

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Atrial fibrillation (AF) is the most common cardiac arrhythmia requiring medical therapy and is associated with an increased risk of ischemic stroke, embolic events, congestive heart failure, impaired quality of life, and death (1-5). However, AF is often asymptomatic and frequently diagnosed for the first time on admission for stroke management (6). Therefore, early diagnosis and proper management are important for prevention of cardiovascular complications of AF.
Premature atrial contraction (PAC) is frequently observed in clinical practice, and often considered a benign condition (7-9). However, frequent PACs have been reported to be associated with an increased risk of new occurrence of AF and adverse cardiovascular outcomes (10-12). Prolonged PR interval, which is a component of the Framingham risk score for AF, is also reported to be associated with increased risk of AF, pacemaker implantation, congestive heart failure, and all-cause mortality (13-15). A large prospective cohort study reported that neither mortality nor hospitalization rates due to coronary artery disease, heart failure, AF, or stroke was associated with prolonged PR interval (16). However, there has been no report addressing the association between prolonged PR interval and AF occurrence rate in patients with frequent PACs. In this study, we investigated whether prolonged PR interval could predict new occurrence of AF in patients with frequent PACs.
MATERIALS AND METHODS
Study population
In our study, we enrolled the patients with frequent PACs. Frequent PACs were defined as more than 100 PACs/day in 24-hour Holter monitoring at least two times in order to compensate the day-to-day variation. We retrospectively reviewed the medical records of 2,713 patients who performed 24-hour Holter monitoring at least two times at Samsung Medical Center from April 1999 and June 2008. Among these, a total of 967 patients had more than 100 PACs/day in all repeated Holter monitoring. Exclusion criteria were previously documented AF or atrial flutter, structural heart disease (atrial septal defect; ventricular septal defect; patent ductus arteriosus, and hypertrophic cardiomyopathy), history of congestive heart failure, high-grade atrioventricular block, presence of pacemaker or implantable cardioverter defibrillator (ICD), rheumatic heart disease, moderate-to-severe heart valve disease, and any mechanical or bioprosthetic heart valve. We also excluded patients who had taken any antiarrhythmic drug within five days and those who had taken amiodarone within two months. During enrollment, 76 patients (11%) used beta blockers (BBs) and 104 patients (15%) used calcium channel blockers (CCBs). We did not exclude the patients with coronary artery disease without evidence of myocardial infarction.
Study design and end point
Demographic data, cardiovascular risk factors, medications, and indications for 24-hour Holter monitoring were analyzed by medical records review. Patients were divided into two groups according to baseline PR interval: group A (normal PR interval group) and group B (prolonged PR interval group). Prolonged PR interval was defined as baseline PR interval > 200 msec. The primary end point was new occurrence of AF as evaluated from the medical records of our hospital. New occurrence of AF was defined as AF documented by 12-lead electrocardiogram (ECG) or Holter monitoring during follow-up.
ECG, transthoracic echocardiography (TTE), and 24-hour Holter monitoring analysis
A baseline resting ECG performed within 30 days of Holter monitoring was analyzed to provide baseline rhythm and PR interval. The PR interval was automatically measured by the ECG system or manually measured using customized software (Cardio Calipers, version 3.3, Iconico, Inc., New York, NY, USA). TTE data, which was performed within three months, were also analyzed. The left ventricular (LV) end-diastolic dimension, LV end-systolic dimension, left atrial (LA) dimension, and left ventricular ejection fraction (LVEF) were estimated. All Holter monitoring data were analyzed by two independent cardiologists to provide the frequency of PACs and the presence of other arrhythmia. Patients with insufficient Holter monitoring data were excluded.
Statistics
Continuous variables are expressed as the mean ± standard deviation or median and interquartile range. Categorical variables are expressed as frequency and percentage. To evaluate difference according to PR interval, we used Student’s unpaired t test for normally distributed data and Mann-Whitney test for skewed data. Categorical variables were analyzed with chi-square test or Fisher’s exact tests. A Kaplan-Meier and log-rank test was used to compare AF-free survival distributions between study groups. Cox regression analysis was used to calculate the hazard ratios (HR) and 95% confidence intervals (CI) of new-onset AF. Calculations were performed using SPSS software (SPSS for Windows, version 20.0, IBM Corp., Armonk, NY, USA). A P value of < 0.05 was considered to be significant.
RESULTS
Among 967 patients with more than 100 PACs/day, 133 had previously documented AF or atrial flutter, 74 had structural heart disease, 18 had permanent pacemakers, and 56 were lost to follow-up. A total of 684 patients (335 males, mean age 61.8 ± 15.0 years) were finally analyzed in this study (Fig. 1). The median number of PACs was 2,558 beats/day (inter-quartile range: 1,213–5,409 beats/day).

Baseline clinical characteristics of the study population
The median PR interval was 166 msec (interquartile range: 153–179 msec). Fifty-eight patients had a PR interval longer than 200 msec at baseline ECG. Clinical characteristics of the patients according to PR interval are summarized in Table 1. The mean age was significantly older (P = 0.007) and proportion of male was higher (P = 0.004) in group B. The prevalence of hypertension was also higher in group B (P = 0.002). The use of BBs and CCBs which could affect the heart rate did not differ between the groups A and B (11% vs. 12.1%, P = 0.808; 15.0% vs. 17.2%, P = 0.652, respectively). Mean heart rate was not also different (P = 0.118). The prevalence of diabetes, dyslipidemia, and coronary artery disease were not significantly different between the two groups. Mean LA dimension as determined by TTE was larger in group B (P = 0.025). The number of PACs and the LVEF were not significantly different between the two study groups.
Table 1
Baseline characteristics of the study groups
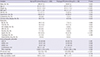
BMI, body mass index; DM, diabetes mellitus; BB, beta blocker; CCB, calcium channel blocker; ACE, angiotensin converting enzyme; ARB, angiotensin receptor blocker; LVEF, left ventricular ejection fraction; LVEDD, LV end-diastolic dimension; LVESD, LV end-systolic dimension; LA, left atrium; PAC, premature atrial contraction.
Factors predicting new occurrence of AF
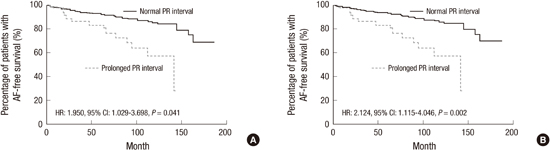
During a mean follow-up period of 59.3 ± 51.7 months, 50 patients (8.0%) in group A and 14 patients (24.1%) in group B developed new-onset AF (P < 0.001). Duration of follow-up was not significantly different between groups A and B (P = 0.130). Mean duration from initial Holter monitoring to new-onset AF was 52.9 ± 45.5 and 57.6 ± 41.5 months in groups A and B, respectively (P = 0.601). Table 2 shows the clinical characteristics according to new occurrence of AF. Univariate analysis revealed that age, hypertension, LA dimension, and prolonged PR interval were associated with new occurrence of AF. Kaplan-Meier estimates of new-onset AF-free survival according to PR interval are demonstrated in Fig. 2A (log rank P < 0.001). Cox regression analysis showed that age (HR, 1.033; 95% CI, 1.006–1.060; P = 0.015), prolonged PR interval (HR, 1.950; 95% CI, 1.029–3.698; P = 0.041), and LA dimension (HR, 1.061; 95% CI, 1.012–1.112; P = 0.015) were independent predictors of new occurrence of AF (Table 3). The receiver operating characteristic (ROC) curve analysis showed that PR interval longer than 200 msec predicted the development of AF with a sensitivity of 78% and a specificity of 93% (area under curve = 0.581).
Table 2
Clinical characteristics of patients according to new occurrence of atrial fibrillation
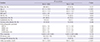
Fig. 2
Kaplan-Meier estimate of new-onset AF-free survival in patients with frequent PACs (A) and in patients with frequent PACs who received follow-up for more than one year (B). AF, atrial fibrillation; PAC, premature atrial contraction; HR, hazard ratio; CI, confidence interval.

Table 3
Multivariate analysis of the new occurrence of atrial fibrillation

Subgroup analysis of patients who received follow-up for more than one year
We conducted a subgroup analysis of 489 patients who received follow-up for more than one year (mean 82.0 ± 43.7 months). Mean duration of follow-up was 82.4 ± 44.0 and 78.9 ± 42.1 months in groups A and B, respectively (P = 0.717). Kaplan-Meier estimates of new-onset AF-free survival according to PR interval are shown in Fig. 2B (log rank P < 0.001). In this subgroup, Cox regression analysis showed that age (HR, 1.041; 95% CI, 1.013–1.069; P = 0.004), prolonged PR interval (HR, 2.124; 95% CI, 1.115–4.046; P = 0.022), and LA dimension (HR, 1.051; 95% CI, 1.001–1.102; P = 0.044) were independent predictors of new occurrence of AF (Table 4).
Table 4
Multivariate analysis of new occurrence of atrial fibrillation in patients who received follow-up for more than one year

DISCUSSION
We investigated whether prolonged PR could predict new occurrence of AF in patients who experienced more than 100 PACs/day. Two prospective studies previously reported that frequent PACs were an independent predictor of new occurrence of AF (11,17). In these two studies, frequent PACs were defined as more than 100 and 720 PACs/day, respectively. Additionally, two large prospective cohort studies recently reported that prolonged PR interval is associated with increased risk of new occurrence of AF (14,18), pacemaker implantation (14), and all-cause mortality (14). A meta-analysis also revealed the similar result (19), and another prospective cohort study reported that prolonged PR interval is associated with heart failure and death in patients with stable coronary artery disease (13). However, most of these previous studies evaluated the prognostic significance of prolonged PR interval in the general population. None of previous studies addressed whether prolonged PR interval also could predict new occurrence of AF, especially in patients with frequent PACs.
Our main finding is that, in patients with frequent PACs, the prolonged PR interval is associated with new occurrence of AF and is an independent surrogate marker of AF development. Enlarged LA dimension and advanced age, known risk factors for AF, were also independent predictors in this study.
There are several potential mechanisms to explain the association between prolonged PR interval and new occurrence of AF. First, PR interval is influenced by the autonomic nervous system (20). Several studies have reported that both the sympathetic and parasympathetic nervous systems play a role in AF development (21,22). Prolonged PR interval might represent an abnormality of the cardiac autonomic nervous system. Second, PR prolongation can be explained by aging of the atrial myocardium and its conduction system, which is in line with AF genesis. It was previously reported that PR interval increased with age due entirely to prolongation of the interval between P wave onset and His bundle potential (23). Third, a meta-analysis of genome-wide association studies reported that chromosome loci from voltage-gated sodium channel genes and cardiac developmental genes were associated with PR interval, and five of the loci were also associated with AF (24). That study supports a possible shared genetic background between PR interval and AF.
Recently, there have been great advances in understating the pathophysiology of AF. Several studies have suggested that ectopic beats originating from the pulmonary vein (PV) initiate AF (25,26). Yamane et al. (27) reported that the number of PAC significantly decreases after successful PV isolation in patient with paroxysmal AF. Moreover, AF recurrences after PV isolation are associated with an increased the number of PAC in that same study (27). These findings indicate that PACs are a potent predictor of AF occurrence. In ischemic stroke patients without known AF, frequent PACs (PACs ≥ 70; forth quartile) are associated with a higher incidence of AF (28,29). A prospective study reported that frequent PACs are independent predictors for new AF in patients who complain of palpitation, dizziness, or syncope (11).
Until now, the factors that predict AF occurrence in patients with frequent PACs were unknown. Thus, we sought to investigate the factors that could predict AF in patients with frequent PACs. Our findings are not consistent with previous results regarding PACs. In our study, we did not find any association between the number of PACs and AF occurrence in patients with more than 100 PACs/day. The median values of PAC in all patients were 2,558 PACs/day, and median values in patients with or without AF development were not significantly different. We presumed that our patients might be more susceptible to the development of AF than average. Our cumulative incidence rate of AF was actually higher than previously reported (14,18), which supports the increased susceptibility of our study population to AF development. In other words, PAC burden itself was not associated with AF occurrence in patients with increased susceptibility for AF in this study population. The susceptibility of our study population to AF might confound the association between PAC and AF development compared to previous studies. Ultimately, we found that prolonged PR interval was an independent predictor of AF occurrence in patients with frequent PACs, which is also a potent risk factor for AF. In other words, a decrease in PACs burden is not the only solution to prevent the development of atrial fibrillation in the patients with frequent PACs with prolonged PR interval. The clinical implication of this study is that if a patient has frequent PACs (> 100 PACs/day) with prolonged PR interval on routine examination, we should observe this patient carefully at an outpatient clinic.
There are several limitations to our study. First, this study was a retrospective observational study and so we could not control for confounding factors. For example, although there was no statistical significant difference between study groups, we could not completely capture patient history of drugs that might affect PR interval, such as beta blockers and calcium channel blockers. Second, although we defined the number of frequent PACs base on previous studies, the definition is arbitrary. Third, a 24-hour Holter monitor was used to determine PAC burden. A longer duration of monitoring might be preferable because of day-to-day variability in PAC frequency, especially in the presence of frequent PAC burden of more than 100 beats/day. Whenever feasible, ambulatory monitoring for at least 48 hour is preferable.
In conclusion, our findings suggest that prolonged PR interval, advanced age, and enlarged LA dimension are associated with new occurrence of AF in patients with frequent PACs.
 XML Download
XML Download