

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Thyroid nodules are a common clinical problem, and differentiated thyroid cancer is becoming increasingly prevalent (1). Approximately 90% of thyroid cancer cases are well differentiated, and are usually classified as papillary thyroid carcinoma (PTC) or follicular thyroid carcinoma based on the predominant histology (2). Many variants of PTC have been described, including oncocytic, tall-cell, columnar-cell, diffuse-sclerosing, encapsulated, and follicular variants (3). Follicular variant PTC (FVPTC) is the second most common variant of PTC and variably accounts for 9% to 50% of all PTCs following conventional PTC, which is the most common type of thyroid cancer (456). FVPTC is composed predominantly of follicular architecture, which is lined by cells with nuclear features of PTC (7). Nevertheless, because it behaves clinically like PTC, it is classified as a subtype of PTC in the International Histological Classification of Tumors by the World Health Organization (8).
With the increasing incidence of thyroid cancer, FVPTC has been increasingly diagnosed in recent years. This increase in incidence may be due largely to increased detection of small nonpalpable nodules by thyroid US or other imaging modalities. Therefore, the incidence of papillary thyroid microcarcinoma (PTMC), defined as a PTC with a maximum diameter of 1 cm or less, has increased rapidly and a similar increase in micro-FVPTC is expected. However, the clinical behavior and outcomes of FVPTC remain controversial (4691011121314). In addition, cytologic diagnosis of FVPTC using fine-needle aspiration (FNA) can be difficult owing to the paucity of nuclear changes of PTC and overlapping features with other follicular-derived lesions (15).
Many clinical studies have reported relatively consistent sonographic findings of thyroid malignancy, especially for PTCs (161718); however, the sonographic features of FVPTC are not established. Some studies reported that FVPTC has a relatively benign appearance and is more similar to a follicular neoplasm than PTC on ultrasonography (US) (192021). To date, there are few studies of US features of FVPTC according to tumor size.
Therefore, in this study, we compared US features of FVPTC to those of conventional PTC according to tumor size.
MATERIALS AND METHODS
Subjects
All patients who underwent thyroidectomy and were finally diagnosed with PTC at our hospital between January 2007 and December 2012 were searched and a total of 249 cases (83 FVPTCs, 166 conventional PTCs) were included in statistical analysis for this study. A propensity score matching method was used for matching with age and sex as confounding variables, and logit was used to indicate the maximum width of the caliper for which matching should be done. The caliper size was 0.145 and the matching ratio was 1:2.
Thyroid ultrasonography
The sonographic findings of these thyroid nodules were retrospectively reviewed and clinical information was obtained from the medical records. The US images were analyzed retrospectively in a review by one endocrinologist (J.E.D.) with 10 years of experience in evaluating thyroid nodules. Ultrasound examinations were performed with a Philips HD 11 ultrasound system (Philips Healthcare, USA) equipped with a 5- to 12-MHz linear array transducer. The scanning protocol for all cases included both transverse and longitudinal real-time imaging of the thyroid nodules.
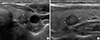
Each lesion was described using the sonographic features, including echogenicity, margin, shape, and presence of calcifications. The echogenicity of the tumor was compared with that of adjacent thyroid parenchyma. Malignant sonographic features were defined as marked hypoechogenicity (echogenicity lower than that of the surrounding strap muscle), irregular margins, a taller-than-wide shape (greater in the anteroposterior dimension than the transverse dimension in any plane), and microcalcification (tiny, punctate echogenic foci of 1 mm or less either with or without posterior shadowing). We classified the nodules as malignant even if only one of these suspicious sonographic features was present (16). Clinicopathologic variables such as tumor size, extrathyroidal invasion, and lymph node metastasis were evaluated. PTMC was defined as a tumor that measured ≤ 1 cm in diameter. Follicular neoplasm (FN)-like nodules were defined as having no accepted malignant feature (Fig. 1). PTC-like nodules were defined as having at least one accepted malignant feature (Fig. 2). The tumor-node-metastasis (TNM) stage of the tumor was determined using criteria from the 7th edition of the American Joint Committee on Cancer staging manual (22).

Statistical analysis
Comparison of mean values for the two groups was performed with t-test or Mann-Whitney U test, as appropriate. The categorical variables are presented as numbers and percentages, and were compared using the chi-square test or Fisher exact test. P < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA).
RESULTS
Comparisons of clinicopathologic findings of FVPTC and conventional PTC
Clinicopathologic characteristics of FVPTCs and conventional PTCs are summarized in Table 1. A total of 249 patients were included, 83 patients in the FVPTC group and 166 in the conventional PTC group. There was no significant difference in age and gender between the two groups. The size of the tumor was not significantly different between the two groups: 0.90 ± 1.11 cm in FVPTC patients and 0.74 ± 0.67 cm in PTC patients (P = 0.236). Micro- PTC was more common than macro-PTC in both groups (74.7% versus 80.7%, P = 0.274). The conventional PTC group had significantly higher central lymph node metastasis (36.7% versus 9.6%, P < 0.001) and extrathyroidal invasion (24.1% vs. 6.0%, P < 0.001) than the FVPTC group. The majority of FVPTCs (72.3%) were defined as suspicious for PTC by FNA.
Table 1
Comparisons of clinicopathologic findings of FVPTC and conventional PTC
Comparisons of sonographic findings of FVPTC and conventional PTC
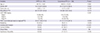
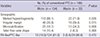
Sonographic features of an irregular margin (40.4% vs. 19.3%, P = 0.001) and marked hypoechogenicity (84.9% vs. 60.2%, P < 0.001) were more frequent in conventional PTCs than FVPTCs (Table 2). An irregular margin was less common in FVPTCs than conventional PTCs (19.3% vs. 40.4%, P = 0.001). Taller-than-wide shape (9.6% vs. 9.6%, P = 0.582) and microcalcification (13.3% vs. 22.9%, P = 0.071) were not significantly different between FVPTCs and conventional PTCs. A total 31 of 83 FVPTCs (37.3%) did not have sonographic malignant features, compared with only 13 of 166 conventional PTCs (7.8%, P = 0.001).
Ultrasonographic features according to the size of the tumor
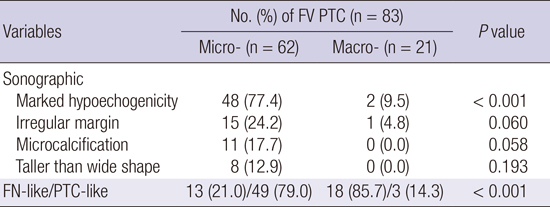
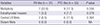
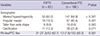
We evaluated the US features of FVPTCs according to the size of the tumor in a pathologic diagnosis. In the patients with macro-FVPTC (i.e., tumors larger than 1 cm) the sonographic feature of marked hypoechogenicity was significantly less common than for micro-FVPTC (9.5% vs. 77.4%, P < 0.001; Table 3-1). Sonographic features of irregular margin (24.2% vs. 4.8%, P = 0.060), microcalcification (17.7% vs. 0.0%, P = 0.058), and taller-than-wide (12.9% vs. 0.0%, P = 0.193) were not significantly different between the groups. Of the 62 micro-FVPTCs, 13 (21%) had FN-like features and 49 (79%) had PTC-like features. Of the 21 macro-FVPTCs, 18 (85.7%) had FN-like features and 3 (14.3%) had PTC-like features. However, in the comparison of US features of PTCs according to the size of the tumor, 124 of the 134 micro-PTCs (81%) and 29 of the 32 macro-PTCs (90.6%) had PTC-like features (Table 3-2). Unlike the results for FVPTCs, the conventional PTC group showed PTC-like features in US regardless of the size of the tumor.
Table 3-1
Sonographic findings of FVPTC according to tumor size
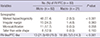
Table 3-2
Sonographic findings of conventional PTC according to tumor size
Comparisons of clinicopathologic characteristics of FN-like and PTC-like FVPTC
There were 31 patients in the FV-like group and 52 patients in the PTC-like group of FVPTCs (Table 4). Multifocality, extrathyroidal invasion, and lymph node metastasis were not significantly different between PTC-like FVPTCs and FN-like FVPTCs.
DISCUSSION
In the present study, FVPTCs showed a lower frequency of sonographically malignant features than conventional PTCs. Especially, FVPTCs larger than 1 cm had a more common benign sonographic appearance. As a very common variant of PTC, FVPTC has been increasingly diagnosed with the dramatic increasing incidence of PTC (1). This may be due to the increased use of neck US and early diagnosis (23). Despite the high incidence, the clinical behavior and outcomes of FVPTC remain controversial, making it challenging to establish a standard treatment strategy (4691011121314). Most published studies involved a small sample size and a short mean duration of follow-up. In a recent large population-based study, Yu et al. (14) reported that the clinical behavior of FVPTC larger than 1 cm is unique and represents an intermediate entity with clinical features that are between those of conventional PTC and follicular thyroid carcinoma (FTC). Interestingly, despite the variations in clinical behavior, the long-term outcome of these patients remains excellent and similar to that of conventional PTC. In addition, total thyroidectomy and radioiodine ablation significantly improved the disease-specific survival in patients with conventional PTC, but did not benefit the survival of FVPTC and FTC patients (14). Based on current evidence, the overall management and prognosis of FVPTC would be assumed to be similar to that of conventional PTC. However, it is still important to diagnose and differentiate FVPTC clinically and pathologically until any consensus is reached.
As mentioned earlier, FVPTC is known to have a relatively benign appearance on ultrasonography, more similar to that of follicular neoplasm than PTC (192021). However, there are few studies comparing the sonographic characteristics of FVPTC with those of conventional PTC. Yoon et al. (24) attempted to establish the sonographic findings of FVPTC and assess the role of preoperative FNA biopsy. The common sonographic findings of FVPTC were hypoechoic (51.9%), well-defined margins (51.9%), an oval shape (63%), and no microcalcifications (85.2%). Nevertheless, most lesions were correctly classified as malignant by both US and FNA biopsy. In our study, the sonographic findings of FVPTC patients were hypoechoic (60.2%), well-defined margins (80.7%), an oval shape (90.4%), and no microcalcifications (86.7%) (Table 2). Kim et al. (25) reported the sonographic features of FVPTC in comparison with conventional PTCs. The sonographic features of a taller-than-wide shape (5% vs. 22%), a spiculated margin (7% vs. 32%), marked hypoechogenicity (5% vs. 38%), and microcalcification (7% vs. 24%) were less common in FVPTCs than in conventional PTCs (all P < 0.05). In this study, marked hypoechogenicity was observed in the majority of FVPTCs and conventional PTCs (60.2% vs. 84.9%, P < 0.001).
Table 2
Comparisons of sonographic findings of FVPTC and conventional PTC
At the present time, the incidence of PTMC (defined as thyroid tumor ≤ 1 cm in diameter) has increased. Therefore, we performed a comparison of US features between micro- and macro-FVPTC. Among the patients with FVPTC, the sonographic feature of marked hypoechogenicity was significantly less frequent in macro- than micro-FVPTCs (9.5% vs. 77.4%, P < 0.001). In the patients with macro-FVPTC, the FVPTCs were relatively lower when malignant components are present (14.3% vs. 79.0%, P < 0.001). In contrast, the conventional PTC group showed PTC-like features in US regardless of the size of the tumor (81% in micro-PTC vs. 90.6% in macro-PTC, P = 0.475). Based on this result, it may be hard to find differences among FVPTCs on US in cases of microcarcinoma.
In the most recent study, Rhee et al. (26) reported that patients with FVPTC with malignant US features (taller-than-wide shape, infiltrative margin, marked hypoechogenicity, and micro- or macrocalcifications) have a worse prognosis (e.g., lymph node metastasis, higher stage) than patients with FVPTC without malignant US features. FVPTCs were divided into PTC-like and FN-like groups based on US findings. PTC-like nodules were defined as having at least one accepted malignant feature. These authors suggested that US might help to predict the behavior of FVPTC. However, in our data, multifocality, extrathyroidal invasion, and lymph node metastasis were not significantly different between PTC-like FVPTCs and FN-like FVPTCs.
Our study had some limitations. First, this retrospective analysis was limited by the small sample size. In addition, the prevalence of PTC variants in Korea was previously reported as 6.7% (2728). A large-scale prospective study would overcome these limitations. Second, although cytology specimens were evaluated by experienced pathologists, they did not use the defined criteria of the Bethesda System for Reporting Thyroid Cytopathology (29). This system can promote uniformity in the reporting of thyroid aspirates and is associated with defined risks of malignancy, allowing standardized management algorithms for each diagnosis. Third, FVPTCs were not divided into encapsulated and unencapsulated groups. It may differ from characteristics between two groups on US. Two distinct types of FVPTC are the common (or encapsulated) follicular variant with a less aggressive course and prognosis apparently similar to classical PTC, and the widely invasive (diffuse or multinodular) follicular variant (diffuse FVPTC) with a more aggressive course (30). Therefore, further distinction of US findings of the tumor may be helpful in order to define the clinical management strategy and prognosis.
In conclusion, FVPTCs showed fewer sonographically malignant features compared with conventional PTCs. In particular, FVPTCs larger than 1 cm had a more common benign sonographic appearance. Our data suggest that the possibility of FVPTC should be considered if the FNA result is suspicious for PTC in a nodule larger than 1 cm with no suspicious US features.
 XML Download
XML Download