

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Gout, one of the most common types of inflammatory arthritis, occurs when monosodium urate (MSU) crystals are deposited within or around the joints (1). Radiographic changes, such as periarticular soft tissue swelling and joint effusion, faint calcification, and bone erosion with/without tophi, can develop in the late stage of disease or after recurrent attacks (2). In gout, these radiographic abnormalities at periarticular and/or intraarticular structures have often been associated with functional disabilities and impaired quality of life due to the damage at joint structures such as cartilage and bones (3). In addition, clinical studies using diverse radiographic imaging modalities including plain radiography, conventional computed tomography (CT), and dual energy CT (DECT) have demonstrated that MSU crystals and tophi potentially contribute to bone erosion and structural damage at the joints affected by gout (45).
The evaluation of radiographic damage in inflammatory arthritis is extremely important, since structural damage of affected joints impairs the functional status of patients with various inflammatory rheumatic diseases and increases their economic problems and mortality (67). With regard to gouty arthritis, physicians have been highly interested in detecting radiographic damage through plain radiography, conventional CT, DECT, and magnetic resonance imaging (MRI) (24589). However, no relevant radiographic index has yet been proposed for assessing damage of affected joints in patients with chronic gouty arthritis. Recently, assessment of radiographic damage in chronic gout patients has been performed using application of the modified Sharp/van der Heijde (SvdH) method which is most widely used in RA (10) revealed that this scoring method could be reliable for assessment of radiographic damages in gout (11). In addition, new radiographic modalities such as conventional CT (12) or DECT (8) have been used with the rheumatoid arthritis MRI scoring system (RAMIS) (13) to evaluate bone erosion in gout.
However, no definite and simple radiographic imaging tools are available to detect radiographic joint damage such as bone erosion in gouty arthritis, despite the clinical investigations for development of radiographic tools that have been performed so far (81112). The SvdH scoring method has been proposed to be an alternative method for assessing joint damage in chronic gout (11). However, this scoring system is relatively complex and its relevance to clinical practice has not been proven. Thus, a simple method that can be applied in clinical practice is needed. The purpose of this study was to develop a new scoring method for radiographic damage (DAmagE index of GoUt; DAEGU) by modifying the SvdH method and to validate this new method.
MATERIALS AND METHODS
Patients
Fifteen male patients with chronic gout were recruited from an outpatient rheumatology clinic in Daegu, South Korea. All patients met the American College of Rheumatology criteria for acute gout (14). Patient demographic and clinical data including age, sex, disease duration, blood chemistry, and concomitant treatments were reviewed.
Radiographic damage scoring
Digital radiographic scans, including both anteroposterior and oblique views of the feet, were obtained according to the standard protocol of our department. Imaging for foot joint was obtained by plain x-radiography at the exposure of 54 kv and 200 mAs (Philips diagnostics, Hamburg, Germany). Preliminary training and standardization were performed for both the DAEGU and SvdH scoring methods. All radiographs were assessed by two radiologists (KTE and PKM) who were blinded to the clinical information including a pseudonymisation. Two experienced radiologists performed a second reading of the radiographs for the assessment of intraobserver and interobserver agreement.
For the DAEGU scoring method, the 10 metatarsophalangeal (MTP) and 2 interphalangeal (IP) joints of the first toes of both feet were analyzed, similar to the SvdH method. The erosion score for each joint site ranged from 0 to 4 (Fig. 1A). Erosions were given a score of 1 if localized lesions of cortical irregularity were present at the toe phalanx, without definite bony erosion. Erosions were given a score of 2 if any amount of definite bone erosion was present on the toe phalanx, without any evidence of intraarticular involvement. A score of 3 was given if the erosion was present on less than half of the circumference of the intraarticular surface of the joint involved. A score of 4 was given if the erosion extended over half or more of the circumference of the intraarticular surface of the joint involved. The maximum bone erosion score possible was 48 for each patient. Joint space narrowing was scored as follows: 0 = normal, 1 = generalized space narrowing without close contact between the two joint spaces, and 2 = bony ankylosis or complete subluxation (Fig. 1B). Thus, the cumulative joint space narrowing score ranged from 0 to 24 for each patient. Scoring examples from the affected joints of patients with gout are illustrated in Fig. 1C.

Statistical analysis
Clinical characteristics are described as median with interquartile range (IQR), unless specified otherwise. The normality of the data distribution was tested using both Kolmogorov-Smirnov and Shapiro-Wilk analyses, which showed a non-normal distribution. Intraobserver and interobserver reproducibility were analyzed using intraclass correlation coefficients (ICCs) and the 95% confidence interval (95% CI).
All validation tests were performed by comparing the median erosion scores, JSN scores, and sums of the erosion and JSN scores. To measure the extent of agreement of the two independent radiologists between the two different radiographic damage scoring methods (SvdH and DAEGU), intraobserver reliability and interobserver reliability were assessed by calculating the ICC and minimal detectable change (MDC) values. To calculate the ICC value, a two-way mixed average measure model (absolute agreement) was used. The ICC was considered excellent when the ICC value was greater than 0.8 (1516). The MDC was calculated using the standard error of measurement (SEM) in the formula given below (17). The MDC95 indicate that the difference in two measurements for about 95% of patients will be in this range. In case of excess for MDC95 values, it was regarded as the presence of real difference. In this formula, the Z-score represents the CI from a standard normal distribution (i.e. 1.96 for the 95% CI in this study), and the standard deviation (SD) was calculated from all the testing scores of the 2 assessments.


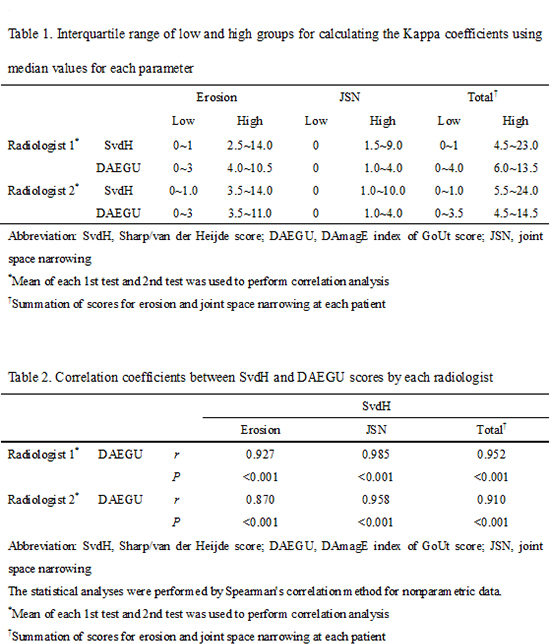
The correlation and agreement between the SvdH and DAEGU methods was assessed by calculating the Spearman's rho correlation coefficients for non-parametric data and Kappa coefficients. The median values for each parameter were classified into high and low groups, which were used to calculate the Kappa coefficients (Supplementary Table 1). When P values were less than 0.05, the results were considered statistically significant. All statistical analyses were performed using SPSS (version 18.0, SPSS Inc, Chicago, IL, USA).
Ethics statement
All patients provided written informed consent, and the protocol of this study was approved by the institutional review board (IRB) of Daegu Catholic University Medical Center (IRB No. CR-14-142-L). The authors assert that all procedures contributing to this work comply with the Helsinki Declaration of 1975 and its later amendments.
RESULTS
Baseline characteristics of enrolled subjects
A total of 15 male patients with chronic gouty arthritis were recruited for this study (Table 1). The median patient age was 50.0 (IQR 41.0–56.0) years. The median duration of gout was 40.0 (IQR 10.0–123.0) months. The median radiographic damage index scores for the two different methods were (total, bone erosion, and JSN, respectively): SvdH – 5.0 (IQR 0.0–7.5), 3.0 (IQR 0.0–5.3), and 1.3 (IQR 0.0–2.8); DAEGU – 4.3 (IQR 1.3–8.0), 3.8 (IQR 1.3–6.0), and 1.0 (IQR 0.0–2.0).
Table 1
General characteristics of enrolled subjects (n = 15)

*Summation of scores for erosion and joint space narrowing at each patient. IQR, interquartile range; SvdH, Sharp/van der Heijde score; DAEGU, DAmagE index of GoUt score; JSN, joint space narrowing.
![]()
Reproducibility of the DAEGU score
The intraobserver and interobserver reliabilities of the DAEGU scoring method were assessed by ICC analysis. The intraobserver ICC values ranged from 0.945 to 0.996 for the SvdH and DAEGU scoring methods (Table 2). The intraobserver DAEGU ICC values for reader 1 (Kim TE) and reader 2 (Park K) were 0.986 and 0.945 for the erosion score, 0.979 and 0.964 for the JSN score, and 0.987 and 0.968 for the total score, respectively. The interobserver DAEGU ICC values between reader 1 and reader 2 for erosion, JSN, and total score were 0.994, 0.993, and 0.996, respectively, which also indicates excellent agreement between the two readers (Table 3). These ICC values for intraobserver and interobserver reliability are comparable to those obtained using the SvdH scoring method.
Table 2
Intraclass correlation coefficient for intraobserver reliability

*Summation of scores for erosion and joint space narrowing at each patient. SvdH, Sharp/van der Heijde score; DAEGU, DAmagE index of GoUt score; IQR, interquartile range; ICC, intraclass correlation coefficient; CI, confidence interval, SEM, standard error of mean; MDC95, minimal detectable change at the 95% confidence interval; JSN, joint space narrowing.
![]()
Table 3
Intraclass correlation coefficient for interobserver reliability

*Summation of scores for erosion and joint space narrowing at each patient. SvdH, Sharp/van der Heijde score; DAEGU, DAmagE index of GoUt score; IQR, interquartile range; ICC, intraclass correlation coefficient; CI, confidence interval; SEM, standard error of mean; MDC95, minimal detectable change at the 95% confidence interval; JSN, joint space narrowing.
![]()
Other measurements of error and agreement, such as the SEM and the MDC, are given in Tables 2 and 3. The absolute SEM values in intraobserver tests for the DAEGU method ranged from 0.2 to 0.8, which indicates that minimal differences were obtained on repeated measurements compared with the original measurement (Table 2). Especially, the SEM values in interobserver test were less than 0.3, indicating excellent agreement with minimal differences (Table 3). These values were smaller than the SEM values obtained with the SvdH method, except for the erosion and total scores for reader 2 in the intraobserver test. Regarding the assessment of MDC95, the absolute MDC95 values ranged from 0.5 to 2.1 in intraobserver and from 0.3 to 0.7 in interobserver analysis performed by the DAEGU method (Tables 2 and 3). Generally, the MDC95 values for JSN were much smaller than those for erosion scores.
Correlation between DAEGU and SvdH scoring methods
We next assessed the degree of correlation between the DAEGU and SvdH methods for each radiological abnormality by comparing the erosion, JSN, and total scores as determined by each method. The DAEGU scores showed strong positive correlations with the SvdH scores for each reader (KTE: r = 0.927, P < 0.001; PKM: r = 0.870, P < 0.001 for erosion scores; KTE: r = 0.985, P < 0.001; PKM: r = 0.958, P < 0.001 for JSN scores; and KTE: r = 0.952, P < 0.001; PKM: r = 0.910, P < 0.001 for total scores) (Supplementary Table 2).
Fig. 2A and 2B showed close correlation of median scores of erosion and JSN measured by two radiologists between two different scoring methods (r = 0.871, P < 0.001 for erosion and r = 0.969, P < 0.001 for JSN). Strong positive correlations were also observed between the erosion scores and JSN scores in each of the different methods for assessing radiological damage (r = 0.954, P < 0.001 for the SvdH method and r = 0.860, P < 0.001 for the DAEGU method) (Fig. 2C and 2D).
 | Fig. 2Spearman's correlation analysis for median values of bone erosion and joint space narrowing calculated by two radiologists within and between SvdH and DAEGU scoring methods.
|
The Kappa coefficients for the total score between the DAEGU and SvdH methods were 0.869 (0.618–1.000) for radiologist 1 and 1.000 (1.000–1.000) for radiologist 2 (Table 4), illustrating very good agreement. Similarly, the Kappa coefficients for erosion score and JSN score between the two readers were 0.732 (0.387–1.000) for erosion and 1.000 (1.000–1.000) for JSN score.
Table 4
Kappa coefficients (95% confidence intervals) for DAEGU versus SvdH according to two categories of score
*Mean of each 1st test and 2nd test was used to perform Kappa analysis. SvdH, Sharp/van der Heijde score; DAEGU, DAmagE index of GoUt score; JSN, joint space narrowing.
![]()
DISCUSSION
Although nearly half of all patients experience radiographic changes over the course of disease, a reliable and simple radiographic outcome measure for structural joint damage in patients with chronic gout has not yet been established (2). The development of assessment tools for radiographic damage in gout is crucial for clinical investigative trials and for medical treatment at outpatient clinics. Moreover, the increasing prevalence and incidence of gout, in addition to the strong detrimental effects that gout can have on life quality and functional ability, also highlight the necessity of radiographic assessment modalities (31819). A number of diverse methods for scoring bone damage on the feet or hand joints of patients with gout have been introduced. These methods use radiographic imaging tools such as plain radiography (11), conventional CT (12), and DECT (8). The main purpose of the present study was to develop a more reliable and simple method for radiographic scoring for patients with gout. This method should enable physicians to easily score the degree of joint damage and explain this score to patients. We proposed a novel semi-quantitative radiographic damage index based on a simplified version of the SvdH method. Our method uses plain radiography to score the affected foot joints of patients with chronic gout.
Dalbeth et al. (11) was the first to demonstrate that a modified SvdH scoring method, which is frequently used for RA, can also reliably represent radiographic damage in chronic gout. The different radiographic characteristics of bone erosion and joint space narrowing manifested in chronic gout, including intraarticular as well as extra-articular bone erosion and well-defined erosions with sclerotic margins and overhanging edges in the advanced stage, necessitated substantial modification of the SvdH method, even though RA pathogenesis and gout pathogenesis have been proposed to be similar to erosive arthropathies (4). Chronic gout is also distinguished by the sequential radiographic changes that occur as the disease progresses. For example, periarticular soft tissue swelling and joint effusion mark the early phase, faint calcification occurs in the intermediate phase, and definite bone erosion with/without tophi distinguishes the late phase (2). As gout progresses, bone erosion is caused by the pressure exerted by growing tophi and also by proinflammatory cytokines, chemokines, and matrix-degrading enzymes produced by inflammatory and immune cells within or around the tophi (202122). Our scoring system takes these factors into account and is unique because of the following features: First, our method scores radiographic changes according to the time sequence of disease progression. Second, two opposite surfaces within the same joint are considered a single-scoring target joint. This method contrasts with RA scoring, in which two opposite surfaces of the same joint are scored separately. Our method simply and intuitively measures joint damage, which we regard as an important strength of our scoring method. Third, joint space narrowing is not commonly seen in uncomplicated gout (19). Instead, joint space narrowing is either accompanied by osteoarthritis or appears in the late stage of gout along with severe bone erosion (2324). The presence of joint space narrowing in the affected joint of gout might at least partially indicate some degree of disease progression. Therefore, we awarded one point for the presence of joint space narrowing, regardless of its degree, and two points for ankylosis or complete subluxation.
We assessed reproducibility of the two scoring methods by calculating the ICC, SEM, and MDC95 values. Similar to the SvdH scoring method, excellent DAEGU ICC coefficients were obtained for each individual radiologist and also between the two radiologists for the erosion, JSN, and total scores. Spearman's correlation analysis also showed a high degree of correlation between median scores of either erosion or JSN the two methods including DAEGU and SvdH scorings, as illustrated in Supplemental Table 2 and Fig. 2. Although the correlation between the JSN score and erosion score was slightly higher for the SvdH method compared with the DAEGU method, the analysis still indicates that the DAEGU scoring method is reliable and valid for assessing joint damage in chronic gout.
To assess radiographic erosion in the affected joints of gout, two new imaging modalities have been introduced, conventional CT (12) and DECT (8). Scores from the CT method, which is based on the RAMRIS, have been shown to be closely associated with plain radiographic damage scores (r = 0.86, P < 0.001), the number of subcutaneous tophi affecting the feet (r = 0.82, P < 0.001), and disease duration (r = 0.42, P < 0.05) (12). This preliminary method, which used conventional CT scanning, opened the door for new alternatives for assessing bone erosion. Recently, Shi et al. measured tophus urate volumes, bone erosion volumes, and erosion scores based on the RAMRIS using DECT scans of the feet or hands (8). This method had many advantages over previous methods and was proposed to be the new standard measure of joint damage in patients with gout. We fully agree that conventional CT and DECT each have unique strengths for detecting tophi in subcutaneous or deep tissues and directly visualizing MSU crystals, not to mention their excellent reproducibility and validity (19). However, these modalities also have some disadvantages, including high costs, the need for specialized equipment, and the exposure of patients to ionizing radiation. Plain radiography is the most widely available technique for identifying bone damage in clinical practice for patients with gout, even though plain radiography has somewhat lower sensitivity and accuracy compared with MRI and CT modalities (19). A quantitative analysis comparing plain radiography with CT scanning revealed a strong correlation between the radiographic erosion score and the CT erosion diameter (P < 0.001 for the linear trend) (4). We propose that our new method, which uses plain radiography, is reliable and feasible for assessing radiographic changes, even though our method has somewhat low sensitivity and accuracy for the detection of bone erosion at the joint affected by gout. Furthermore, the DAEGU method can be easily scored by physicians, and can also play an important role in patient education. Therefore, the DAEGU method will potentially encourage physicians to obtain the radiographic damage index on a more regular basis. It will also potentially help physicians explain conditions to their patients with confidence, and possibly also increase the level of patient treatment compliance via simple scoring.
The present study does have some limitations. First, only a small number of cases were included. Further studies with a larger group of subjects should be performed. Second, our proposed method assesses bone erosion and JSN in affected joints, but it does not include other various radiographic manifestations of gouty arthritis, such as the presence of tophi or new bone formations (NBFs), including spurs, osteophytes, periosteal NBF, ankylosis, and sclerosis (25). In addition, plain radiography revealed a strong correlation between NBF and bone erosion/JSN (25). Third, the present study did not examine correlations with clinical features such as disease activity or chronicity state, treatment response, or impairment of physical function. Therefore, future follow-up studies using the DAEGU method are required to look for these correlations with clinical characteristics. Fourth, this study only analyzed the 10 MTPs and 2 IP joints of the first toes of both feet. It did not include the DIP foot joint or any hand joint. Foot radiography is the basic test for diagnosing and assessing follow-up progress of patients with gout (19). Gout occurs most commonly in the foot, particularly in the 1st MTP, and affects the mid-foot and the ankle more frequently than the upper limb or the finger (26). However, our previous study using DECT scanning in patients with gout demonstrated bony erosion with MSU crystal deposition in the PIP joints of the feet (27). In addition, bone erosion by MSU crystals at the 2nd to 5th PIP and DIP joints has also been proposed to contribute to the erosion score (11). Therefore, further tests that include the PIP and DIP joints of the feet should be performed using our DAEGU method.
In conclusion, our radiographic damage scoring method (the DAEGU method) is reliable, feasible, and simpler for scoring chronic gout in patients compared with the modified SvdH scoring method. The DAEGU method will facilitate the evaluation of structural damage in patients with gout in clinical practice. It will also help physicians better understand gout progression and its treatment, thus simplifying and improving patient explanations.
 XML Download
XML Download