

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Despite the recent advancements in prevention and treatment of stroke, stroke remains the leading cause of disability and the fifth leading cause of death in the US. Especially in those older than 65 years, stroke is a leading cause of death and disability. In the future, due to rapid aging, stroke will have a larger socio-economic influence (1). Therefore, to aid in prevention, the identification of markers of stroke risk is important. Although stroke has been believed to be a multifactorial disorder with minimal classical patterns of inheritance, accumulating evidence has shown the importance of genetic factors in stroke. Especially, it has been reported that a number of inflammatory mechanisms play a fundamental part in stroke (2); thus, various inflammatory genes showing an association with stroke have received attention as candidate genes (34567891011). Also, genetic factors could have an effect on stroke onset, infarct size, and prognosis (12,13). Although several candidate genes have been studied as risk factors for stroke, there are few useful markers for the prevention, diagnosis, and treatment of stroke (14,15).
Interleukin-6 (IL-6) is a potent pleiotropic cytokine that regulates survival and differentiation of neuronal cells. This cytokine plays a substantial role in the immune system. The counterpart, interleukin-6 receptor (IL-6R) complex consists of IL-6R and the interleukin 6 signal transducer (IL6ST/GP130/IL-6 beta), which is associated with many other cytokines. If IL-6 binds to IL-6R, this complex binds to GP130, leading to intracellular signaling cascades (16). IL-6 performs as the main stimulator of C-reactive protein (CRP) production, the levels of which are known to be associated with metabolic syndromes such as obesity and diabetes, as well as with vascular events (17). As an extension of the study of IL-6R, IL-6, and CRP in stroke, the role of IL-6R needs to be elucidated. To our knowledge, there is no study about the associations between IL-6R polymorphisms and ischemic stroke (IS).
Disability after stroke is assessed through formal observation. The National Institutes of Health Stroke Scale (NIHSS) is a neurologic impairment assessment tool that provides an objective quantified measurement in stroke patients (18,19). Higher scores on NIHSS indicate greater stroke severity. In a previous IL-6 polymorphism study, patients with severe disability (NIHSS ≥ 6) were associated with a specific genotype (20). Stroke rehabilitation outcomes are usually assessed using the Modified Barthel Index (MBI), which is a validated tool scoring independent daily living (21).
The aim of this study was to assess whether single nucleotide polymorphisms (SNPs) of the IL-6R gene were associated with the development, neurologic status, and clinical features of ischemic stroke in the Korean population.
MATERIALS AND METHODS
All participants with stroke were patients who visited the Departments of Rehabilitation Medicine at Kyung Hee Medical Center and Kyung Hee University Hospital at Gangdong. Healthy control subjects were recruited from a general health check-up. IS patients were diagnosed based on magnetic resonance (MR) imaging, computed tomography (CT), or angiography. Exclusion criteria were ischemic heart disease or other causes of cerebrovascular events such as traumatic brain injury, transient ischemic attack, and vascular malformation, etc. The NIHSS and MBI scored were measured in the IS patients.
Peripheral blood samples were collected from the subjects, and genomic DNA extraction was performed using a QIAamp® DNA mini kit (QIAGEN, Valencia, CA, USA). The genotypes of the two selected SNPs ware determined by direct sequencing (MACROGEN, Seoul, Korea). The following primers were used in the polymerase chain reaction (PCR) amplification: rs4845617 (forward 5’-CTGTTCTCCCCGCTCAGGTGCG-3’, reverse 5’-AGAGGCGGACAGGCTAATG-3’) and rs2228144 (forward 5’-GTAGCCTGGGCCACTTCATCA T-3’, reverse 5’-GACCTCTGAGGCACAACTCAC-3’).
PCR consisted of 40 cycles at 94°C for 30 sec, 58°C for 30 sec, 72°C for 30 sec, and 1 cycle at 72°C for 5 min. An ABI PRISM 3730XL analyzer (PE Applied Biosystems, Foster City, CA, USA) sequenced the PCR products, and SeqManII software (DNASTAR, Madison, WI, USA) was used to analyze the sequencing data (22).
To obtain odds ratios (ORs), 95% confidence intervals (CIs), and P values adjusted for age and sex as covariates, SNPAnalyzer Pro (ISTECH, Goyang, Korea), Helixtree (Golden Helix, Bozeman, MT, USA), and SNPStats (http://bioinfo.iconcologia.net/index.php?module=Snpstats) were used. The Chi-square test was used to determine Hardy-Weinberg equilibrium (HWE). A multiple logistic regression analysis was adjusted for age and sex. In terms of increasing risk of disease, an increased specific allele frequency was noted in IS patients compared with the allele frequency of controls. To analyze the association between a polymorphism and disease, a contingency table and Chi-square test were applied using a prespecified genetic model. The codominant model was the most general model “where the disease risk associated with AB individuals lies between that of AA and BB individuals. In dominant model, with the hypothesis that carrying allele B increased risk of disease (dominant model), the AB and BB genotypes are pooled giving a 2 * 2 table. Alternatively, under a recessive model for allele B, cells AA and AB would be pooled. Additive model is assumed that increased disease risk of γ for AB genotypes and 2 γ for BB genotypes” (23). In this study, codominant model 1 compared major allele homozygotes with heterozygotes, and codominant model 2 compared major allele homozygotes with minor allele homozygotes.
To determine the haplotypes between the two SNPs and the clinical features in patients with IS, Haploview version 4.2 (Daly Lab, Cambridge, MA, USA) was used.
The statistical significance level was set at P < 0.05.
Ethics statement
The study was approved by the institutional review board of Medical Research Institute, School of Medicine, Kyung Hee University and Center, and Kyung Hee University Hospital at Gangdong (IRB No. KMC-IRB-761-09, KHNMC-IRB-2007-020). Informed consent was obtained from all patients before inclusion in the study.
RESULTS
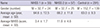
There were 121 IS patients (mean ± SD, 65.7 ± 12.1 years) and 291 controls (mean ± SD, 63.0 ± 9.3 years). The total IS group consisted of 68 males and 53 females. The control group consisted of 152 males and 140 females. There was a difference in mean age between IS patients and control subjects, but it was not significant (P = 0.30). Therefore, we adjusted the statistical results for age and gender. IS patients were classified into two subgroups according to NIHSS score (NIHSS 1, NIHSS score < 6; and NIHSS 2, NIHSS score ≥ 6) and MBI score (MBI 1, MBI ≤ 60; and MBI 2, MBI score > 60). The numbers of IS patients with NIHSS score < 6 and ≥ 6 were 56 and 57, respectively. The characteristics of the IS and control groups are shown in Table 1. The numbers of IS patients with MBI score ≤ 60 and > 60 were 71 and 25, respectively (data not shown).
Table 1
Demographic characteristics of ischemic stroke patients (NIHSS 1,2) and control subjects
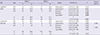
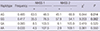
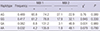
The genotype and allele frequencies of the two examined SNPs are shown in Tables 2 and 3, respectively. Two SNPs (rs4845617, 5TUR; rs2228144, Ala31Ala) of the IL-6R gene were in HWE in the IS and control groups, respectively (P > 0.05, data not shown). The genotype and allele frequencies of the two SNPs demonstrated no significant difference in IS cases and controls (Table 2). As shown in Table 3, the SNP rs4845617 was associated with the NIHSS score of IS patients (P = 0.011, OR = 0.24, 95% CI = 0.08-0.72 in codominant model 2, P = 0.006, OR = 0.30, 95% CI = 0.12-0.74 in recessive model, and P = 0.008, OR = 0.48, 95% CI = 0.28-0.84 in log-additive model). In SNP rs4845617, the frequencies of genotype according to NIHSS score was significantly different in the codominant model 2, recessive model, and log-additive model, and the A allele frequency was significantly higher in the NIHSS 1 group of IS patients. However, in SNP rs2228144, the genotype and allele frequencies did not correlate with the NIHSS score of the IS group (Table 3). Furthermore, rs4845617 and rs2228144 had no correlation with MBI score in the IS group (data not shown).
Table 2
Genotype and allele frequencies of the two SNPs (rs4845617, rs2228144) in ischemic stroke patients and control subjects
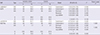
Table 3
Genotype and allele frequencies of the two SNPs (rs4845617, rs2228144) in ischemic stroke patients (NIHSS 1, 2) according to NIHSS score
We investigated the associations between haplotypes of control subjects and IS patients and NIHSS score. The haplotype frequencies of the two SNPs were not significantly different between control subjects and IS patients (Table 4). However, as shown in Tables 5 and 6, the AG and GG haplotypes differed between the NIHSS 1 and NIHSS 2 groups in IS patients. The frequency of the AG haplotype was higher in the NIHSS 1 group, and that of the GG haplotype was higher in the NIHSS 2 group of IS patients (P = 0.014, P = 0.0024, respectively). However, the haplotype frequencies found no significant difference by MBI scores (Table 6).
Table 4
IL-6R Haplotype frequencies in ischemic stroke patients and control subjects
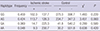
Table 5
Haplotype frequencies in ischemic stroke patients according to NIHSS scores
DISCUSSION
Ischemic stroke is known to be a heterogeneous multifactorial disease (24). Although conventional risk factors such as hypertension, diabetes, dyslipidemia and smoking account for a significant proportion of these stroke events, a considerable portion remains insufficiently explained by these factors (25,26). As risk factors for stroke, several genetic factors have been studied; however, there are few useful markers for prevention, diagnosis, and treatment of stroke (26). Therefore, increasing our understanding of risk factors including genetic components would allow us to predict the risk better, identification of novel stroke mechanisms, and new therapeutic approaches using genetic factors (27).
Several studies have reported the relationship between SNPs and stroke risk in Korea. Some of these SNPs include apolipoprotein E (3), 5-methyltetrahydrofolate-homocysteine methyltransferase (6), interleukin 4 (11), interleukin-1 receptor antagonist, tumor necrosis factor, interleukin 1 beta (8), neuropeptide Y (5), peroxisome proliferator-activated receptor gamma (9), phosphodiesterase 4D cAMP-specific chemokine (C-C motif) ligand 5 (4), thromboxaneA2 receptor, and thromboxane A synthase 1 (platelet) (10).
Several SNPs have been identified in the IL-6R gene, associated with carotid plaque (28), CRP (17,29) and obesity or diabetes (30313233). However, there has been no study of polymorphisms of the IL-6R gene in relation to stroke. Carotid plaque is assumed to be associated with increased stroke risk. In a genetic study in a Dominican population, IL-6R was suggested to be a related gene associated with carotid plaque (28).
Elevated CRP level predicts risk of stroke (17). IL-6 has been shown to have a positive correlation with CRP and to predict the risk of vascular events. The polymorphism of IL-6R gene is linked with CRP expression and plasma IL-6 level (34). Lu Qi et al. (35) demonstrated that the IL-6R variants (rs6684439, rs4845622, rs8192284, rs4329505) are significantly associated with plasma CRP level, independent of IL-6 level. In addition, the IL-6R variant interacts with CRP in relation to diabetes risk. In another study, the IL-6R gene (rs4845617) was suggested to play an important role in the pathogenesis of dyslipidemia and atherosclerosis (36). We identified SNPs of IL-6R, in coding regions near the promoter region, that had greater than 0.1 heterozygosity and greater than 0.1 minor allele frequency. For rs4845617, heterozygosity is 0.471, and minor allele frequency is 0.3804; for rs2228144, heterozygosity is 0.208, and minor allele frequency is 0.1178.
This is the first report to identify an association between SNPs of the IL-6R gene associated with risk of stroke and the clinical features of stroke. The two SNPs (rs4845617 and rs2228144) were not associated with development or daily activities of IS. However, our results revealed that SNP rs4845617 contributes to the neurologic status of IS patients. The mechanisms remain of the effects of IL-6R gene polymorphisms on stroke severity remain unclear. Compared with previous SNPs studies, the sample size in this study was relatively small. Therefore, other stroke risk factors analyses could be included while sample size became smaller after dividing groups with regard to hypertension, diabetes, dyslipidemia, and smoking history in this study. Further studies with larger sample size are necessary to elucidate this result.
In summary, two SNPs of the IL-6R gene (rs4845617, rs2228144) were analyzed in Korean ischemic stroke patients. The frequencies of genotype and alleles of the two SNPs demonstrated no significant difference in IS cases and controls. Therefore, the two SNPs are not associated with development of IS. However, in SNP rs4845617, the frequencies of genotypes according to NIHSS score are statistically different, and the A allele frequency in the mild stroke patients is significantly higher than an allele frequency in the severe stroke patients. This indicates that SNP rs4845617 is associated with the neurologic status evaluated by NIHSS in patients with IS. In addition, the A allele of SNP rs4845617 might have a protective effect against neurologic deficit in IS patients.
 XML Download
XML Download