

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
According to the definition of the International Headache Society (IHS), occipital neuralgia (ON), also known as C2 neuralgia, involves paroxysmal shooting or stabbing pain in the dermatomes of the greater occipital nerve (GON or nervus occipitalis major) and the lesser occipital nerve (LON or nervus occipitalis minor). From an origin in the suboccipital region, the pain spreads throughout the vertex, particularly the upper neck, back of the head, and behind the eyes. The pain may be accompanied by hypesthesia or dysesthesia in the affected areas. The most common trigger is compression of the GON or LON (1), with the GON more frequently involved (90%) than the LON (10%) (2).
EPIDEMIOLOGY
ON is a well-known disorder, but its incidence remains to be accurately determined. A study in the Dutch general population reported a relatively low incidence of 3.2 per 100,000. Female dominance was present but not significant, and no time and seasonal variation was found (3).
ETIOLOGY AND PATHOPHYSIOLOGY
Neuralgia is pain in one or more nerves caused by compression and/or irritation of peripheral nerve structures. In ON, irritation of the GON and/or LON by chronically contracted muscles and spondylosis of the upper cervical spine is often implicated (4,5). In addition, compression from intra- or extra cranial vessels, giant cell arteritis, callus formations after vertebral fractures, schwannomas, and other masses are rare causes of ON. The etiologies are summarized in Table 1.
Table 1
Known possible causes of irritation: vascular, neurogenic, muscular, and osteogenic

| Category | Causes of irritation |
|---|---|
| Vascular | · Irritation of the C1/C2 nerve roots by an aberrant branch of the posterior inferior cerebellar artery (69) |
| · Dural arteriovenous fistula at the cervical level (70) | |
| · Bleeding from a bulbocervical cavernomas (71) | |
| · Cervical intramedullar cavernous hemangioma (72) | |
| · Giant cell arteritis (73, 74, 75) | |
| · Fenestrated vertebra artery pressing on C1/C2 nerve roots (76) | |
| · Aberrant course of the vertebra artery (77) | |
| Neurogenic | · Schwannoma in the area of the craniocervical junction: schwannoma of occipital nerve (78, 79) |
| · C2 myelitis (80) | |
| · Multiple sclerosis (81) | |
| Osteogenic | · C1/C2 arthrosis, atlantodental sclerosis (82) |
| · Hypermobile C1 posterior arch (83) | |
| · Cervical osteochondroma (84) | |
| · Osteolytic lesion of the cranium (85) | |
| · Exuberant callus formation after C1/C2 fracture (86) |
CLINICAL PRESENTATION
Patients with ON suffer from a shooting or stabbing pain in the neck that radiates over the cranium. The pain is characterized as persistent, paroxysmally aggravating, and of variable distribution; can be perceived in the retro-orbital area due to the convergence of the C2 dorsal root and the nucleus trigeminus pars caudalis (6). Due to connections with the VIII, IX, and X cranial nerves and the cervical sympathicus, vision impairment/ocular pain (67%), tinnitus (33%), dizziness (50%), nausea (50%), and congested nose (17%) can also be present (7). On physical examination, tenderness along the course of the GON and LON can be observed. Sometimes hypoesthesia or dysesthesia can occur. The pain is located in the occipital area and may spread toward the vertex. Though usually unilateral, it may be bilateral.
DIAGNOSTIC METHODS
According to the International Classification of Headache Disorder (ICHD-II), ON belongs to the same family as cranial neuralgias, central and primary facial pain, and other headaches.
The diagnostic criteria are as below:
A. Paroxysmal stabbing pain, with or without persistent aching between paroxysms, in the distribution of the greater, lesser, and/or third occipital nerve
B. Tenderness over the affected nerve
C. Pain is eased temporarily by local anesthetic block of the nerve
Physical examination
Along the course of the GON (over the occipital protuberance) and/or the LON (about 3 cm superomedially to the tip of the mastoid process), tenderness is detected by palpation (8). Tingling may be evoked by light pressure or percussion on the nerve (Tinel’s sign). When patients lie on a pillow and hyperextend or rotate their neck, pain can occur (“pillow sign”).
Imaging studies
Magnetic resonance imaging is the most important tool in the diagnosis of this disorder as it enables visualization of the surrounding cervical and occipital soft tissues. A simple X-ray is useful to rule out underlying pathologies, such as arthritis and craniocervical instability. A CT scan of the craniocervical junction can reveal neoplastic or degenerative osseous pathology. Sometimes there may be a discrepancy between the radiological findings and the symptoms (9).
Diagnostic block
The clinical presentation (i.e., tenderness over the occipital nerves) and a temporary improvement in the headache with a local anesthetic diagnostic block of the occipital nerve on the affected side confirm the diagnosis (1). Occipital nerve block, as well as an essential diagnostic tool, can also be a good treatment option for ON. Thus, the anatomy of the occipital nerve and the location of the exact target site are very important. Clinicians should keep in mind that occipital nerve block relief is not specific for ON and that false-positive results occur with migraine and cluster headaches (7,10).
Anatomy of the occipital nerve
The GON is the largest pure sensory nerve in our body. The GON is the medial branch of the dorsal ramus of the C2 spinal nerve. The GON initially courses in a downward, lateral direction, makes the bend along the inferior oblique and is covered by the splenius capitis, the longissimus, and the semispinalis muscles. On rare occasions, the nerve travels intramuscularly within the inferior oblique muscle. The GON then turns upward and pierces the semispinalis capitis. Finally, it turns superolaterally to emerge into the scalp by piercing the aponeurotic fibrous attachment of the trapezius muscle and sternocleidomastoid muscle (SCM) to the superior nuchal line. At this exit site, the occipital artery and GON are closely associated. The GON splits and innervates the occipital skin (medial branches) and the region behind the pinna (lateral branches) immediately below the superior nuchal line (11-14). The emergence point of the GON is at the semispinalis muscle at a point 3 cm below the occipital protuberance and 1.5 cm lateral to the midline (13,15). Anatomical variations of GON are occasionally found, particularly in the vertical axis (16,17). The C2 ramus could be compressed between the posterior arch of the C1 and the lamina of the C2, but the nerve is not especially vulnerable at this location (11).
The LON originates from the dorsal ramus of the C2 and, occasionally, the C3. It ascends toward the occiput along the posterior border of the SCM. Near the cranium, it perforates the deep fascia and runs upward over the occiput, where it innervates the skin and communicates medially with the GON (18). Although there is some variability in the anatomy, the nerve mostly emerges from the posterior border of the SCM superior to the exit of the great auricular nerve. This point is approximately 6-7 cm lateral from the midline and 4-6 cm caudal to a line connecting the lowest points of the external auditory canals (15).
1) The Cruveilhier plexus: the connection among the C1, C2, and C3 sensory branches (Fig. 1)
Fig. 1
Anatomy around occipital nerve; Asan medical illustration team modified this figure with permission from Shane Tubbs (91).

Hollinshead stated that “The upper parts of the back muscles in the cervical region are also supplied by direct twigs from the dorsal rami of the second and third cervical nerves, and by branches that arise from the so-called posterior cervical plexus, a very simple series of loops between the first and second and the second and third dorsal rami, sometimes also with a loop to the fourth (19).” Articular branches of the C2–3 facet joint arising from communicating branches between the third occipital nerve and C2 dorsal ramus have also been found (20).
Neural interconnections, such as the Cruveilhier plexus, can affect the therapeutic results of cervical muscular and facet denervation procedures. Therefore, the anatomical variations in the craniocervical region, such as the Cruveilhier plexus, may result in resistant pain after partially destructive surgical procedures for ON (21).
2) The innervations of the C1, 2, and 3 nerves
Although the C1 nerve is not thought to innervate a cutaneous tissue, it supplies some sensory innervations to deep somatic tissues in the suboccipital region, including the short muscles of the occipital triangle, through its dorsal ramus, and the SCM, trapezius, and atlanto-occipital joint, through its ventral ramus. In addition, the sinuvertebral nerve of C1 innervates the median atlantoaxial joint, dura mater, and vertebral artery, in conjunction with the sinuvertebral nerves of the C2 and C3. The dorsal ramus of the C2 innervates the splenius capitis and semispinalis capitis and finally becomes the GON. The ventral ramus of the C2 supplies articular branches to the lateral C1/2 joint as well as the prevertebral muscles, SCM, and trapezius. The dorsal ramus of the C3 has three significant branches, the lateral, deep medial, and superficial medial branches. The lateral branch supplies the splenius capitis, cervicis, and longissimus capitis; the deep medial branch innervates the semispinalis cervicis and multifidus; and the superficial medial branch innervates the semispinalis capitis. The superficial medial branch is also known as the third occipital nerve, and innervates the C2–C3 zygapophyseal joint as well as the skin in the suboccipital region (22). Cervicogenic headache, which involves pain referral from cervical structures, appears to be produced by convergent excitation that is evoked by stimulation of these nerves and that results in excitation of second-order neurons in the trigeminocervical complex (Fig. 2) (23,24).

Injection point (Fig. 3)
Fig. 3
Landmarks for injection of the occipital nerves and electrical stimulation; Rogier Trompert Medical Art, modified with permission from Vanelderen et al. (9).

The injection points are variable. One of the points is located on a line that connects the middle of the ears, 3.18 cm from the midline. The other point is situated 3.8 cm lateral to the midline and one quarter of the distance along a line connecting the external occipital protuberance to the mastoid (or 2 cm lateral and 2 cm inferior to the external occipital protuberance). Some authors have described this point as being 1.5 cm lateral and 2 to 2.5 cm inferior to the external occipital protuberance (15-17,25-27). Great variability in the course of the GON is described in the literature (18,25,27).
Differential diagnoses
Several disorders share certain features with ON, such as pain in the posterior neck and head. It is therefore sometimes difficult to distinguish these disorders, unless additional features are seen. There are two important disease categories that clinicians should keep in mind. First, tumors, infections, and congenital anomalies (e.g., Arnold-Chiari malformation) should be distinguished. It is crucial to diagnose these disorders. If they are missed by clinicians, a devastating situation may result. ON can be mistaken for migraine, cluster headache, tension headache, or hemicrania continua (28). ON must be distinguished from referred pain from the atlantoaxial or upper zygapophyseal joints or from trigger points in neck muscle or their insertions (cervicogenic headache) (23,24,28). The critical differential point is that ON is neuralgia from the occipital nerve, whereas cervicogenic headache is nociceptive referred pain from cervical structures.
TREATMENT OPTIONS
Since ON was first described in 1821, numerous causes have been suggested and a variety of interventions have been used in its treatment (29). Currently, there is still no clear consensus on the management of ON. Medication, physical therapy, minimal intervention, and aggressive surgery are applied step-by-step. Evidence for the success of this approach is relatively weak. In addition, well-designed studies have rarely been reported. Treatment methods include medication, nerve blocks and, in refractory cases, neurosurgical procedures. Education, patient support, and reassurance are also important components of treatment. Management of neuropathic pain, which can develop following long-standing ON, should address both the pain itself and the psychological aspects associated with it.
Conservative management
Conservative treatment includes posture correction and reducing the neuralgic and muscle pain. Pharmacological treatment may include tricyclic antidepressants, serotonin reuptake inhibitors, anticonvulsants (e.g., carbamazepine, oxycarbamazepine, gabapentin, pregabalin), and opioids. Nonsteroidal anti-inflammatory drugs and paracetamol tend to have transient effects. The use of ergot derivatives is controversial. Infliximab has shown some benefit (9,30-32).
Interventional management
Botulinum toxin infiltrations
Several studies have shown an analgesic effect of Botulinum toxin A (BoNT-A) that outlasted the duration of its muscle relaxant effect (1,34). A few theories have been proposed to explain this analgesic effect of the toxin (35-38). For instance, BoNT-A’s inhibitory effects on sensory nerve mediators like substance-P (36), calcitonin gene-related peptide (37), and glutamate (38) may be involved in pain relief. Botulinum toxin may directly inhibit local neurogenic inflammation and indirectly inhibit central sensitization by significantly decreasing the activity of wide dynamic range neurons (38). Clinically, Botulinum toxin has been successfully used to treat several different types of headaches, including tension-type headaches (39), cervicogenic headaches (40), migraine (41), and chronic daily headaches (39). BoNT-A injection can relieve the sharp, shooting pain associated with ON, though not dull, aching pain, and improve quality of life for several months (42,43). The studies conducted with Botulinum toxin are listed in Table 2.
Table 2
Publications on the treatment of ON with Botulinum toxin injection, pulsed radiofrequency (PRF), and nerve neurolysis

| Study | Study design | Case No. | Follow-up duration | Outcome measure method | Results |
|---|---|---|---|---|---|
| The treatment of ON with botulinum toxin injection | |||||
| Taylor et al. (42) 2008 | Retrospective | 6 | 12 wk | VPAM | Sharp/shooting pain significantly improved; |
| Dull aching pain not significantly improved, | |||||
| Kapural et al. (43) 2007 | Case series | 6 | 4 wk | VAS | VAS 8.5 → 1 |
| PDI | PDI 56 → 17.5 | ||||
| Volcy et al. (87) 2006 | A case report | 1 | N/A | N/A | Improved temporarily |
| The treatment of ON with PRF | |||||
| Huang et al. (48) 2012 | Retrospective, multicenter | 102 | At least 3 mon | ≥ 50% pain relief for at least 3 mon | 51% positive result |
| Vanelderen et al. (49) 2010 | Prospective | 19 | 1, 2, and 6 mon | VAS | 52.6% significant improvement at 6 mon |
| Likert scale | |||||
| Choi et al. (47) 2012 | Retrospective | 10 | 6-10 mon | VAS, TPI | All patients improved |
| The treatment of ON with nerve neurolysis | |||||
| Ducic et al. (54) 2008 | Retrospective | 206 | Minimal, 12 mon | ≥ 50% pain relief | 80.5% positive result |
| Gille et al. (52) 2004 | Retrospective | 10 |
Mean, 37 mon (33-43) |
1) VAS | 1) 80/100 → 20/100 |
| 2) Consumption of analgesics | 2) decrease in all | ||||
| 3) Patient satisfaction | 3) satisfaction in all | ||||
| Magnússon et al. (5) 1996 | Retrospective | 18 |
Mean, 28.7 mon (12-38) |
NRS relief |
88.9% better than fair |
| > 75%: excellent | |||||
| 50%-74%: good | |||||
| 25%-49%: fair | |||||
| < 24%: poor | |||||
Pulsed radiofrequency treatment
Pulsed radiofrequency (PRF) treatment is known to reduce pain, primarily by the induction of a low-intensity electrical field around sensory nerves that results in depressed conduction and inhibition of long-term activation in the lightly myelinated A-delta fibers and the small unmyelinated C fibers (44). In animal studies, PRF-mediated pain relief is suggested to be due to modulation of the descending noradrenergic and serotonergic pathways (45).
To date, a few reports have been published concerning PRF treatment of ON (Table 2). All reports were observational cohort studies without controls. The treatment in these ON studies showed short-term to intermediate-term pain control and the parameters used were: 40–60 V voltage output; 2 Hz frequency; 20-ms pulses in a 1-second cycle, 120 seconds/cycle; 150–500 W impedance range; and 42°C plateau temperature. The authors advise that careful attention to selection criteria and treatment parameters may further improve treatment outcomes (46-49).
Surgery
Surgical treatment of ON can be considered when a patient does not respond adequately to medical therapies, such as repeated injections, or minimally invasive procedures, such as PRF treatment. Neurolysis of the occipital nerve (with or without sectioning of the inferior oblique muscle), C2 gangliotomy, C2 ganglionectomy, C2 to C3 rhizotomy, C2 to C3 root decompression, and neurectomy were historically introduced for medically refractory patients (5,50-57). However, the results were variable. Recently, there have been a few positive reports on peripheral nerve stimulation, a less invasive surgery, of the GON or LON. Of these approaches, both occipital neurolysis and occipital nerve stimulation (ONS) have been used commonly in the clinical field, recently. In selective cases, these methods have shown good outcomes, but a well-designed randomization study with a long-term observation is not yet available. Clinicians should bear in mind the risk that destructive procedures carry, which include the possibility of the development of painful neuroma or causalgia, conditions that may be even harder to control than the original complaint (58).
Neurolysis
Entrapment of the GON in its peripheral course is a significant pathology in ON. Five potential sources of entrapment of the GON are suggested: C2 nerve root (rare), inferior oblique muscle (rare), within the semispinalis capitis muscle, within the trapezius muscle/aponeurotic tendon, and angiolymphatics (occipital artery/vein crosses the GON; lymph node presence, within or distal to the trapezial tunnel) (54).
Neurolysis of the GON appears to provide safe, durable pain relief in selected patients with chronic headaches caused by ON (Table 2). Factors correlated with a positive outcome include tenderness over the GON, a positive response to GON block or Botox, a history of direct occipital trauma, and preoperatively being under the care of a neurologist or pain specialist (54). Sectioning of the inferior oblique muscle is reported to be effective when occipital pain is exacerbated or triggered by flexion of the cervical spine (52). However, cervicogenic headache is a contraindication of neurolysis (51). Careful preoperative diagnosis is needed.
Occipital nerve stimulation
Recently, successful results with ONS have been reported in the management of intractable headaches (Table 3), including cervicogenic headache, ON, transformed migraine, hemicrania continua, and cluster headaches. This stimulation technique involves the subcutaneous insertion of electrodes in the C1–C2 region of the posterior cervical spine (Fig. 3). Convergence of afferents from C1–C3 cervical nerves with trigeminal afferents is explained as the cause of the cervicogenic headache that results from activation of these nerves (59). The pain control mechanism of ONS is similar to that of gait control theory, considered in other peripheral nerve stimulation (58). As opposed to destructive surgery, ONS is fully reversible. If the patient does not want to use stimulation, it is easy to stop the stimulation and the device can be removed with a simple procedure.
Table 3
Summary of noteworthy articles on ONS for ON

| Study | Study design | No. | Follow-up duration | Outcome measure method | Results | Lead type used |
|---|---|---|---|---|---|---|
| Picaza et al. (88) 1977 | Retrospective | 6 | 12-46 mon | N/A | 3/6, good to excellent | N/A |
| Weiner et al. (64) 1999 | Retrospective | 13 | (1.5-6 yr) | > 50% pain relief | 92% positive result | Cylinder type |
| Oh et al. (66) 2004 (paddle) | Retrospective | 20 (10 ON, 10 migraine) | 1-6 mon | > 50% pain relief | 1 mon 100% (20/20) | Paddle type |
| 6 mon 94% (17/18) | ||||||
| Kapural et al. (67) 2005 | Retrospective | 6 | 3 mon | VAS | VAS 8 → 2 | Paddle type |
| PDI | PDI 48 → 14 | |||||
| Rodrigo-Royo et al. (89) 2005 | Retrospective | 4 | 4-16 mon | 50% pain reduction | Improved in all | Cylinder type |
| Slavin et al. (58) 2006 | Retrospective | 14 | Mean 22 mon (5-32 mon) | VAS 50% reduction | 70% positive | Cylinder type |
| Johnstone and Sundaraj et al. (65) 2006 | Retrospective | 7 | Mean 25 mon (6-47 mon) | VAS 50% reduction | 5/7 (71%) positive | Paddle type |
| Opioid doses | Reduction in all cases |
Other destructive surgeries
The approach to patients with ON must initially be conservative. Although C2 gangliotomy, C2 ganglionectomy, C2 to C3 rhizotomy, C2 to C3 root decompression, and distal neurectomy have been tried historically for intractable cases, these kinds of destructive surgeries risk the development of painful neuroma, causalgia, or intractable neuropathic pain, and thus their use is decreasing. The studies conducted with destructive surgeries are listed in Table 4.
Table 4
Summary of noteworthy articles on destructive surgery for ON

| Study | Study design | Surgical method | No. | Follow-up duration | Outcome measure method | Results |
|---|---|---|---|---|---|---|
| Sharma et al. (90) 2005 | Retrospective | Neurectomy | 22 | 6 wk | Pain relief | Relief in 90% |
| 18 mon | Relief in 70% | |||||
| Dubuisson (21) 1995 | Retrospective | Rhizotomy at C1-3 | 14 | 33 mon (3–66) | > 50% pain reduction | 71% positive result |
| Wang and Levi (56) 2002 | A case report | Ganglionect-omy of C2 | 1 | N/A | N/A | Pain relief (+) |
POTENTIAL COMPLICATIONS AND RED FLAGS
Complications of interventional management
Infection or bleeding may result from any percutaneous technique, though these are usually minor problems. A case of sudden unconsciousness due to inadvertent subarachnoid injection in a patient with a craniotomy defect has been reported (60). Temporary dizziness, injection site soreness, focal alopecia, and paresthesia due to nerve injury should be anticipated (61-63).
Complications of ONS
Poor outcomes after electrode implantation are a common problem that has been reported following up to 30% of implantations. Therefore, a test stimulation before permanent implantation is recommended in many studies. Permanent implantation is usually recommended when 50% pain reduction occurs on test stimulation.
CONCLUSION
Occipital neuralgia is defined by the IHS as paroxysmal shooting or stabbing pain in the dermatomes of the GON or LON (1). The GON is the medial branch of the dorsal ramus of the C2 spinal nerve. The GON initially courses in a downward, lateral direction, makes the bend along the inferior oblique and is covered by the splenius capitis, the longissimus, and the semispinalis muscles. The GON then turns upward and pierces the semispinalis capitis. Finally, it turns superolaterally to emerge into the scalp by piercing the aponeurotic fibrous attachment of the trapezius muscle and SCM to the superior nuchal line (11-13). On diagnosis, tumors, infections, vascular problems (e.g., posterior circulation hemorrhage or infarction), and congenital anomalies (e.g., Arnold-Chiari malformation) should be ruled out first. Various treatment methods exist, from medical treatment to open surgical procedures.
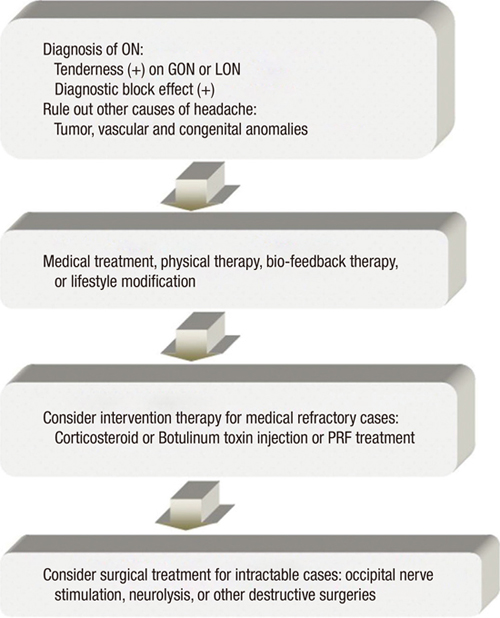
Clinicians should always remember that destructive procedures carry grave risks: once an anatomic structure is destroyed, it cannot be easily recovered, if at all, and with any destructive procedure there is always the risk of the development of painful neuroma or causalgia, conditions that may be even harder to control than the original complaint (58). The treatment of ON should be performed through adequate algorithm (Fig. 4).

 XML Download
XML Download