

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dermatomyositis (DM) is an autoimmune connective tissue disease primarily involving the skeletal muscle and skin. Interstitial lung disease (ILD) is a common extra-muscular manifestation of DM and the main cause of death, with a reported prevalence of 20%-65% (123). Clinically, amyopathic dermatomyositis (CADM), a unique subset of DM, presents with cutaneous manifestations pathognomonic for DM, but with little or no muscle weakness (4,5). Compared with classic DM, patients with CADM are at higher risk of developing ILD. Moreover, ILD associated with CADM often progresses to respiratory failure, despite aggressive medical treatment (678). High serum ferritin levels, anti-melanoma differentiation-associated gene 5 (MDA5), interleukin (IL)-6, IL-8, IL-18, and Krebs von der Lungen (KL)-6 are predictive of rapid ILD progression and respiratory failure in DM patients; however, these factors cannot be measured in routine clinical practice (9,10).
Erythrocyte sedimentation rate (ESR) is a routinely used laboratory marker that reflects the extent of systemic inflammation. An elevated ESR is often observed in cases of infection, malignancy, and autoimmune disease (111213). The diagnostic value of routine inflammatory markers such as ESR has not been fully determined for DM, and is often neglected in routine clinical care. A recent study showed that an elevated ESR was associated with pulmonary impairment rather than with muscular inflammation in patients with inflammatory myopathies (14). However, the prognostic value of the ESR is unknown. Therefore, the aim of this study was to examine whether an elevated ESR is predictive of ILD and mortality in patients with DM.
MATERIALS AND METHODS
A total of 167 DM patients were treated at the Rheumatology Clinic at Seoul National University Hospital and Seoul National University Bundang Hospital from January 2004 through to June 2013. Classic DM and CADM were classified according to the Bohan et al. criteria and the Sontheimer definition, respectively (4,15). Patients with concurrent infection were excluded. Twenty-five DM patients with additional rheumatic diseases and seven whose ILD diagnosis was not definitive at the time of DM diagnosis were excluded. Furthermore, 21 patients with no available baseline ESR data at the time of DM diagnosis were excluded, resulting in a final study cohort of 114 patients (Fig. 1). ESR measured between DM diagnosis and the commencement of immunosuppressive therapy was considered as baseline ESR. ESR was automatically measured using only the modified Westergren method in a standardized manner. In addition, to rule out the influence of anemia, the main confounding factor on ESR elevation, ESR was individually revised as the hematocrit (Hct)-corrected ESR (ESR*[Hct/45]) (16). Demographic and clinical characteristics and laboratory values were ascertained from medical records.
 | Fig. 1 Diagnostic flow chart for patients with dermatomyositis (DM). DM, dermatomyositis; ESR, erythrocyte sedimentation rate; ILD, interstitial lung disease; CDM, classic dermatomyositis; CADM, clinically amyopathic dermatomyositis.
|
Diagnosis of ILD
A diagnosis of ILD was based on typical HRCT findings, which included irregular linear, reticular, or ground-glass opacities, consolidation, traction bronchiectasis, or honeycombing (17,18).
Pulmonary function test (PFT) results were obtained for 78 patients (46 [86.8%] with ILD and 32 [52.5%] without ILD). Forced vital capacity (FVC) and diffusing capacity of the lung for carbon monoxide (DLCO) were used to evaluate the degree of pulmonary impairment. FVC and DLCO were expressed as a percentage of predicted values, which were based on the patient’s age, sex, height, and weight.
Statistical analysis
Student’s t-tests, Mann-Whitney U test, and Fisher’s exact tests were performed for two-group comparisons as appropriate. Normal distribution of continuous variables was determined using Shapiro-Wilk statistics. Analysis of covariance (ANCOVA) was used to compare ESR values between groups after adjusting for clinical and laboratory parameters. Spearman’s correlation analysis was used to evaluate the relationships between ESR, pulmonary function, and muscle injury. Survival outcomes for each study group were calculated using the Kaplan–Meier method with the log-rank test and Cox regression analysis. A P value < 0.05 was considered statistically significant. Data analyses were performed using SPSS software version 18.0 (SPSS, Inc., Chicago, IL, USA).
Ethics statement
The study was approved by the institutional review board (IRB) at Seoul National University Hospital. The need for informed consent was waived by the IRB as the study involved no more than minimal risk due to its retrospective nature and because no identifiable information was used.
RESULTS
Clinical characteristics of DM patients with and without ILD
The demographic and clinical characteristics of DM patients with and without ILD are summarized in Table 1. For DM, the median age at diagnosis was 51.5 (interquartile range [IQR], 41.0-58.0) years and the median duration of follow-up was 20.4 (IQR, 8.3–60.3) months. ILD was diagnosed in 53 (46.5%) patients, and showed a similar prevalence in patients with classic DM or CADM (45.3% vs. 50.0%; P = 0.828). There was no difference between patients with ILD and those without in terms of fever, cutaneous manifestations (e.g., Gottron’s papules or heliotrope rash), and Raynaud’s phenomenon. By contrast, anemia, arthralgia, and mechanic’s hands were more common in patients with ILD. There was no difference in the levels of creatine kinase (CK) and lactate dehydrogenase (LDH) between the ILD and non-ILD groups. Anti-histidyl-tRNA synthetase (Jo-1) antibodies tended to be more common in patients with ILD (12.5% vs. 4.0%; P = 0.155). Strikingly, cancer was almost exclusively observed in DM patients without ILD (39.3% vs. 3.8%; P < 0.001).
Table 1
Baseline clinical characteristics and treatment histories of patients with and without interstitial lung disease (ILD)
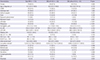
Data are expressed as the median (25th percentile-75th percentile), mean ± SD, or No. (%). P < 0.05 was considered statistically significant. Anti-Jo-1 antibodies were examined in 98 patients (48 patients with ILD and 50 patients without ILD). Baseline FVC and DLCO values were available for 78 and 72 patients with DM, respectively. *Student's t-test was used, instead of Mann-Whitney U test, because the data followed a normal distribution. †Steroid dosage prescribed initially is presented as the prednisolone equivalent dose (mg/day). ¶ Cumulative steroid dose is shown as the annual dose (mg/yr). DM, dermatomyositis; ILD, interstitial lung disease; CADM, clinically amyopathic DM; CK, creatine kinase; LDH, lactate dehydrogenase; FVC, forced vital capacity; DLCO, diffusing capacity of the lung for carbon monoxide; IVIG, intravenous immunoglobulin.
![]()
When comparing the treatment for DM, the median cumulative steroid dose (mg/year) was higher in DM patients with ILD than in those without (6,352.0 [IQR, 3774.0-8545.0] vs. 4665.0 [IQR, 2022.5-7430.0], respectively, P = 0.047). In addition, cyclosporine A, tacrolimus and cyclophosphamide were more frequently used in patients with ILD (Table 1).
ESR in DM patients with ILD
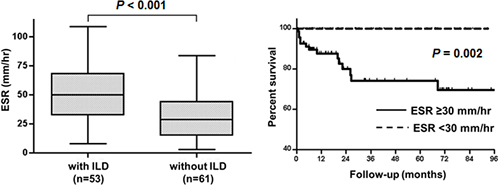
The ESR was markedly higher in patients with ILD than in those without (median 50.0 [IQR, 32.5-68.5] vs. 29.0 [IQR, 15.0-44.5] mm/hour; P < 0.001) (Fig. 2A). This association remained significant after adjusting for demographic and clinical variables (age, sex, fever, Hct, and malignancy) (P = 0.009). In case of Hct-corrected ESR, level difference according to ILD status was also remained (median 40.9 [IQR, 23.3-53.1] vs. 23.9 [IQR, 13.3-36.6] mm/hour, P = 0.006, after adjusting for age, sex, fever, and malignancy). Interestingly, ESR elevation was even more pronounced in the CADM subgroup of patients with ILD (ILD vs. non-ILD, median 56.5 [IQR, 38.8-74.8] vs. 20.0 [IQR, 14.5-28.0] mm/hour; P = 0.002). CADM patients with ILD showed the highest ESR, whereas CADM patients without ILD showed the lowest ESR (Fig. 2B). Of note, there was no significant difference in C-reactive protein (CRP) levels between the ILD and non-ILD groups (median 0.5 [IQR, 0.1-1.9] vs. 0.4 [IQR, 0.0-1.8] mg/dL; P = 0.434).
 | Fig. 2 Association between elevation of the baseline ESR and pulmonary impairment in patients with DM. (A) ESR levels at the time of DM diagnosis were higher in patients with ILD than in those without. (B) Differences in the baseline ESR were more pronounced in the CADM subgroup. The highest ESR level was observed in CADM-ILD patients, whereas there was no significant difference in the baseline ESR between CADM patients with ILD and classic DM patients with ILD (P = 0.235). (C) ESR was inversely correlated with FVC and DLCO. By contrast, there was no correlation between ESR and the extent of muscle injury, as measured by serum creatine kinase (CK) and aldolase levels. Box plots represent the median values (horizontal bars inside the box) and the 25th and 75th percentiles (bottom and top borders of each box, respectively). The whiskers represent the 5th and 95th percentiles, respectively. ρ = Spearman rank correlation coefficient. CDM, classic dermatomyositis; CADM, clinically amyopathic dermatomyositis; FVC, forced vital capacity; DLCO, diffusing capacity of the lung for carbon monoxide.
|
Baseline ESR was inversely correlated with FVC (Spearman ρ = - 0.303; P = 0.007) and DLCO (ρ = - 0.319; P = 0.006). Interestingly, ESR did not correlate with markers of muscle injury, i.e., CK (ρ = - 0.039; P = 0.683) and aldolase (ρ = 0.156; P = 0.128), at the time of diagnosis (Fig. 2C).
ESR elevation and mortality in DM
Nine patients with ILD and 23 patients without ILD were lost to follow-up. ILD led to higher death rate in DM patients (P = 0.017, log-rank test; power 0.504). A baseline ESR ≥ 30 mm/hour was associated with the presence of ILD (odds ratio 3.5; 95% confidence interval [CI], 1.5–8.1, P = 0.004). Overall, the mortality rate for DM patients with a baseline ESR ≥ 30 mm/hour was 19.7%, with a median survival time of 19.6 (IQR, 8.1-57.1) months. No deaths occurred in patients with a baseline ESR < 30 mm/hour (P = 0.002, log-rank test; power 0.839) (Fig. 3A). Also, an ESR ≥ 30 mm/hour at baseline tended to be associated with a 47.1-fold increase in the risk of death after adjustment for covariates including age, ILD status, accompanying malignancy, and the cumulative steroid dose (95% CI, 0.6–3933.8; P = 0.088).
 | Fig. 3Elevated ESR was predictive of mortality. (A) All-cause mortality for patients with a baseline ESR ≥ 30 mm/hour was higher than that for patients with a baseline ESR < 30 mm/hour. No deaths were observed in DM patients with a normal baseline ESR, even after 8 years of follow-up. (B, C) In both DM patients with ILD and DM patients without ILD, a baseline ESR < 30 mm/hour was associated with an excellent survival rate. (D) The ESR decreased with treatment in a time-dependent manner. (E) Patients with a persistently elevated ESR at 6 months (ESR ≥ 30 mm/hour) showed worse survival than patients whose ESR normalized after treatment.
|
In the ILD group, 10 (24.4%) of 41 patients with a baseline ESR ≥ 30 mm/hour and none (0%) of 12 patients with a baseline ESR < 30 mm/hour died during follow-up (P = 0.088, log-rank test; power 0.523) (Fig. 3B). Nine (90%) of the ten deaths were due to respiratory failure associated with ILD progression, and one was due to sudden cardiac death of unknown cause. In the non-ILD group, four (13.8%) of 29 patients with a baseline ESR ≥ 30 mm/hour died, whereas none of the 32 patients with a baseline ESR < 30 mm/hour died (P = 0.029, log-rank test; power 0.548) (Fig. 3C). All four died of complications associated with cancer progression or treatment (Table 2). In DM patients with cancer, an ESR ≥ 30 mm/hour was associated with higher mortality than an ESR < 30 mm/hour (P = 0.002; log-rank test; power 0.741).
Table 2
Causes of death in DM
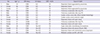
*Age at the time of DM diagnosis. †Baseline ESR level at the time of DM diagnosis. CDM, classic dermatomyositis; TPL, transplantation; MUO, metastasis of unknown origin; AKI, acute kidney injury; DLBL, diffuse large B cell lymphoma.
![]()
A normalized ESR after therapy and improved survival
All patients received high-dose glucocorticoids with or without additional immune-suppressants. Treatment led to reductions in the ESR in patient groups with and without ILD. The larger decline in ESR was observed in DM patients with ILD, with levels approaching those in the non-ILD group. The median ESR levels in patients with ILD vs. in those without ILD at 6, 12, and 24 months (± 1 month) were 28.0 (IQR, 13.5-51.0) vs. 20.0 (IQR, 11.0-34.0) mm/hour (P = 0.100) at 6 months, 22.5 (IQR, 15.3-40.0) vs. 19.0 (IQR, 10.0-32.0) mm/hour (P = 0.212) at 12 months, and 25.0 (IQR, 11.0-29.0) vs. 18.0 (IQR, 8.8-26.3) mm/hour (P = 0.284) at 24 months, respectively (Fig. 3D).
Patients with a persistently elevated ESR (i.e., ESR ≥ 30 mm/hour) after 6 months of treatment showed higher mortality than those whose ESR returned to normal (P = 0.039, log-rank test; power 0.582) (Fig. 3E). Persistently elevated ESR was significantly associated with the higher mortality after adjusting for the afore-mentioned covariates (hazard ratio 10.3; 95% CI, 1.1-100.2; P = 0.044).
DISCUSSION
We showed that the ESR is elevated in a distinct subset of DM patients, and that an elevated ESR correlates with both pulmonary impairment and overall mortality.
The ESR is influenced by several factors. For example, it increases with age and in the presence of anemia, chronic kidney disease, congestive heart failure, infection, and malignancy (111213). During inflammatory processes, monocytes and macrophages produce inflammatory cytokines such as IL-1, IL-6, tumor necrosis factor (TNF)-α, and interferon (IFN)-γ, which in turn induce hepatic production of acute phase proteins (19). The resulting change in plasma protein composition increases erythrocyte aggregation and accelerates the sedimentation rate. Therefore, an elevated ESR is expected in inflammatory conditions, and it should theoretically correlate with the total burden of inflammation in DM, in which global disease activity is associated with IL-6 and TNF-α levels (10). However, the present study confirms the previous finding that an elevated ESR in patients with DM is not associated with the extent of inflammatory muscle injury, but rather with the severity of pulmonary involvement (14,20). This suggests that inflammatory cells in muscle tissue secrete negligible amounts of cytokines into the blood stream, whereas cytokine production in the context of ILD is sufficient to induce an acute phase response. Indeed, higher serum TNF-α levels were uniquely associated with ILD (10) and a successful treatment of refractory DM-associated ILD with adalimumab, monoclonal antibody targeting TNF-α, supports the notion that the TNF-α, which is a key cytokine to increase ESR, might play a central role in ILD pathogenesis (21). The possibility that muscle inflammation makes a small contribution to the overall acute phase response is supported by the observation that classic DM patients (i.e., those without ILD) tend to have a slightly higher ESR than CADM patients without ILD (Fig. 2B). Alternatively, the lung parenchyma could be directly involved in producing acute phase reactants in patients with ILD. Further studies should address whether cytokine production is different among the specific organs involved in DM.
In contrast to ESR, CRP levels were only mildly elevated in DM and were not associated with ILD. In patients with systemic lupus erythematosus (SLE), type 1 IFN may directly inhibit the hepatic production of CRP, whereas the production of other acute phase reactants appears unaffected, leading to the ESR/CRP dissociation commonly observed during lupus flares (22,23). In DM, disease activity correlates with the expression of IFN-inducible genes and proteins (242526). Furthermore, IFN production in CADM patients is associated with ILD and an elevated ESR (27). Interestingly, Sato et al. (28) reported that the IFN-inducible proteins, CADM-140 or melanoma differentiation-associated protein 5 (MDA-5), are major auto-antigens in DM. As such, type 1 IFN may play a key role in the pathogenesis of ILD, and increased IFN production in patients with DM may contribute to both ILD and an elevated ESR.
Here, we found that the frequency of fever, Raynaud’s phenomenon, and muscle enzyme elevation was similar in DM patients with or without ILD. However, arthralgia, mechanic’s hands, and anemia were more common in patients with ILD. The difference in ESR between patients with and without ILD remained significant after adjusting for these variables, thereby identifying an elevated ESR as an independent risk factor for ILD.
In our study, the most common cause of death in DM patients was respiratory failure (Table 2). Since not all cases of ILD progress to respiratory failure, early identification of patients at risk of dying from ILD progression is of paramount importance (29). A previous study showed that low baseline FVC and DLCO levels were associated with a poor clinical outcome for DM-associated ILD (7). Here, we demonstrated that an elevated ESR at the time of DM diagnosis was correlated with low baseline FVC and DLCO levels (Fig. 2), and a persistently elevated ESR despite treatment was predictive of worse overall mortality (Fig. 3). A persistently high ESR might be explained by ongoing pulmonary inflammation. As such, measurement of the baseline ESR along with changes over time might be a highly cost-effective marker of disease activity and prognosis in patients with DM-associated ILD.
Since cancer is a major complication in patients with DM, active cancer screening is recommended at DM diagnosis (30). A prior study by Na et al. (31) showed that cancer was the leading cause of death among Korean patients with juvenile and adult DM, whereas the respiratory failure due to ILD progression was the most common cause of death in the current study. The difference might be explained by the relatively low prevalence of ILD of 12.5% in the prior study as compared to 46.5% in our study. Consistent with previous reports, we found that cancer was negatively associated with ILD (2,32); the cancer prevalence was much lower in the group with ILD (Table 1). This might suggest that cancer-associated DM spares the lung. Therefore, although cancer-associated DM is associated with the increase of ESR (12), a confounding effect of cancer on ESR elevation in DM patients with ILD would be only trivial.
This retrospective study has some limitations. First, laboratory and pulmonary function data were not available at regular intervals during follow-up. Therefore, there was a slight time discrepancy in ESR measurement among patients. Although ESR was measured in a standardized manner in our medical centers, it remains unclear as to whether all samples were processed in same way since information on the sample processing was not available. Second, we may have underestimated the prevalence of CADM because patients might primarily seek dermatology-related care, thereby contributing to selection bias. Third, patients without ILD were more likely to be lost to follow-up after recovery from their muscular symptoms. Fourth, we did not consider myositis-specific antibodies other than anti-Jo-1 because they are not included in the routine laboratory tests performed at our institution.
In conclusion, an elevated ESR in patients with DM is associated with pulmonary impairment and increased all-cause mortality. Elevated ESR in patients with DM should prompt the physician to carefully screen for the presence of ILD and to consider an early and aggressive treatment regimen.
 XML Download
XML Download