

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Enterovirus 71 is one of the main causative pathogens of hand, foot and mouth disease. Compared to other enterovirus serotypes, enterovirus 71 more frequently involves the central nervous system (CNS), and induces diverse neurologic features such as brainstem encephalitis, aseptic meningitis, and acute flaccid paralysis (1,2). Since enterovirus 71 was first described in 1974, large-scale epidemics of enterovirus 71 infection have been reported in Asia-Pacific regions including Malaysia, Taiwan, and China and have caused many fatalities (3-6). Additional epidemics of hand, foot and mouth disease caused by enterovirus 71 that included fatal cases occurred in Korea between 2009 and 2013 (7-9).
Enterovirus 71 infection predominantly involves the brainstem. Most of the fatalities caused by enterovirus 71 infection result from autonomic dysfunction such as pulmonary hemorrhage in patients with brainstem encephalitis (1,2). Moreover, deaths usually occur within 6–24 hours after admission because the disease rapidly progresses to the critical stage (2,10). Hence, early diagnosis of enterovirus 71 infection with neurologic involvement and prompt, appropriate management is important.
To aid in the early detection of neurologic involvement in enterovirus 71 infection, we aimed to describe the diverse clinical features, magnetic resonance imaging (MRI) findings and cerebrospinal fluid (CSF) profiles of patients with neurologic complications associated with enterovirus 71 infection that were encountered during a 5-year period in a single Korean institute.
MATERIALS AND METHODS
Patients
We retrospectively reviewed the medical records of 31 children hospitalized with acute neurologic manifestations accompanied by confirmed enterovirus 71 infection at Ulsan University Hospital between January 2010 and December 2014. All patients included in this study were healthy prior to infection without neurologic problems. Of the 31 patients included in this study, 17 patients were included in our previous case series study and case report (11,12).
At the time of admission and during the hospitalization period, all patients were queried about, and observed for, the presence of myoclonus, tremor, ataxia, fever, vomiting, headache, seizure, irritability, lethargy, and decreased consciousness. Based on their clinical features, patients were classified into four clinical groups: 1) brainstem encephalitis characterized by myoclonus, tremor, ataxia, nystagmus, oculomotor palsies, bulbar palsy, and autonomic dysfunctions such as pulmonary edema, in various combinations, with or without neuroimaging evidence; 2) aseptic meningitis characterized by fever, headache, vomiting, and neck stiffness, without the other neurologic manifestations; 3) encephalitis characterized by decreased consciousness, seizure, and fever without myoclonus, tremor, ataxia, and autonomic dysfunction; and 4) acute flaccid paralysis characterized by acute onset motor weakness of the extremities.
Neurological and virological diagnostic tests
MRI was performed on either a 3.0 Tesla system (Intera Achieva; Philips, Best, The Netherlands) or a 1.5 Tesla system (Achieva; Philips). The protocol included T1-weighted images, T2-weighted images, fluid-attenuated inversion recovery (FLAIR) images, and contrast-enhanced T1-weighted images. Virus examinations were conducted with stool and CSF collected from the patients using real-time reverse transcription polymerase chain reaction (RT-PCR) at the Division of Enteric and Hepatitis Viruses, Korea Centers for Disease Control and Prevention. For genome detection and genotyping of the enterovirus, RT-PCR using Taq-Man technology was attempted on all stool and CSF samples obtained from patients. For genotyping, semi-nested RT-PCR was used to amplify part of the VP1 gene of the enterovirus based on the United States Centers for Disease Control and Prevention protocol for the detection of enterovirus by the use of confirmed enterovirus-positive specimens and real-time PCR. CSF analysis was performed to determine the white blood cell count, red blood cell count, levels of protein and glucose, and bacterial cultures.
RESULTS
Patient demographics and seasonal distribution
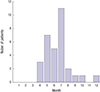
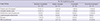
Eighteen patients were male and 13 patients were female. The age distribution is shown in Table 1. The mean age of the patients was 2.9 ± 5.5 years (range, 18 days to 12 years), and 80.6% of the patients were less than 4 years old. The majority of patients were 1 to 2 years old, accounting for 32.3% of the patients. The number of cases appearing per year was as follows: 8 cases appeared in 2010, 8 cases in 2012, 12 cases in 2013, and 3 cases in 2014. No cases appeared in 2011. As for the seasonal distributions, 10 cases (32.2%) developed in the spring (March–May), 18 cases (58.1%) in the summer (June–August), 2 cases (6.5%) in the autumn (September–November), and 1 case (3.2%) in the winter (December–February) (Fig. 1). The peak months for developing the disease were July (n = 11, 35.5%), May (n = 7, 22.6%), and June (n = 5, 16.1%).
Table 1
Age distribution and clinical diagnosis according to patients’ age
![]()
Virological analyses
Stool samples obtained from 30 patients and CSF samples from 15 patients were examined for enterovirus 71. All 30 stool samples were enterovirus 71-positive. Four of the CSF samples (26.7%) were enterovirus 71-positive.
Clinical features
All of the patients except one (96.8%) had a fever above 38°C, and 17 patients (54.8%) had body temperatures above 39°C. Twenty-five patients (80.6%) had a characteristic hand, foot and mouth disease rash before or during the neurologic symptoms. Neurologic symptoms or signs appeared within 4 days after the onset of skin lesions in the 25 patients that experienced the rash.
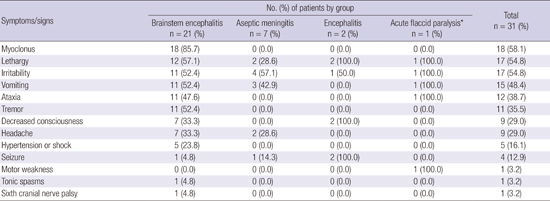
As mentioned above, the patients were classified into 4 clinical groups based on their clinical features: brainstem encephalitis (n = 21), meningitis (n = 7), encephalitis (n = 2), and acute flaccid paralysis (n = 1). The neurologic features presented by the patients in each of the 4 clinical groups are summarized in Table 2.
Table 2
Neurologic features of the patients in the four clinical groups
*The patient who was classified into the acute flaccid paralysis group also showed clinical features of brainstem encephalitis.
![]()
One patient who was classified as being in the acute flaccid paralysis group showed acute motor weakness of the right lower extremity in conjunction with clinical features of brainstem encephalitis such as ataxia. The most common neurologic features presented by the patients included myoclonus (n = 18, 58.1%), lethargy (n = 17, 54.8%), and irritability (n = 17, 54.8%). In the 21 patients with brainstem encephalitis, myoclonus (n = 18, 85.7%), ataxia (n = 11, 52.4%), and tremor (n = 11, 52.4%) occurred more frequently than they did in the patients of the other 3 groups due to the definitions for disease classification. Despite the low occurrence rate, some patients with brainstem encephalitis showed hypertension or hypotension (n = 5, 16.1%), tonic spasms (n = 1, 3.2%), and sixth cranial nerve palsy (n = 1, 3.2%). Three infants under 5 months of age who were classified into the aseptic meningitis group showed non-specific neurologic manifestations, such as lethargy and irritability along with fever, yet they revealed CSF pleocytosis and were enterovirus 71-positive (CSF and stool samples in two patients; stool sample in one patient). Seizures occurred in 4 patients (12.9%); of these, 2 patients were included in the encephalitis group, while the other 2 patients were included in the aseptic meningitis and brainstem encephalitis groups, respectively. The two patients included in the aseptic meningitis and brainstem encephalitis groups were 17 months and 19 months of age, respectively, and showed typical features of febrile seizures, which were generalized seizures lasting 2–3 minutes accompanied by high fever.
MRI findings
MRI was performed on 25 patients. The locations of the lesions in the MR images for all 4 clinical groups are summarized in Table 3. Fourteen (56.0%) of the 25 patients revealed increased signal intensity in the posterior region of the brainstem (the pons in 12 patients, and the pons and midbrain in 2 patients) and bilateral cerebellar dentate nuclei on T2-weighted and FLAIR images (Fig. 2A and B). Two patients (8.0%), who both had seizures, revealed leptomeningeal enhancement of the cerebral hemispheres without brain parenchymal lesions (Fig. 2C). Eight patients (32.0%) showed no apparent abnormalities. None of the patients had abnormalities in brain regions outside the brainstem and cerebellum. Twelve (57.1%) of the 21 patients presenting with clinical brainstem encephalitis revealed the characteristic lesions in the dorsal brainstem and bilateral cerebellar dentate nuclei on brain MR images. One additional patient (4.8%) showed leptomeningeal enhancement of the cerebral hemispheres and the remaining 7 patients (33.3%) had no abnormalities. MRI could not be performed in 1 patient with clinical brainstem encephalitis (4.8%) due to the patient’s very critical condition including pulmonary hemorrhage and acute heart failure. In the 2 patients with clinical encephalitis, one showed leptomeningeal enhancement of the cerebrum without focal brain lesions, while the other patient, who presented with decreased consciousness, lethargy, irritability, and seizure, had lesions in the dorsal brainstem and bilateral cerebellar dentate nuclei. One patient with the clinical features of acute flaccid paralysis and brainstem encephalitis revealed contrast-enhancement of the bilateral ventral nerve roots at the lumbar spine level on spine MR images, as well as abnormalities in the dorsal pons and cerebellar dentate nuclei on brain MR images. One patient with clinical aseptic meningitis displayed a small lesion in the left dorsal pons. Ten (71.4%) of the 14 patients who displayed lesions in the bilateral dentate nuclei of the cerebellum on brain MR images exhibited ataxia. The remaining 4 patients (28.6%) did not show ataxia. Two (18.2%) of the 11 patients with ataxia revealed no cerebellar lesions on brain MR images. Three (20%) of 15 patients with brainstem and cerebellar lesions in MR images and 2 (25%) of 8 patients with no abnormality in MR images were managed in the intensive care unit. In 7 of the 14 patients with brainstem and cerebellar lesions on brain MR images, follow-up brain MRI was performed between 7 days and 1 month after the first images were obtained. All of the follow-up MR images revealed apparent improvement compared to the initial images.
Table 3
Locations of lesions in magnetic resonance images in the patients of the four clinical groups
*The patient who was classified into the acute flaccid paralysis group showed simultaneous lesions in the brainstem and spinal cord on MRI; †Two of 14 patients who showed brainstem lesion in MR images had lesions in the pons and midbrain, while the other 12 patients had lesion only in the pons.
![]()
 | Fig. 2Magnetic resonance imaging findings in the brain. Note the high signal intensity lesion in the posterior portion of the pons and bilateral dentate nuclei of the cerebellum on the axial T2-weighted images in (A) and (B) (arrows). Note the leptomeningeal enhancement of both cerebral hemispheres on contrast-enhanced T1-weighted images in (C) (arrowheads).
|
CSF findings
Routine CSF analysis was performed in 30 patients. CSF examination was not conducted in one patient because the patient’s parents refused the examination. The CSF findings of the patients in each of the 4 clinical groups are summarized in Table 4. Twenty-six patients (86.7%) showed CSF pleocytosis (range, 28 to 900 cells/mm3), whereas four patients (13.3%) revealed no pleocytosis (range, 0 or 1 cells/mm3). Sixteen patients (53.3%) revealed mild pleocytosis (10–100 cells/mm3). The mean protein level was 48.4 mg/dL (range, 10.9 to 130.9 mg/dL), and 11 patients (36.7%) showed increased protein levels (> 50 mg/dL). The mean glucose level was 66.7 mg/dL (range, 46 to 149 mg/dL).
Table 4
Cerebrospinal fluid findings in the patients of the four clinical groups

![]()
Treatment and outcomes
We considered administration of intravenous immunoglobulin to patients with suspected enterovirus 71 infection who showed 1) apparent abnormal neurological signs such as decreased consciousness, acute motor weakness, ataxia, and daytime myoclonus; 2) lesions of brainstem, cerebellum, and spinal cord in MR images; 3) CSF pleocytosis; or 4) prolonged high fever (> 38.5°C for more than 2 days after hospitalization) despite symptomatic treatment. However, despite satisfying the aforementioned conditions, intravenous immunoglobulin administration was not considered in cases that showed 1) rapid improvement of abnormal neurological sign and symptoms and fever in response to symptomatic treatment after admission and 2) relatively good general condition with signs of aseptic meningitis such as headache, vomiting, and neck stiffness without other neurologic manifestations. Milrinone was administered when patients had hypertension as well as hypotension.
Intravenous immunoglobulin was administered in 17 patients. The other 14 patients were managed symptomatically. Five patients (16.1%) with hypertension or acute heart failure were managed with intravenous milrinone. In all 4 groups, the number of patients treated with intravenous immunoglobulin was as follows: 14 (66.7%) of 21 patients with clinical brainstem encephalitis, 1 (14.3%) of 7 patients with aseptic meningitis, 1 (50%) of 2 patients with encephalitis, and 1 patient (100%) with acute flaccid paralysis. Milrinone was administered to 5 (23.8%) of 21 patients with brainstem encephalitis. The mean time from admission to disappearance of fever was 2.5 days (range, 1–8 days) and 2.3 days (range, 1–5 days) in patients treated with intravenous immunoglobulin and those managed symptomatically, respectively. The mean duration of hospitalization was 9 days (range, 5–17 days) and 5.6 days (range, 3–10 days) for these 2 groups, respectively. The mean time from administration of intravenous immunoglobulin to disappearance of fever was 1.4 days (range, 1–2 days). Twenty-seven patients (96.8%) recovered completely without neurologic deficits, whereas one patient (3.2%) with brainstem encephalitis died due to pulmonary hemorrhage, acute heart failure and shock within 15 h after admission to the emergency department, despite aggressive management including intravenous immunoglobulin, milrinone and empirical antimicrobial therapy.
DISCUSSION
In the present study, the clinical features we noted in patients with neurologic complications of enterovirus 71 infection were mostly concordant with the findings of previous studies (1,2,13-15). The majority of patients with neurologic complications related to enterovirus 71 were under the age of 4 years. The peak seasons of the disease were late spring to summer. The patients mostly had a high fever above 38°C and the characteristic skin rash of hand, foot and mouth disease before or during the neurologic manifestations. The characteristic clinical features of enterovirus 71 brainstem encephalitis such as myoclonus, ataxia, and tremor also often appeared, as reported in previous studies.
Brainstem encephalitis is the most critical presentation of CNS involvement in enterovirus 71 infection because it can cause pulmonary hemorrhage/edema, which may lead to death (10,14). Although several hypotheses, such as the presence of receptors for enterovirus 71 in the brainstem that induce tissue tropism, have been proposed, the pathophysiology is currently unknown (2). In this study, brainstem encephalitis was the most common neurologic manifestation of enterovirus 71 infection. Enterovirus 71 brainstem encephalitis has been defined as an illness characterized by myoclonus, ataxia, nystagmus, oculomotor palsies, and bulbar palsy, in various combinations, with or without confirmation by neuroimaging in conjunction with virus isolation from at least one site (throat swab, stool, CSF, or others) (15,16). Whereas many studies have documented that brainstem encephalitis is the most common neurologic complication of enterovirus 71 infection, as described in this study (2,3,15), other studies have reported that aseptic meningitis is the most common complication (13,17). These differences may result from the level of detail acquired when obtaining a patient’s medical history or from the level of observation regarding the presence of clinical symptoms such as myoclonus and tremor, since enterovirus 71 brainstem encephalitis is diagnosed based on clinical features even without neuroimaging, as mentioned above. Myoclonus in patients with enterovirus 71 brainstem encephalitis occurs during wakefulness and deep sleep, as well as light sleep, and may appear frequently, unlike sleep myoclonus (13,18). Myoclonus is not only the most common symptom, but is also associated with disease severity and a higher incidence of neurologic sequelae in children with enterovirus 71 infection (12,14,16). The brainstem is known as one of the origin sites for myoclonus. Brainstem myoclonus typically presents as generalized myoclonus, and particularly affects the upper body in response to sudden unexpected stimuli (19). It often begins in the sternocleidomastoid and trapezius muscles, and propagates rostrally to the brainstem-innervated cranial muscles and down the spinal cord (20). Nevertheless, many physicians and parents often overlook it as a non-specific symptom of febrile illnesses in children with hand, foot and mouth disease by enterovirus 71 infection, which may possibly lead to misdiagnosis of aseptic meningitis instead of brainstem encephalitis. Hence, all patients with suspected enterovirus 71 infection should be queried or carefully observed for all clinical symptoms such as myoclonus and ataxia for early detection of CNS involvement, since significant differences in the outcome may exist between patients with brainstem encephalitis and aseptic meningitis.
The characteristic MRI findings of enterovirus 71 brainstem encephalitis are high signal intensities on T2-weighted and FLAIR images in the posterior portion of the pons, medulla oblongata, midbrain, and bilateral dentate nuclei of the cerebellum, although the MR images may be normal (1,21). In children with acute flaccid paralysis, MR images typically show high signal lesions in the anterior horn cells of the spinal cord on T2-weighted images, and contrast-enhanced ventral root on T1-weighted images (22,23). Although the clinical features are positively correlated with MRI findings (21,22,24), they are not necessarily consistent with MRI findings (11). The present study also showed the characteristic clinical features of enterovirus 71 CNS involvement together with the typical MRI findings in many patients. However, MRI findings were not necessarily correlated with the neurologic symptoms and signs.
Although isolation of enterovirus 71 from the CSF is confirmatory of CNS infection by enterovirus 71, unlike other enteroviruses, the detection rate of enterovirus 71 in the CSF of patients with neurologic disease is very low (0–10%) (1). Enterovirus 71 is isolated mainly from throat or stool specimens, and occasionally from skin vesicle fluid (2). Nevertheless, CSF examination is essential in patients who have suspected CNS involvement associated with enterovirus 71 infection, since most patients with neurologic complications revealed CSF pleocytosis (1). Mild lymphocytic pleocytosis of 10–100 cells per μL is typical, but occasionally pleocytosis is not observed. This study also showed a high rate (86.7%) of CSF pleocytosis, despite a low viral detection rate from the CSF.
Antiviral therapy is currently ineffective for treating enterovirus 71 infection (25). In patients with severe neurologic complications of enterovirus 71 infection, such as brainstem encephalitis, intravenous immunoglobulin and milrinone treatment are recommended (2). Intravenous immunoglobulin therapy provides neutralization antibodies, decreases sympathetic outflow and attenuates cytokine production. Milrinone is a drug for congestive heart failure, and has both inotropic and vasodilator properties (26). A recent prospective, open-label, randomized controlled study showed that patients who were treated with intravenous milrinone (0.5 μg/kg/min) and intravenous immunoglobulin had a lower 1-week mortality rate compared to patients who were treated with dopamine or dobutamine and intravenous immunoglobulin (18.2% vs. 57.9%) (27).
This study showed low mortality and morbidity rates compared to previous studies (1,2,4,5). CNS involvement in enterovirus 71 infection accompanied with cardiopulmonary failure is associated with a high mortality rate during the acute stage of the infection (30–40%) and a poor long-term prognosis (28-30), whereas CNS involvement without cardiopulmonary failure is associated with good short- and long-term outcomes (30). Although the reasons for the low incidences of cardiopulmonary failure and fatality in this study are unclear, the size of the epidemic, differences in the enterovirus 71 subgenotypes during epidemics, absence of medulla oblongata lesion in MR images, treatment with intravenous immunoglobulin and milrinone, environmental factors such as climate, and the ethnicity or genetic background of the patients may affect the mortality and morbidity rates.
This study has several limitations. Since this was a retrospective study performed at a single institute, ascertainment bias may have occurred. In addition, because this was not a case-control study, more severely affected patients were managed with intravenous immunoglobulin and milrinone, whereas relatively mildly affected patients were managed symptomatically. Hence, we cannot say to what degree the intravenous immunoglobulin and milrinone treatments contributed to the low mortality and morbidity rates observed in this study, although these are known to be efficient treatments.
In conclusion, this study demonstrated that brainstem encephalitis was the most common neurologic manifestation of enterovirus 71 infection. Identification of the characteristic clinical symptoms such as myoclonus, ataxia, tremor, CSF pleocytosis, and brainstem lesions on MR images is pathognomonic for the early diagnosis of enterovirus 71 infection with neurologic involvement. Early diagnosis and management of enterovirus 71 infection with CNS involvement may reduce the mortality and morbidity rates of patients with the disease.
 XML Download
XML Download