

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Infection is the leading cause of morbidity and mortality in multiple myeloma (MM), in which 26%–45% of early deaths are attributable to infection (1,2). Infection is not only the direct cause of death but also affects disease progression due to the delaying of planned anti-myeloma therapy. The risk of bacterial infection increases 7-fold in patients with MM compared with matched controls (2), and the increased susceptibility to infection is due to disease-related immune deficits on innate and adaptive immune system including hypogammaglobulinemia (3,4), renal failure (3), treatment-related toxicities (4,5), and the use of high-dose corticosteroid therapy (6).
The treatment of MM has undergone a paradigm shift with the use of immunomodulatory drugs (thalidomide, lenalidomide, and pomalidomide) and proteasome inhibitors (bortezomib) (7). The effects of these drugs on the immune system are distinct from those of conventional anti-myeloma agents. In addition, these drugs are usually used in combination with high-dose dexamethasone, resulting in impairment of cell-mediated immunity. Therefore, the types and patterns of infections have changed by the administration of these novel agents. Bortezomib suppresses essential T-cell mediated immune responses by inhibiting the functions of human CD4+ T cells (8,9), reducing antigen presentation by CD8+ T cells, and reducing the cytotoxic T cell response (10). Consequently, the incidence of varicella zoster virus infection increased in patients treated with bortezomib-based regimens compared with those treated with melphalan plus prednisone (11) or with high-dose dexamethasone (12). In contrast to viral infections, the incidence of bacterial infections was similar (10%–13%) (11,13) to that of regimens with melphalan plus prednisone (7%–10%) (14,15) but lower than that of regimens with intensive chemotherapeutic agents such as VAD (vincristine, doxorubicin, and dexamethasone) (14%-27%) (16,17) and DCEP (dexamethasone, cyclophosphamide, etoposide, and cisplatin) (7.5%–22.5%) (18).
As the types and patterns of infections change, the risk factors for severe bacterial infection (SBI) in the MM patients treated with bortezomib-based regimens may be different from previously known risk factors. The risk of bacterial infection increased in the early period of treatment with high tumor burden and decreased with a favorable response because of the restoration of the immune deficit (16). Therefore, a comprehensive pretreatment assessment of the risk factors for SBI in each treatment course can discriminate the patients at increased risk of SBI and allow the application of patient-oriented prophylactic and therapeutic approaches for SBI.
In this study, we analyzed the various clinical and laboratory parameters that were associated with infectious complications to determine the risk factors for SBI in 98 MM patients treated with bortezomib-based regimens during 427 treatment courses.
MATERIALS AND METHODS
Patient eligibility
A total of 98 consecutive patients diagnosed with MM and who were treated with upfront or salvage bortezomib-based treatments in the Severance Hospital between January 2006 and December 2012 were included. In the cases of patients treated with more than one bortezomib-based regimen as a different line of therapy, we used only the data related to the first bortezomib-based regimen. This study was approved by the Institutional Review Board of the Severance Hospital.
Treatment protocol and schedule
We retrospectively analyzed the data of 427 bortezomib treatment courses in 98 MM patients. Of the 98 MM patients, 58 patients received bortezomib (1.3 mg/m2 intravenously [i.v.] on days 1, 4, 8, and 11) and dexamethasone (40 mg/day on days 1–4) every 3 weeks (VD regimen). Twenty-five patients received bortezomib (1.3 mg/m2 i.v. on days 1, 4, 8, 11, 22, 25, 29, and 32 during courses 1 to 4 and on days 1, 8, 22, and 29 during courses 5 to 9), melphalan (9 mg/m2 via oral route on days 1–4), and prednisolone (60 mg/m2 via oral route on days1–4) every 6 weeks (VMP regimen). To simplify the statistical analysis, one VMP regimen was divided into 2 courses, each with a 3-week schedule, and the VMP regimen variables presented are based on 1 course with a 3-week schedule. Fifteen patients received bortezomib (1.3 mg/m2 i.v. on days 1, 4, 8, and 11), doxorubicin (9 mg/m2 i.v. on days 1–4), and dexamethasone (40 mg on days 1–4) every 3 weeks (PAD regimen). Antibacterial prophylaxis was not routinely administered but a prophylactic antibacterial agent (ciprofloxacin or levofloxacin) was used in 70.4% of the patients and a prophylactic antifungal agent (fluconazole) was used in 64.3% of the patients before or immediately after starting chemotherapy according to each physician’s decision. No patient received antiviral prophylaxis in this study.
Definitions
We investigated infectious complications and treatment-related toxicities within 1 month after each bortezomib course and the data from that period were analyzed. Chemotherapy-related toxicities were graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events (CTCAE) version 4.0. SBI was defined as grade 3–5 infection of each system or neutropenic fever. We divided patients into two groups: 1) the SBI group, composed of patients who developed SBI during the bortezomib treatment, 2) the non-SBI group, composed of patients who did not develop SBI during the bortezomib treatment. SBI was classified into three categories: 1) clinically documented infection (CDI), for the cases in which clinical signs and symptoms of infection were present although the culture results were negative, 2) microbiologically documented infection (MDI), for the cases in which pathogens were isolated from a blood sample or other cultures, 3) fever of unknown origin (FUO), for the cases in which fever was the only sign of infection. In defining CDI and FUO, the episodes which were highly suspicious for bacterial infection were included and documented viral or fungal infections were excluded. Lymphopenia was defined as an absolute lymphocyte count (ALC) of < 1.0 × 109/L. Mortality was defined as infection-related death regardless of refractory or progressive disease.
Response to treatment was assessed according to the International Myeloma Working Group uniform response criteria (19). Progression-free survival (PFS) after bortezomib treatment was measured from the initial date of bortezomib treatment to the date of progression or the final follow-up visit without progression or the date of death. Overall survival (OS) after bortezomib treatment was measured from the initial date of bortezomib treatment to the final follow-up date or the date of death from any cause.
Statistical analysis
To identify the risk factors for the development of SBI during bortezomib treatment, we analyzed the variables using two approaches: 1) analysis of the patients who developed SBI during a specific period of treatment (total, 2 courses, or 3 months), or 2) analysis of each bortezomib treatment course.
Continuous variables were compared using Mann-Whitney U test and categorical variables were compared using χ2 test or Fisher's exact test. Univariate analysis for the factors that affected the development of SBI was performed using a logistic regression method. The factors with P < 0.1 were selected and included in the multivariate logistic regression analysis. Potential confounding factors and multicollinearity were evaluated, and the factors strongly associated with other significant factors were excluded from the multivariate analysis. The survival curves were calculated using the Kaplan-Meier method and were compared using the log-rank test. A P value of < 0.05 was defined as statistically significant. All statistical calculations were performed with the PASW software version 20.0 (IBM Corp., Armonk, NY, USA).
RESULTS
Patient characteristics
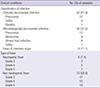
The clinical characteristics of the 98 patients are summarized in Table 1. Ninety-eight patients received a median of 4 treatment courses (range, 1–15) of bortezomib-based chemotherapy and a total of 427 bortezomib courses. Most of the clinical characteristics were not significantly different between the SBI group and the non-SBI group except the performance status.
Table 1
Clinical characteristics of the 98 patients undergoing chemotherapy with the bortezomib-containing regimen

Continuous variables are presented as median (range). *Missed data in 7 patients; †Missed data in 3 patients; ‡Missed data in 35 patients. SBI, severe bacterial infection; ECOG, Eastern Cooperative Oncology Group; ISS, International Scoring System.
![]()
Infection profile
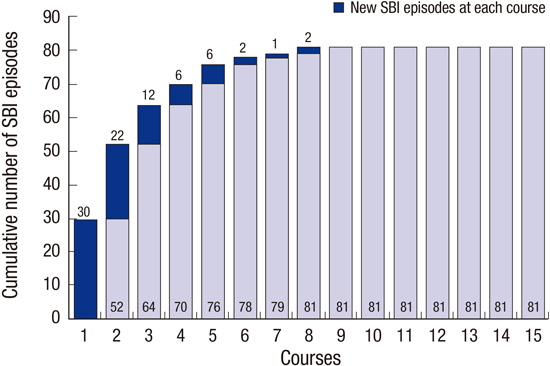
Infection development was assessed in each patient and for each treatment course. Of the 98 patients, SBI was observed in 56 (57.2%) patients, and 18 (18.3%) patients developed SBI more than once. Of the 427 treatment courses, 81 SBI cases occurred and the incidence of SBI per treatment course was 19.0%. Reactivation of herpes zoster viruses developed in 13 (13.3%) patients and in 14 (3.0%) treatment courses. Fungal infections, defined as proven or probable invasive fungal disease, developed in 13 (13.2%) patients and in 18 (4.2%) treatment courses. Most of the SBI episodes (79.0%) occurred in the first 3 courses and no SBI episode was observed after the 8th course (Fig. 1).
 | Fig. 1Number of severe bacterial infections (SBI) episodes during treatment with the bortezomib-based regimens. Cumulative numbers of SBI are presented at the bottom of the bars, and numbers of SBI episodes at each course are presented at the top of the bars.
|
Of the 81 SBI episodes, 42 (52.5%) were CDI, 30 (37.0%) were MDI, and 9 (11.1%) were FUO (Table 2). Pneumonia was the most common type of infection in both CDI and MDI and accounted for 60.5% of the SBI episodes, and both bacteremia (n = 9) and urinary tract infection (n = 8) were frequently observed. In addition, non-neutropenic fever was frequently observed (n = 75) whereas neutropenic fever accounted for only 6 episodes (7.4%). Most of the SBI episodes (62 of 81) were appropriately treated with systemic antibiotics although the subsequent bortezomib courses were postponed in 31 episodes and interrupted in 9 episodes. Among total 19 patients died during the bortezomib-based treatment (19.3% of overall mortality rate), 12 patients died from infection with at least partial response to bortezomib and 7 patients died from infection in progressive or refractory status.
Table 2
Eighty-one episodes of severe bacterial infections during chemotherapy with the bortezomib-containing regimens
![]()
Variable pathogens were identified in 30 MDI cases. Gram-negative bacteria (n = 21) were more prevalent than gram-positive bacteria (n = 9). Acinetobacter baumannii (n = 6), Escherichia coli (n = 5), Klebsiella species (n = 4), coagulase-negative Staphylococci (n = 4), and Staphylococcus aureus (n = 3) were common pathogens.
Risk factors for developing SBI in 98 MM patients
To identify the risk factors for developing SBI in 98 patients, three types of analysis were introduced in this study. An analysis of the risk factors was performed 1) during the total period of bortezomib-based treatment, 2) within 3 months from initiation of therapy, and 3) in the first 2 treatment courses. The clinical and myeloma-associated variables evaluated are presented in Table 3. Multivariate analysis showed that only poor performance status (Eastern Cooperative Oncology Group [ECOG] performance status ≥ 2) had statistical significance as a risk factor for developing SBI during the total period of bortezomib-based treatment (hazard ratio [HR], 5.365; 95% confidence interval [CI], 2.004–14.364, P = 0.001, Table 3), within 3 months (HR, 4.976; 95% CI, 1.817–13.624, P = 0.002), and within 2 courses (HR, 8.652; 95% CI, 2.845–26.310, P < 0.001).
Table 3
Univariate and multivariate analysis for the risk of developing severe bacterial infection during bortezomib-based treatment in 98 patients (patient-based analysis)

HR, hazard ratio; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group; DS, Durie-Salmon; ISS, International Scoring System; VD, bortezomib-dexamethasone; VMP, bortezomib melphalan prednisolone; PAD, bortezomib doxorubicin dexamethasone; WBC, white blood cell; ANC, absolute neutrophil count; ALC, absolute lymphocyte count; Ig, immunoglobulin.
![]()
Risk factors for developing SBI during the 427 courses of bortezomib-based treatment
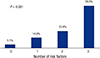
The risk factors that changed during each treatment course were evaluated. The incidence of SBI was higher in the treatment courses where poor performance status (ECOG ≥ 2, 34.2% vs. 10.6%, P < 0.001), pretreatment lymphocytopenia (ALC < 1.0 × 109/L, 25.1% vs. 14.6%, P = 0.005), and pretreatment hypoalbuminemia (serum albumin < 3.5 g/dL, 36.0% vs. 11.1%, P < 0.001) were reported, and early in the course of treatment (≤ 2 courses, 28.4% vs. 11.9%, P < 0.001) compared with other courses. There was no significant change of the median ALC at each cycle during bortezomib-based treatment (P = 0.983). According to the univariate analysis, poor performance status (P < 0.001), pretreatment lymphocytopenia (P = 0.007), pretreatment hypoalbuminemia (P < 0.001), and early course of treatment (P < 0.001) were significantly associated with the development of SBI in each treatment course (Table 4). In the multivariate logistic analysis, poor performance status (HR, 3.920; 95% CI, 2.305–6.666, P < 0.001), early course of treatment (HR, 2.782; 95% CI, 1.633–4.740, P < 0.001), and pretreatment lymphopenia (HR; 1.728; 95% CI, 1.016–2.937, P = 0.043) were risk factors for developing SBI in each treatment course. The probability of developing SBI was 5.1% in the absence of risk factors, 14.9% with 1 risk factor, 23.9% with 2 risk factors, and 59.5% with 3 risk factors (P < 0.001, Fig. 2).
Table 4
Univariate and multivariate analysis for the risk of developing severe bacterial infections during the 427 courses of the bortezomib-based treatment according to the clinical and laboratory characteristic at the beginning of each course (course-based analysis)
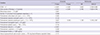
*These variables were excluded in the multivariate analysis because of collinearity with early courses of therapy. HR, hazard ratio; CI, confidence interval; ECOG, Eastern Cooperative Oncology Group.
![]()
Treatment outcomes
The overall response rate (at least partial response) of the SBI group was 51.9%, which was lower than that of the non-SBI group (70.5%, P = 0.048). Among the 98 enrolled patients, 48 patients (49.0%) died during the median follow-up period from the initiation of bortezomib treatment of 6.3 months (range, 0.5–57.1 months). The median OS was significantly higher in the non-SBI group compared with the SBI group (30.1 months vs. 6.1 months, P = 0.004) although PFS was not significantly different between the two groups (21.9 months vs. 18.1 months, P = 0.418).
In the 57 patients aged less than 65 year, 14 of the 24 (58.3%) patients in the non-SBI group received autologous stem cell transplantation, but only 6 of 33 (18.2%) patients in the SBI group received autologous stem cell transplantation (P = 0.002). Among the patients aged below 65 year, the SBI group showed a significantly shorter median OS compared with the non-SBI group (11.2 months vs. not reached, P = 0.016) and a significantly shorter PFS compared with the non-SBI group (6.0 months vs. 24.4 months, P = 0.015, Fig. 3).
 | Fig. 3Overall survival (A) and progression-free survival (B) after the bortezomib-based treatment of 57 MM patients under 65 years of age according to the presence of severe bacterial infection (SBI). MM, multiple myeloma; SBI group, patients who developed SBI; Non-SBI group, patients who did not experience SBI.
|
DISCUSSION
Herein we demonstrate that poor performance status (ECOG ≥ 2), early course of treatment (≤ 2 courses), and pretreatment lymphopenia (ALC < 1.0 × 109/L) are risk factors for developing SBI in MM patients treated with bortezomib-based regimens. More than half (59.5%) of the patients with all three risk factors developed SBI whereas only 5.1% of the patients without risk factors developed SBI. Therefore, we could expect the risk of developing SBI at the subsequent course of bortezomib-based treatment. It would be beneficial to manage MM patients susceptible to SBI. Although we found the poor performance status at diagnosis as significant risk factor for developing SBI during the total period of bortezomib-based treatment, the assessment of the risk factors in each course of bortezomib-based treatment would be more suitable to predict the exact risk of developing SBI in subsequent bortezomib-based treatments because the clinical and laboratory parameters changed in each treatment course.
The early course of treatment (≤ 2 courses) was defined as a risk factor for SBI in this analysis because of hypogammaglobulinemia associated with high tumor burden in the early period of treatment (21). A decreased level of uninvolved immunoglobulins in MM serves as a risk factor for infection with encapsulated bacteria (e.g., Streptococcus pneumoniae or Haemophilus influenzae) (7). The degree of immunoglobulin suppression and disease stage are interrelated (20), and decreased levels of uninvolved immunoglobulin have been known as an independent prognostic factor for shorter OS (21). Many studies conducted before the development of the novel agents demonstrated the increased risk of infections in the early period of treatment, particularly within 4-6 months following treatment, and the decreased risk of infections after achieving a favorable response to treatment (16,22,23). Because of the serial reduction of tumor burden in subsequent courses of the bortezomib-based treatment, the risk of SBI was significantly higher in the first two courses of bortezomib-based treatment in this study.
Poor performance status has been reported as a poor prognostic factor for survival (1,24), which increases treatment-related toxicity and/or the risk of infection in MM (25). Because the bortezomib-based treatment for patients with poor performance status is usually performed in the inpatient setting, these patients can be easily exposed to a variety of nosocomial infections. Cesana et al. reported a higher incidence of nosocomial infections in MM patients treated with VAD regimen in the inpatient setting compared with in the outpatient setting (6% vs. 0%) (16). Gram-positive encapsulated bacteria are known to be predominant pathogens in patients with MM. The incidence of infection with gram-negative bacilli increased after using alkylating agents or novel antimyeloma agents (7,26). In this study, gram-negative bacteria accounted for 70% of MDI cases and the most common pathogen was Acinetobacter baumannii (n = 7), a major pathogen of hospital-acquired pneumonia (27).
Lymphopenia at the beginning of each course was a novel risk factor for SBI in this study. It is generally considered to be associated with viral and fungal infections (28). However, several studies reported lymphopenia as a marker of severe sepsis and septic shock (19,29). Lymphopenia indicates a preexisting immunosuppressed condition. Therefore, patients with lymphopenia have inadequate immunologic reactions and consequently are vulnerable to bacterial infection. Until now, there is limited data about lymphopenia as a predictive factor for infection in MM. Jung et al. analyzed the data from 139 patients treated with bortezomib and observed that lymphopenia levels of < 0.8 × 109/L at diagnosis were a risk factor for SBI. Total 30 out of the 74 patients (40.5%) with lymphopenia developed SBI (30). In this study, the incidence of SBI in treatment courses with lymphopenia (< 1.0 × 109/L) was 42.0%, which was higher than the incidence of SBI in courses without lymphopenia (14.6%, P = 0.007). Considering the change of lymphocyte counts in each treatment course, the impact of lymphopenia at the beginning of each course in this study would be more valuable in clinical application.
Corticosteroid therapy has been reported to increase the incidence of infections with intracellular pathogens such as Listeria monocytogenes, various fungal species, and herpes viruses (31). The risk for infection is associated with the dose and the duration of therapy, and doses exceeding 20 mg of prednisone equivalent per day or a cumulative dose of more than 700 mg of prednisone can increase the risk of infections (22). Large cumulative doses of corticosteroids are frequently used during MM treatments and contribute to increase the risk of infection. A recent clinical trial compared lenalidomide plus low-dose dexamethasone (40 mg once a week, on days 1, 8, 15, and 22, every 28 days), lenalidomide plus high-dose dexamethasone (40 mg per day for four consecutive days on days 1–4, 9–12, and 17–20, every 28 days), and reported a higher incidence of infection in the high-dose dexamethasone arm (16%) compared with the low-dose dexamethasone arm (9%). The trial demonstrated a significantly decreased incidence of infectious complications and resultant improved OS in low-dose dexamethasone group (32). In this study, there was a trend to lower incidence of SBI in courses with lower doses of concomitant corticosteroid than higher doses of corticosteroid. The incidence of SBI was 18.0% in course with lower doses of corticosteroid (≤ 160 mg of dexamethasone equivalent dose) and 26.5% in course with higher doses of corticosteroid (> 160 mg of dexamethasone equivalent dose) (P = 0.151). However, we could not demonstrate a relationship between corticosteroid doses and the incidence of SBI because most of our patients received relatively low doses of corticosteroids during bortezomib-based treatment. Of the patients who received bortezomib combined with dexamethasone, the mean dose of dexamethasone was 157.45 ± 113.94 mg, which was very similar to the dose of low-dose dexamethasone, and only 6% of the patients received high-dose dexamethasone. Therefore, our cohort would be considered as a homogenous population that is suitable for assessing the risk factors for SBI.
The prophylactic use of antibiotics for reducing the bacterial infections has been proposed in MM. However, evidence about the prophylactic use of antibiotics in non-neutropenic MM patients is still inconclusive (33) whereas the prophylactic use of fluoroquinolone has been recommended by the National Comprehensive Cancer Network (34). The emergence of resistance to antibiotics as well as their efficacy and safety are concerns with regard to the prophylactic antibiotics (35). Therefore, the prophylactic use of antibiotics should not be recommended to all MM patients but only to those at increased risk of bacterial infection. In addition, adjustments in the corticosteroid dose in patients with high risk of SBI in each treatment course can be a good strategy to decrease the incidence of treatment-related infectious complications. Therefore, further prospective studies are needed to elucidate the effectiveness of the prophylactic use of antibiotics in MM patients and to assess the potential risks and benefits of using lower doses of corticosteroids.
One of the limitations of this study is its retrospective nature. The prophylactic antibiotics and the corticosteroid dose were inconsistently administered depending on the patient’s situation. Therefore, the assessment of the risk of SBI after removing these confounding factors was limited although these factors might affect the risk of SBI. Although the SBI rates were not statistically different between the different regimens adopted (60.0% for VMP, 46.7% for PAD, and 58.6% for VD regimen), the rate obtained in this study was somewhat higher than that of other studies (11,21,36). Because many of the patients in this study had a relatively poor performance status (36.8%) at the time of bortezomib initiation, the high incidence of SBI in this study may be attributed to this factor.
In conclusion, the three risk factors for developing SBI identified in the present study were the early course of therapy, poor performance status, and lymphopenia at the beginning of each treatment course in MM patients treated with bortezomib-based regimen. Therefore, patients with these risk factors should be more closely monitored for developing bacterial infections during subsequent bortezomib-based treatments. Risk-adapted approaches such as the prophylactic use of antibiotics or modification of the corticosteroid dose should be considered to reduce the incidence of bacterial infection in those patients. Further prospective studies are needed to support the implementation of effective preventive strategies against bacterial infection.
 XML Download
XML Download