

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Venous thromboembolism (VTE), either deep vein thrombosis (DVT) or pulmonary embolism (PE) is one of the most common complications following total knee arthroplasty (TKA) (12). Although the clinical relevance and natural course of asymptomatic DVT remains unclear, symptomatic DVT is considered to have substantial risk for morbidity and fatal PE (1345). Thus, routine thromboprophylaxis for preventing VTE is recommended in all patients undergoing TKA, except in the case of high bleeding risk (145). On the other hand, unicompartmental knee arthroplasty (UKA) is less invasive and has a faster recovery time compared to TKA, and patients undergoing UKA are generally younger and more active compared with patients undergoing TKA. Indeed, the prevalence of symptomatic VTE following UKA in patients receiving routine pharmacological thromboprophylaxis is remarkably lower than that of TKA (6789). However, no gold standard strategy for preventing VTE in patients undergoing UKA has been established, and the optimal aggressiveness of thromboprophylaxis in UKA patients remains a challenging issue (8).
Recent studies have reported the prevalence of VTE following TKA was lower in the Korean compared to Western population (1011121314), and all VTE following TKA in Korean patients were completely resolved without pharmacological thrombolytic treatment (1516). Thus, taking into account for surgical invasiveness and patients demographics of UKA, the prevalence of VTE following UKA in the Korean population is estimated to be lower than that of Western populations with mild clinical course. However, equivocal results, regarding the prevalence of VTE following TKA between the Asian and Western population, have reported (1718). Moreover, most previous studies have tended focus on the prevalence of VTE following major orthopaedic surgery, such as total hip arthroplasty (THA) or TKA (1920). Therefore, the incidence of both asymptomatic and symptomatic VTE and the clinical features of VTE following UKA in the Korean population remain to be determined.
This study was conducted to determine the prevalence of VTE following UKA in Korean patients who do not receive thromboprophylxis; and the natural course of VTE following UKA in patients who do not receive therapeutic thrombolytic treatment.
MATERIALS AND METHODS
Subjected patients
The medical records of 71 consecutive patients who underwent 78 primary UKAs (unilateral or same-day bilateral) between March 2013 and March 2014 at single institution were reviewed using a prospectively collected database. After approved by institutional review board of our institution, only those patients who underwent UKA and had known clinical and radiographic outcomes with a minimum follow-up period of 1 year were included. Exclusion criteria included a history or current treatment of VTE or; newly diagnosed VTE at the preoperative evaluation. One patient was excluded because of a newly detected PE at the preoperative evaluation. Consequently, 77 knees of 70 patients, consisting of 60 female patients (67 knees) and 10 male patients (10 knees), were selected for final analyses. The mean age of the patients was 61 years (standard deviation [SD] 6.7, range 40–82). The mean body mass index (BMI) was 26.1 kg/m2 (SD 3.4, range 17.5–33.7).
All surgeries were performed by a single surgeon (I.Y.) under general anesthesia in a standard fashion. Oxford (Biomet, Warsaw, IN, USA) mobile bearing UKAs were used in 42 knees of 40 patients and Zimmer® Unicompartmental High-Flex Knee (Zimmer, Warsaw, IN, USA) fixed bearing UKAs were used in 35 knees of 30 patients using standardized cementation technique. A pneumatic tourniquet that inflated to 300 mmHg was applied. Patients were encouraged to start their ambulation from the operation day and gradually increasing range-of-motion exercises. None of the patients received either pharmacological or mechanical thromboprophylaxis for VTE prevention. The mean hospital stay was 8 days (SD, 1.6; range, 7-16 days).
VTE were diagnosed based upon the findings of multidetector-row computed tomography (MDCT) venography (Somatome definition AS+, Siemens, Munich, Germany) which was read by a single radiologist. The presence of VTE was defined as any types of VTE, either DVT or PE detected on MDCT, regardless of symptom. In all patients, MDCTs were undertaken preoperatively and at postoperative 7 days. All patients who had newly diagnosed postoperative VTE were consulted to specialized internists in thrombolytic therapy whether to perform therapeutic thrombolytic treatment. The specialized internists agreed that all patients were followed up without thrombolytic treatment, because all of the VTEs were asymptomatic without radiographically pleuroparenchymal complications. A clinical investigator (K.J.H.) explained the findings of MDCT and the management plan to all patients who had newly detected VTE. Finally, follow up MDCT venography was performed at 6-months after surgery in all patients in whom VTE was diagnosed postoperatively.
A research assistant (K.M.S.) collected all clinical information. The clinical data included demographic information (age, gender, height, weight, and BMI). The indications for UKA were classified as 1) primary degenerative arthritis, 2) osteonecrosis, or 3) other causes. Pre-existing medical comorbidities included 1) cardiovascular conditions (coronary artery disease, congestive heart failure, valvular insufficiency, and arrhythmia), 2) pulmonary conditions (chronic obstructive pulmonary disease and asthma), 3) metabolic-endocrine disorder, 4) neurologic conditions (stroke, Parkinson’s disease, and seizure disorder]), 5) history of malignancy or chemotherapy, 6) history of varicose vein with phlebitis and history of VTE (DVT or PE) or familial history of VTE. VTE-related symptoms were classified into 1) asymptomatic, 2) DVT-related symptoms (pain and edema of the limb, venous distension or enlargement, or the Homan’s sign [21]), 3) PE-related symptoms (chest pain or discomfort, dyspnea, tachycardia, or hemoptysis), or 4) both DVT- and PE-related symptoms. Type of UKA was classified as 1) unilateral UKA, or 2) same-day bilateral UKA. Tourniquet time was also recorded. VTE lesions were classified into 1) No VTE, 2) distal DVT alone, defined as a thrombosis in the calf veins, 3) proximal DVT alone, defined as a thrombus in the femoral and/or popliteal veins, 4) PE with distal DVT, 5) PE with proximal DVT, or 6) PE alone. Each of established VTE lesions was monitored and each finding from MDCT venography was recorded separately.
Statistical analysis
Statistical analyses were performed using SPSS® for Windows (Version18.0; SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to report the prevalence of each VTE lesion. Chi-square tests were used to determine the statistical significance between differences for each categorical variable, and the Wilcoxon signed-rank test was used to evaluate the significance of differences between continuous variables. To determine the rates of VTEs, the proportion of each VTE lesion was calculated separately. To determine the clinical features of VTE, the proportion of each VTE-related symptom was calculated separately. To determine the natural course of VTE, each VTE patient was categorized as 1) complete resolution; or 2) residual lesion; and the prevalence according to the time period was assessed. P values < 0.05 were considered significant.
RESULTS
Although VTE lesions were newly detected in 18 (26%) out of the 70 patients, all of VTEs, either DVT or PE was asymptomatic. The most common type of VTE was the isolated distal DVT (16%) followed by PE combined with distal DVT (7%) and isolated proximal DVT (3%) (Fig. 1). In addition, none of the patients complained of VTE-related symptoms; and MDCT venography demonstrated that all VTEs were small and involved limited portion of calf vein or proximal tibioperoneal vein with neither lower leg edema nor pleuroparenchymal complication. There were no differences in demographic and surgical risk factors for VTE occurrence between the VTE and no-VTE groups (Table 1).
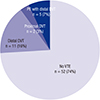 | Fig. 1Prevalence of VTE following UKA in patients who did not receive thromboprophylaxis. The most common VTE lesion was isolated distal DVT (16%) followed by PE with concomitant distal DVT (7%) and isolated proximal DVT (3%).
|
Table 1
Comparison of demographic and surgical factors between VTE and No-VTE groups*
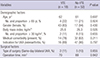
*Data are presented as numbers of patients (percentages). †Data are presented as mean values. VTE, venous thromboembolism; UKA, unicompartmental knee arthroplasty.
![]()
At the 6-month follow up MDCT, all types of VTEs were shown to be completely resolved, regardless of their location (Fig. 2 and 3). All of the VTE lesions maintained an asymptomatic status for 6 months after the surgery.
 | Fig. 2Serial MDCT venography images showing the natural course of postoperatively developed proximal DVT following unilateral UKA in a 71-year old female patient. Normal venous flows are observed at both proximal thighs preoperatively. Arrow indicates the left poplieal vein (A). Mild engorgement of the popliteal vein (arrow) is noted in the left proximal thigh at postoperative 1-week (B). At postoperative 6-month, the DVT lesion is completely regressed without thrombolytic treatment. Arrow indicates the left popliteal vein (C).
|
 | Fig. 3Serial MDCT scans showing the natural course of postoperatively developed PE following unilateral UKA in a 58-year old female patient. Preoperative finding. Arrow indicates the posterior basal segmental artery of right lower lobe (A). Newly developed PEs are noted on bifurcation of the right middle and lower lobe at postoperative 1-week. Arrow indicates the posterior basal segmental artery of right lower lobe (B). These lesions are completely regressed at postoperative 6-month without treatment. Arrow indicates the posterior basal segmental artery of right lower lobe (C).
|
DISCUSSION
This study found that although VTE in Korean patients undergoing UKA occurred frequently (26%), all VTEs were clinically asymptomatic and radiographically insignificant. In addition, they were completely resolved without any treatment.
In this study, the prevalence of VTE after UKA was 26%; however all of the VTEs were asymptomatic. The prevalence of VTE in this study seems to be higher than that of recent studies, which reported very low VTE prevalence following UKA, ranging from 0% to 5% (6782223) (Table 2). However, it is difficult to compare this study with previous studies because previous studies evaluated only symptomatic VTE patients who received routine pharmacological thromboprophylaxis. As there was no symptomatic patient in this study, if we had performed MDCT in symptomatic patients, the prevalence of VTE in this study would be comparable to those of previous studies. These findings concur with previous studies reporting lower prevalence of VTE, even after TKA in the Korean compared with Western population (1011121516) and indicate that appropriate strategies for preventing VTE following UKA reflecting prevalence and clinical features of this study should be established for the Korean population.
Table 2
Summary of previous studies reporting prevalence of VTE following UKA

| Author (year) | Country | No. of cases | Prophylaxis | Evaluation | Prevalence | Comments |
|---|---|---|---|---|---|---|
| Current study (2015) | Korea | 70 | No | All patients | Overall 26% | All PE developed with distal DVT. |
| DVT 26%/PE 7% | All VTEs were asymptomatic and resolved spontaneously. | |||||
| Lombardi et al. (2007) [7] | US | 423 | Chemoprophylaxis | Symptomatic patient | Overall 0% | - |
| Chan et al. (2009) [22] | UK | 239 |
Mechanical (No routine Chemoprophylaxis) |
Symptomatic patient | Overall 5% | 1 patient died due to PE. |
| DVT 3%/PE 3% | VTE occurred 6% of SD BUKA and 4% of St BUKA. | |||||
| Berend et al. (2010) [6] | US | 828 | Chemoprophylaxis | Symptomatic patient | Overall 0.1% | - |
| DVT 0.1%/PE 0% | ||||||
| Willis-Owen et al.(2011) [8] | UK | 1080 | Chemoprophylaxis | Symptomatic patient | Overall 0.3% | Overall VTE prevalence after TKA was 2.2% |
| DVT 0.3%/PE 0% | ||||||
| Chen et al. (2013) [23] | Singapore | 171 | Chemoprophylaxis | Symptomatic patient | Overall 4% | VTE occurred 2% of SD BUKA and 4% of StBUKA. |
| DVT 2%/PE 1% |
VTE, venous thromboembolism; DVT, deep vein thrombosis; PE, pulmonary embolism; SD BUKA, same-day bilateral UKA; St BUKA, staged bilateral UKA.
![]()
One interesting finding in this study was that all of the PEs occurred irrespective of proximal DVTs. In this study, MDCT venography revealed all of the PEs (7%) occurred concomitantly with distal DVT. However, all of the proximal DVTs (3%) were localized within the femoral vein without pulmonary involvement. These findings concur with previous studies reporting no significant association of proximal DVT and PE. These findings also asked question the mechanical propagation theory, which a proximal DVT was more likely to propagate and lead to PE (2425). These findings suggest that further studies are necessary to determine whether routine thromboprophylaxis for preventing DVT would reduce the incidence of PE in patients undergoing UKA.
This study found that all of the VTEs, either DVT or PE neither progress nor result in sequelae. In this study, all patients who had newly detected VTE followed up without receiving thrombolytic treatment. Follow up MDCT venography at postoperative 6-month showed that all VTE lesions resolved completely. These findings agree with previous studies, which reported complete resolution of VTEs without thrombolysis even in patients who underwent TKA, regardless of size or location (1516). The results of this study, together with those of previous studies, suggest that therapeutic thrombolytic treatment might be unnecessary in patients who had only radiological, clinically asymptomatic, VTEs following UKA.
This study has several limitations. First, all study participants were Korean and most were women (86%). Thus, the findings of this study may not be widely generalizable because the prevalence of VTE following UKA may be manifested differently among various ethnic populations and by gender. The female predominance among Korean patients undergoing knee arthroplasty has been well documented previously (2627). Second, we performed MDCT at postoperative 7 days in all patients and 6 months after surgery in patients who had newly diagnosed postoperative VTE. Therefore, asymptomatic VTEs which occurred 7 days after surgery might be missed. However, no gold standard period for monitoring of postoperative VTE has been established. Recent clinical practice guidelines recommend the minimum period of thromboprophylaxis as at least 7 to 10 days after major orthopaedic surgery (134). Third, as routine thromboprophylaxis rather than VTE screening test is recommended in all patients undergoing TKA (134), routine MDCT for VTE screening is not generally accepted in real clinical practice. However, asymptomatic VTE is common and symptoms of VTE are known to be nonspecific. Thus, routine preoperative and postoperative MDCTs were only way to investigate the accurate prevalence and natural history of VTEs following UKA. Fourth, although angiography is considered to be the traditional standard for detecting VTE, MDCT venography was used in this study. MDCT can evaluate DVT and PE simultaneously and previous studies validated its usefulness for detecting VTE in patients following knee arthroplasty (13282930). Fifth, the strategy for PE management used in this study may not be generally accepted because prompt initiation of anticoagulation therapy is recommended after diagnosis of acute PE to prevent thrombus extension and recurrent fatal PE. However, imaging tests for PE diagnosis are recommended after clinical probability assessment based on risk stratification and clinical signs and symptoms (31323334). Thus, no patient who had newly diagnosed postoperative VTE in this study would be indicated to perform MDCT because all VTEs were clinically asymptomatic with a low mortality risk. Moreover, asymptomatic VTE reported to be resolved spontaneously without any long-term sequelae, even after major orthopaedic surgery (153536). We discussed these issues with specialized internists in thrombolytic therapy before research commencement.Finally, the effect of the small sample size should be considered. This study is underpowered and subject to a type II error to detect the difference between the VTE and no-VTE group and to demonstrate the natural course of VTE. Other issues related to MDCT, such as cost and radiation hazard make it difficult to extend the patient enrolment time period. Further detailed prospective studies with sufficient sample size are needed to determine between group differences and the natural course of VTE and to identify the risk factors for VTE after UKA. Despite these limitations, this study is the first to report the prevalence and natural course of VTE following UKA in Korean patients who receive neither thromboprophylaxis nor therapeutic thrombolytic treatment.
In conclusion, this study demonstrates that VTE following UKA in Korean patients who do not receive thromboprophylaxis seems to occur frequently, but all of the VTEs are clinically asymptomatic. Moreover, all VTEs are spontaneously regressed within 6 months after UKA without long-term sequelae. The results of this study suggest that routine thromboprophylaxis or thrombolytic treatment in Korean patients undergoing UKA may not be necessary.
 XML Download
XML Download