreated CPI group.
Previous studies have shown that omega-3 fatty acids can decrease adhesion molecule expression in inflammatory cells and the endothelium (23). Production of inflammatory cytokines such as IL-6, IL-8, or TNF- α, which have been known to be up-regulated in CPI, decreased with exposure to omega-3 fatty acids in human and animal models (24). These results strengthen the evidence that omega-3 fatty acids work mainly through its anti-oxidant and anti-inflammatory properties.
It is becoming more evident that corporal fibrosis is the main underlying etiology for ED in the majority of patients (25). Regardless of age or etiology, 66% to 75% of cases of ED are caused by corporal fibrosis and ultimately, CVOD. Therefore, if the cause of CVOD itself can be prevented, then ED could become a preventable condition. The results of our study strengthen the evidence that omega-3 fatty acids work mainly through its anti-oxidant and anti-inflammatory properties and have an ameliorative function on fibrotic changes of cavernosum tissue.
Chronic atherosclerosis-induced pelvic ischemia induces impaired erectile function and altered protein expression. Administering omega-3 fatty acids could improve erectile function as shown by increases in ICP and the ICP/MAP ratio in the CPI treatment group. Additionally, omega-3 fatty acids have a beneficial role in reducing the pathophysiological consequences of fibrotic changes and the hypoxic damage to the cavernosal molecular environment, in a CPI model representing a vasculogenic ED model.
 XML Download
XML Download