

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Rheumatoid arthritis (RA) is a chronic disease with the characteristic feature of persistent inflammatory synovitis (1). Neovascularization, increased capillary permeability, exudation of plasma proteins into the synovial stroma, and infiltration of cellular elements cause synovial inflammation leading to cartilage destruction, bone erosion and joint destruction (1,2). In the clinical environment, final diagnosis of RA is made on the basis of typical clinical symptoms and signs, detailed physical examination by a rheumatologist, supporting laboratory findings and radiographic imaging.
Recently, imaging modalities such as ultrasonography, MRI, bone scintigraphy and PET/CT in addition to plain radiography have been used to provide information about joint inflammation and damage in the clinical assessment of RA (3). Bone scintigraphy has several advantages over these other imaging modalities for evaluating multiple joint problems because of its high sensitivity, good availability, low cost, and the possibility of whole body imaging (4). However, conventional bone scintigraphic findings in RA are considered as non-specific due to increased uptake of the radiopharmaceutical in the affected joint area as a result of joint inflammation, or reactive bone repair process in the remission state, and is not proportional to disease activity (5,6). Three-phase bone scintigraphy consists of perfusion, blood pool and bone phase images, which are capable of showing active inflammation in specific joints (7), and regional blood flow and inflammation have often been assessed using this modality (8-10). In RA patients, three-phase bone scintigraphy seems able to provide information on periarticular bony structure as well as inflammatory synovitis through perfusion or blood pool activity which is consistent with the central pathologic features of RA. Yet, there are no objective data on the value of bone scintigraphy with additional perfusion or blood pool imaging for evaluating arthralgia and arthritis.
The purpose of this study was to investigate the value of bone scintigraphy with additional blood pool phase (BSBP), compared with conventional bone scintigraphy (CBS), in the assessment of RA.
MATERIALS AND METHODS
Study subjects
All consecutive patients who first visited our rheumatology department from January 2010 to December 2010 for arthralgia (pain, tenderness, or swelling) and underwent BSBP were retrospectively accessed. A total of 242 patients (43 males, 199 females; age range, 14–78 years; mean age ± SD, 48 ± 12 years) were finally included after excluding 12 patients due to inappropriate imaging. Any involved joints were assessed by a rheumatologist for the presence of arthritis at the initial physical examination, and the joints were classified as large or small. Gold standard diagnoses of RA were made by the experienced rheumatologist based on the 1987 American College of Rheumatology (ACR) classification criteria (11) together with detailed history taking and physical examination, laboratory tests, and radiographic findings for symptomatic joints.
Demographic features such as age and sex, as well as laboratory biochemical tests including C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), auto-antibodies including rheumatoid factor (RF), and anti-cyclic citrullinated peptide antibodies (anti-CCP antibody) were also evaluated. The normal upper limits of the above tests in our hospital were 0.3 mg/dL, 10 mm/hr for men and 20 mm/hr for women, 15 IU/mL, and 25 U/mL, respectively.
Image acquisition
Bone scintigraphy was performed in a dual-head gamma camera (ECAM, Siemens Medical System, Chicago, IL, USA) with IV injection of 740 MBq of technechium-99m hydroxymethylene diphosphonate (99mTc-HDP). Regional images were obtained about 5 minutes after injection for joints of interest indicated by reported pain or swelling (additional blood pool phase). Regional images of the same fields, as well as whole body images, were also obtained three to four hours after injection (bone phase). Finally, CBS consisted of whole body images and regional images on bone phase, whereas, BSBP consisted of whole body images, regional images on additional blood pool phase and bone phase.
Scintigraphic diagnosis of RA
Two board-certified nuclear medicine physicians with 15 years and 3 years of experience, respectively, who were not aware of the clinical data, results of laboratory tests, and other imaging studies, evaluated the bone scintigraphy in consensus. First, the number and locations of the joints with abnormal accumulations of 99mTc-HDP on CBS were assessed to interpret the abnormalities as “compatible with RA” or “not compatible with RA”. Increased periarticular bone uptakes in typical areas of RA joint involvement (proximal interphalangeal (PIP), metacarpophalangeal (MCP), wrist, elbow, knee, ankle, and metatarsophalangeal (MTP) joints described on the 1987 ACR classification criteria [11]) were considered as “compatible with RA” whereas periarticular bone uptakes in not typical area of RA joint involvement were considered as “not compatible with RA”. Second, the same parameters were re-evaluated on BSBP two weeks later to avoid recall bias. Patients with fusiform increased radiotracer uptake around joints on the additional blood pool phase with or without increased periarticular bone uptake on the bone phase in typical areas of RA joint involvement (PIP, MCP, wrist, elbow, knee, ankle, and MTP joints described on the 1987 ACR classification criteria [11]) were interpreted as “compatible with RA”. Whereas increased blood pool activity around joint and/or periarticular bone uptakes in not typical area of RA joint involvement were considered as “not compatible with RA”. (Fig. 1 and 2).
 | Fig. 1Findings are not compatible with rheumatoid arthritis (RA) on additional blood pool phase and bone phase of a patient with arthralgia. No significant increased blood pool activity (A) or periarticular bone uptake (B) in hands and wrists, elbows, feet, ankles and knees.
|
 | Fig. 2Findings are compatible with rheumatoid arthritis (RA) on additional blood pool phase and bone phase of patients with RA. Increased blood pool activity (A) and periarticular bone uptake (B) are shown in right 2nd, 3rd, 5th, left 3rd, 5th PIP joints and left 1st IP joint of both hands, in both wrists, in right elbow, in right 4th, left 2nd, 3rd, and 5th MTP joints of both feet, in right ankle, and in right knee.
|
Statistical analysis
Patient characteristics are presented as median and interquartile range. Mann-Whitney U test and Pearson’s χ2 tests were used to analyze statistical differences of demographic features and clinical features between the RA and non-RA group.
To compare the performances of BSBP and CBS in the diagnosis of RA, sensitivity, specificity, accuracy, positive predictive value (PPV), and negative predictive value (NPV) were calculated. The performances of BSBP and CBS in combination with RF or anti-CCP antibody were also evaluated. Differences between the two diagnostic modalities were evaluated using McNemar’s test. In addition, the diagnostic odds ratios of several laboratory biochemical tests, BSBP and CBS, as well as the combination of them, were calculated and compared.
Statistical analyses were performed with software (SPSS, version 10.1.4, SPSS Inc., Chicago, IL, USA) and P values below 0.05 were considered to indicate significant differences.
RESULTS
Clinical and demographic features of the patients
A schematic overview of data analysis and number and diagnosis of patients enrolled is shown in Fig. 3. Of the 242 patients, 95 (39%) were diagnosed as RA, and the remaining 147 (61%) as non-RA. The median (interquartile range) of total numbers of involved joints in the RA and non-RA patients were 5 (2-11) and 0 (0-1), respectively, for small joints (P < 0.001) and 1 (0-1) and 0 (0-1), respectively, for large joint (P < 0.001). The proportion of patients with elevated/positive CRP, ESR, RF, anti-CCP antibody were 42%, 67%, 69%, 76% for RA, and 12%, 23%, 19%, 12% for non-RA (all, P < 0.001). The median (interquartile range) duration of symptoms were 12 (6-36) months for RA and 10 (4-36) months for non-RA (P = 0.336) (Table 1).
 | Fig. 3Flowchart of the study design and number of patients enrolled. RA, rheumatoid arthritis; OA, osteoarthritis; PR, palindromic rheumatism; FMS, fibromyalgia syndrome; SpA, seronegative spondyloarthritis; AOSD, adult onset Still’s disease; Others, others not specified.
|
Table 1
Baseline characteristics of the rheumatoid arthritis and non-rheumatoid arthritis groups with arthralgia
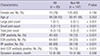
Values are given as median (interquartile range) for non-parametric data unless otherwise specified. P
values for the comparison between RA group and non-RA group were calculated using the Mann-Whitney U test and Pearson’s chi-square test. RA, rheumatoid arthritis; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; RF, auto-antibodies against rheumatoid factor; Anti-CCP antibody, anti-cyclic citrullinated peptide antibodies.
![]()
Of the 242 patients originally attending for arthralgia, 128 (53%) were found to have arthritis on the initial physical examination. Of these 128 patients with arthritis, 87 (68%) were diagnosed as RA, and of the remaining 114 patients without arthritis, only 8 (7%) were diagnosed as RA.
Scintigraphic diagnostic performance of BSBP and CBS for diagnosis of RA
For the original 242 patients with arthralgia, the sensitivity of BSBP for RA (n = 95) was significantly higher than that of CBS (84.2%, 80/95 for BSBP and 75.8%, 72/95 for CBS, P = 0.039). The specificity of BSBP was lower than that of CBS, but not statistically significant (83.0%, 122/147 for BSBP and 87.1%, 128/147 for CBS, P = 0.109). Their accuracies (83.5%, 202/242 for BSBP and 82.5%, 200/242 for CBS, P = 0.832) and PPVs (76.2%, 80/105 for BSBP and 79.1%, 72/91 for CBS) were similar. For the patients with arthritis upon first physical examination (n = 128, RA = 87), the sensitivity of BSBP was higher than that of CBS (87.4%, 76/87 for BSBP and 80.5%, 70/87 for CBS, P = 0.454) but the specificity was lower (63.4%, 26/41 for BSBP and 70.7%, 29/41 for CBS, P = 0.109), though neither effects were statistically significant. Their accuracies (79.7%, 102/128 for BSBP and 77.3%, 99/128 for CBS, P = 0.375) and PPVs (83.5%, 76/91 for BSBP and 85.4%, 70/82 for CBS) were again comparable.
When BSBP was interpreted with the results of elevated/positive anti-CCP antibody, its accuracy (86.0%, 208/242 for BSBP with anti-CCP antibody and 83.1%, 201/242 for CBS with anti-CCP antibody, P = 0.021) as well as sensitivity (68.4%, 65/95 for BSBP with anti-CCP antibody and 61.1%, 58/95 for CBS with anti-CCP antibody, P = 0.039) became significantly higher than that of CBS in the patients with arthralgia. The sensitivities of BSBP and CBS in combination with RF or anti-CCP antibody tend to be decreased, whereas, the specificities, accuracies, and PPVs to be increased compared with that of BSBP and CBS alone in the patients with arthralgia as well as arthritis (Table 2).
Table 2
Comparison of diagnostic efficacies of conventional bone scintigraphy and bone scintigraphy with blood pool for diagnosis of rheumatoid arthritis

Values are given as % (number). P values for the comparison of diagnostic efficacies between CBS and BSBP were calculated using the McNemar’s test. CBS, conventional bone scintigraphy; BSBP, bone scintigraphy with blood pool; RA, rheumatoid arthritis; RF, auto-antibodies against rheumatoid factor; CCP, anti-cyclic citrullinated peptide antibodies; PPV, positive predictive value; NPV, negative predictive value; NA, not available.
![]()
Odds ratio of BSBP and CBS for diagnosis of RA
For the patients with arthralgia (n = 242, RA = 95), the diagnostic odds ratio of BSBP positivity was higher than that of CBS positivity (26.0; 95% CI, 12.9–52.4 for BSBP and 21.1; 95% CI, 10.8–43.3 for CBS), indicating that BSBP positivity was a statistically significant factor for RA diagnosis and it was even higher than anti-CCP antibody positivity. For the patients with arthritis upon first physical examination (n = 128, RA = 87), the diagnostic odds ratio of BSBP positivity was slightly higher than that of CBS positivity (12.0; 95% CI, 4.9–29.4 for BSBP and 10.0; 95% CI, 4.2–23.4 for CBS), but both were much lower than that of anti-CCP antibody positivity. Moreover, when BSBP and CBS were interpreted with the results of elevated/positive RF or anti-CCP antibody, the diagnostic odds ratio of BSBP positivity and CBS positivity were more increased in the patients with arthralgia as well as with arthritis (Table 3).
Table 3
Value of conventional bone scintigraphy and bone scintigraphy with blood pool phase in predicting diagnosis of rheumatoid arthritis
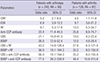
CBS, conventional bone scintigraphy; BSBP, bone scintigraphy with blood pool; RA, rheumatoid arthritis; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; RF, auto-antibodies against rheumatoid factor; Anti-CCP antibody, anti-cyclic citrullinated peptide antibodies; CI, confidence interval.
![]()
Causes of false interpretations of BSBP and CBS
Among the initial 242 patients in our patient population, excluding true positives and true negatives, CBS made 19 false positive interpretations due to increased periarticular bone uptake in 14 osteoarthritis (OA), 3 seronegative spondyloarthritis (SpA), 1 adult onset Still’s disease (AOSD) and 1 palindromic rheumatism (PR) patients, and 23 false negative interpretations. On the other hand, BSBP made 25 false positive interpretations due to increased periarticular blood pool activity and bone uptake in 18 OA, 4 SpA, 2 AOSD and 1 PR patients and 15 false negative interpretations.
DISCUSSION
The median duration of the symptom of RA and non-RA was 12 and 10 months respectively, which might suggest that the patients in our study represent for early arthritis (12). In these patients, both BSBP and CBS were diagnostic for RA, with comparable diagnostic performance. However, of the two, BSBP seems the more suitable for the early diagnosis of RA in arthralgia patients (Fig. 4), because it was more sensitive and gave fewer false negatives than CBS. In actual clinical practice, neither BSBP nor CBS by themselves are diagnostic tools for RA because rheumatologists make clinical diagnosis based on the combination of physical examination, laboratory results, and imaging findings for the gold standard diagnosis of RA. However, BSBP may be a better reference test for RA diagnosis than CBS. Its odds ratio, one of the most important parameters of diagnostic tests for estimating the probability of a positive diagnosis according to the gold standard diagnosis was higher than that of CBS in the patients with arthralgia, as well as in those with arthritis. Among several laboratory tests, anti-CCP antibody is known to have the highest sensitivity and specificity for RA as well as being a strong predictor of RA (13-15). The odds ratio of anti-CCP antibody positivity in the diagnosis of RA has been reported to range between 16.1 to 38.99 (13); and the odds ratio of anti-CCP antibody found in our study were comparable to these. In patients with arthralgia, the odds ratio of CBS positivity was similar to that of anti-CCP antibody positivity but that of BSBP positivity was even higher, suggesting that it has strong predictive value in these patients. These diagnostic odds ratio were more increased compared with anti-CCP antibody positivity when BSBP and CBS were interpreted with the results of clinical risk factors of elevated/positive RF or anti-CCP antibody.
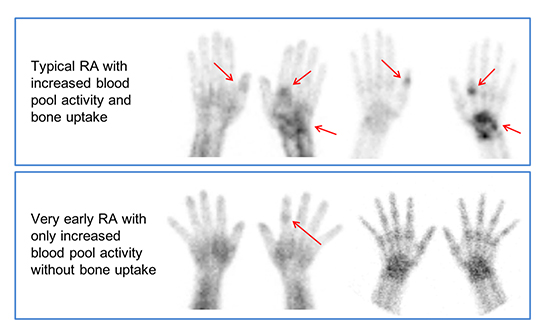
 | Fig. 4Hand radiography and 99mTc-HDP bone scintigraphy findings in rheumatoid arthritis (RA) patients with positive RF and anti-CCP antibodies. (A) A 51-year old female patient with right wrist and bilateral hands pain for 10 years. Hand radiography (left column) shows uniform joint space narrowing with periarticular bony erosion in the right wrist and 1st, 2nd, and 3rd MCP joints of left hand which are suggestive of advanced rheumatoid arthritis. CBS (middle column) and blood pool image of BSBP (right column) show increased periarticular bone uptakes as well as fusiform increased blood pool activity in corresponding area of structural changes on radiography, finally interpreted as “compatible RA” on both CBS and BSBP. (B) A 45-year old female patient with left wrist, both hands and left ankle pain for 3 years. Hand radiography shows (left column) negative finding. However, CBS (middle column) and blood pool image of BSBP (right column) show increased periarticular bone uptakes as well as fusiform increased blood pool activity in right 1st IP, left 2nd MCP joins of both hands and left wrist, finally interpreted as “compatible RA” on both CBS and BSBP. (C) A 47 years old female patient with both hands and both feet pain for 1 month which might represent very early RA patient. Hand radiography (left column) and CBS (middle column) show negative finding. However, blood pool image of BSBP (right column) shows fusiform increased blood pool activity in 2nd PIP joint of left hand, finally interpreted as “compatible RA” only on BSBP.
|
Unexpectedly, CBS had comparable sensitivity to BSBP, and the two modalities had comparable specificities and accuracies, in the patients with arthralgia, as well as in those with arthritis. The reason for this comparable high sensitivity and accuracy of CBS was that all the patients were retrospectively enrolled from our tertiary academic rheumatology department who visited for their joint symptoms. And, the scintigraphy results were carefully assessed by nuclear medicine physicians because of the high probability of periarticular bone uptake in such patients.
The BSBP had a relatively high false positive rate which implies that articular blood pool activity was elevated in the non-RA group such as OA, SpA and AOSD. It has been increasingly recognized that synovitis plays a more important role in the pathogenesis of OA than previously thought (16,17). Synovitis, infiltration of mononuclear cells into synovial membranes and production of several proinflammatory mediators, are not uncommon features of OA, although they are present at significantly lower levels than in RA patients (18). SpA is also a group of inflammatory rheumatic diseases with common clinical and etiological features such as axial and peripheral inflammatory arthritis, enthesitis, extra-articular manifestations (19), which might result in elevated blood pool activity around axial and peripheral joints. Comprehensive use of biochemical markers for acute phase reactants such as ESR, CRP, and ferritin as well as immunologic markers such as RF, anti-CCP antibody, and HLA B27 might lower the false positive interpretations of BSBP and CBS in these clinical circumstances. BSBP has a lower false negative rate than CBS and the use of this modality could help to exclude inflammatory arthritis especially in patients with equivocal joint symptoms and signs.
Several previous studies have underestimated the diagnostic efficacy of bone scintigraphy compared with other imaging modalities (5-7,20), because the majority of these studies involved late phase bone scintigraphy without perfusion or blood pool phase. In recent years, many studies demonstrated that angiogenesis is an essential event in maintaining inflammatory and immune responses, as well as supporting pannus growth and development of RA (21,22). New vessel formation and inflammation may increase the blood pool perfusion at perfusion or blood pool phase. Therefore, comparable or even higher diagnostic efficacy to the other imaging modalities would be expected if the perfusion phase were added. However, in real practice settings it is not possible to obtain additional whole body dynamic perfusion data in polyarthritis patients, and blood pool phase itself could provide clues about the blood stream in the region of affected joints. A previous study (23) found excellent agreement between blood pool scintigraphy and human polyclonal immunoglobulin (HIG) scintigraphy, which had been proposed as a specific imaging modality for assessing synovitis of RA (5,7,24).
Our study had several limitations. First, we retrospectively enrolled patients who visited our clinic (the rheumatology department of a tertiary hospital) and who underwent bone scintigraphy for evaluation of joint pain, tenderness or swelling which are common symptoms of RA. And the prevalence for RA seems to be higher in these subjects than in the general population; in other words, it could be an indication bias of our study result. However, our study is still meaningful in that it reflects clinical reality that is, rheumatologists do not consider bone scintigraphy if a patient has no joint symptoms or problems. Second, we retrospectively enrolled the patients in the year of 2010 when the new 2010 ACR/European League Against Rheumatism (EULAR) criteria for RA were not widely promoted. In other words, the new 2010 ACR/EULAR criteria could not apply for this study, because there was insufficient data to meet the conditions of the new criteria. Thirdly, our subjects were heterogeneous and not classified by symptom duration or presence of medication. Hence further evaluation in a more homogeneous population is needed to obtain more accurate and specified information about the diagnostic values of BSBP and CBS. Lastly, BSBP seems to be a promising imaging technique for sensitively detecting arthritis in multiple joints at a single session. But the value of this modality in the evaluation of early RA needs to be further explored in future studies by comparison with whole body MRI, which is recently been used to detect early RA (25,26).
In conclusion, both BSBP and CBS appear to provide acceptable accuracy and comparable diagnostic performance for diagnosing of RA among patients with arthralgia and/or arthritis. However, in the patients with arthralgia, BSBP was found to be more sensitive than CBS and more accurate when interpreted with the result of anti-CCP antibody. This could help physicians diagnose RA in daily clinical practice.
 XML Download
XML Download