

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Several studies examining the relationship between maternal height and low birth weight showed that shorter maternal height was associated with reduced fetal growth and low birth weight (LBW) (1234) and concluded that the primary reason for this association was undernutrition/malnutrition. In developed countries, however, few studies are available on the effects of shorter maternal height on birth outcomes. Witter and Luke (5) reported that infants born from shorter women were symmetrically smaller than infants born from taller women in the United States. Evidence for the effects of shorter maternal height on birth outcomes remains sparse among women in developed countries.
To the best of our knowledge, no studies of Japanese people have demonstrated the effect of shorter maternal height on newborns’ health outcomes. Obstetric medical technology and maternity health care in Japan differ from those in other countries. First, Japan has one of the lowest infant mortality rates (2.3 per 1,000 births in 2011); medical technology including management in the neonatal intensive care unit (NICU), which is generally provided to both mothers and neonates, contributes to the low infant mortality rates. Second, Japan is rarely affected by food shortages; the food supply is currently stable at the national level. Despite the sufficient food supply, the obesity rate is low (only 7 to 14% of the adults in their 20s and 30s in Japan have a BMI over 25.0, Ministry of Health, Labour, and Welfare, Japan, 2010 [6]), and obesity is not a major health concern among Japanese pregnant or non-pregnant women. Third, health guidelines require frequent obstetrician/gynecologist visits during pregnancy; this also contributes to decreased health problems during pregnancy and at delivery and encourages child growth. In this situation, however, LBW has increased by nearly 10% over the past two decades in Japan (7). At the same time, NICU admission has been increasing and long-term admission is now a substantial problem in Japan.
In Japan, there is a greater focus on weight than on other anthropometry measurements, and most studies conducted on Japanese mothers investigated maternal weight, body mass index (BMI), and weight gain during pregnancy to evaluate their effect on birth outcomes (8910). However, the effects of shorter maternal height on birth outcomes are rarely investigated. The average height of Japanese women in their 20s and 30s is approximately 158 cm. This average value is similar to the average height of women in some low- to middle-income countries (11) but is shorter than that of women in developed countries. Therefore, we investigated the risk of shorter maternal height on LBW and subsequent NICU admission in Japan, where short stature is not an indicator of long-term exposure to undernutrition.
MATERIALS AND METHODS
Data sources
Newborns delivered at Seirei Hamamatsu General Hospital in Shizuoka Prefecture, Japan, from 1997 to 2010 were eligible for inclusion in this study (n = 21,855) (8121314). Seirei Hamamatsu General Hospital is located in the western part of Shizuoka Prefecture and provides advanced medical care for higher risk pregnant women with reproductive health problems. The participants’ information was collected under general clinical practice and recorded in individual medical records. The data included age, sex, smoking habits, alcohol drinking habits, maternal and paternal occupations, and the condition of the neonates after delivery.
Participants
We included singleton newborns who were delivered after the 37th gestational week, who had live births (the Apgar score was ≥ 1 one minute after birth), and whose sex was known (Fig. 1, n = 17,162). Participants for whom maternal height was unknown or determined as incorrect (< 50 cm, > 220 cm) were excluded (n = 12). We only included neonates born after the 37th gestational week to avoid confounding LBW with a mature birth and with a preterm birth (15). Ultimately, 17,150 participants were included in this study.

Exposure variables
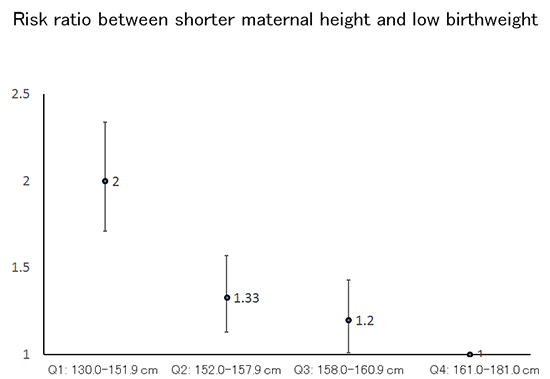
Maternal height was the primary exposure variable in this study. The distribution of maternal height among the participants ranged from 131.0 cm to 182.0 cm. We divided maternal height into four categories at quartile (Q) points: Q1, 131–151.9 cm; Q2, 152.0–157.9 cm; Q3, 158.0–160.9 cm; and Q4, 161.0–181.0 cm. The highest category (Q4) was used as a reference group in the statistical model. We also used this category as a continuous variable according to one quartile change (from Q1 to Q4 as 1 to 4) to check the dose-response relationship (P trend). Maternal height (cm) was used as a continuous value to assess the effect of a 1.0-cm change in height. Trend-test shows if there is an increased risk of LBW following 1cm change of maternal height, as well as 1quartile change (16). Height was measured by medical professionals at the Seirei Hamamatsu General Hospital.
Outcome variables
To evaluate newborn birth outcomes (the outcome variable in this study), we used information on LBW and admission to the NICU. NICU admission immediately following delivery or during hospitalization for the delivery was counted as yes, and other admissions were counted as no. Admission to the NICU after hospital discharge was not included because this information was not obtained. NICU admission may reflect newborns’ poor condition that was either related to or not related to LBW. All reasons for NICU admission were included. The possibility of healthy normal neonates' admission to NICU is minimum among those participants as healthy neonates without any abnormal signs usually stay at obstetric department in Japan. LBW was defined as less than (<) 2,500 g (15).
Covariates
We considered several potential confounders, including maternal age, maternal BMI at baseline (pre-pregnancy), maternal smoking habits, paternal smoking habits, maternal alcohol drinking habits, and maternal occupational status. This information was obtained from mothers by trained obstetricians or midwives at the time of the prenatal examination when the expected due date was confirmed (~ 10 weeks of gestational age) and added or corrected at admission or delivery. Maternal age (continuous value) was adjusted using two methods to avoid collinearity as follows: 1) the individual value of maternal age minus the group mean maternal age of the participants; and 2) the square of (the individual value of maternal age minus the group mean maternal age of the participants). Maternal BMI (kg/m2) was calculated as body weight (kg) divided by the square of height (m). Maternal smoking habits were divided into three categories (no, quit smoking after conception, smoking during pregnancy). Maternal alcohol drinking habits were assessed using dichotomous values (yes/no). Maternal occupation status was combined with paternal occupational status as a proxy of socioeconomic status and divided into seven categories: homemaker married to self-employed worker, homemaker married to company-employed worker (salaried worker), homemaker married to professional worker, all other homemakers, company-employed worker, professional worker, and all other types of workers.
Statistical analysis
A descriptive analysis was conducted to show the demographic characteristics and lifestyles of the mothers, fathers, and newborns. Small for gestational age (SGA) babies are those who are smaller in size than normal for their gestational age. In this study, SGA was defined as a weight below the 10th percentile for gestational age. We evaluated the relationships among maternal height, LBW, and NICU admission. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated using logistic regression. The two outcomes of LBW and NICU admission appeared to be correlated, and we ran three logistic regression models: model 1 was not adjusted (crude model); model 2 was adjusted for maternal age, maternal BMI at baseline, maternal smoking habits, paternal smoking habits, maternal alcohol drinking habits, and maternal occupational status (fully adjusted model); and model 3 was adjusted for LBW in addition to the variables in model 2. Model 3 was designed to determine whether LBW played a role in the relationship between maternal height and NICU admission because newborns with LBW are more likely to be cared for in a NICU environment. We used SPSS version 20.0 for Mac OSX (IBM Japan, Tokyo, Japan) to conduct all of the statistical analyses in this study.
Ethical statement
This study was approved by the institutional review board of Okayama University on November 29, 2011 (No. 498), as well as the institutional review board of Seirei Hamamatsu General Hospital. At Seirei Hamamatsu General Hospital, the administrative staff usually informs the patients that individual medical records may be used for clinical and epidemiologic research and that patients can refuse to allow their records to be included at any time. We strictly followed the clinical research guidelines at Seirei Hamamatsu General Hospital with respect to the usage of individual information.
RESULTS
Descriptive analysis
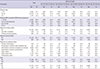
The demographic characteristics and lifestyle habits of study participants are shown in Table 1. Mothers of shorter height were more likely to have LBW newborns, and these newborns were more likely to experience NICU admission (11.4% and 12.1%, respectively). Younger mothers (< 25 years old) were more likely to have LBW newborns, and these newborns were more likely to be admitted to the NICU (9.6% and 11.1%, respectively); older mothers (> 35 years old) showed a similar pattern (8.7% and 10.4%, respectively). A lower maternal BMI was more likely to be associated with LBW. By contrast, a BMI greater than 25.0 was more likely to be associated with NICU admission. Mothers who smoked during pregnancy were more likely to have LBW newborns and newborns admitted to the NICU (12.4% and 15.6%, respectively). There were no significant differences in the distribution of maternal alcohol drinking habits or maternal occupational status with LBW and NICU admission. Approximately 60% of LBW newborns were classified as SGA. Descriptive data divided by each quartile point of height (Q1 to Q4) are shown in Table 2. The women in the shortest group (Q1) were more likely to have SGA and LBW babies than taller women. By contrast, the women in the tallest group (Q4) were more likely to have non-SGA/non-LBW babies than shorter women. There were no obvious differences between the 4 height groups regarding the distribution of other lifestyles or characteristics.
Table 1
Description of study participants who gave birth after 37 gestational weeks (n = 17,150)
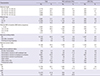
Table 2
Description of study participants by maternal height at quartile points (n = 17,150)
Maternal height and LBW
The relationship between maternal height and LBW was also evaluated (Table 3). In model 1, the shortest maternal height quartile (Q1) was related to LBW (OR 1.91 [CI 1.64, 2.22]). The second shortest (Q2) and third shortest (Q3) maternal height quartiles were also related to LBW (1.31 [1.12, 1.53] and 1.20 [1.01, 1.41], respectively). The results of the adjusted ORs and 95% CIs are shown in Table 2. In model 2, the height of mothers in Q1 remained related to LBW (2.00 [1.71, 2.34]), and the height of mothers in Q2 and Q3 was also related to LBW (1.33 [1.13, 1.57] and 1.20 [1.01, 1.43], respectively). These results showed that the association remained after adjusting for potential confounders. We also conducted an analysis with continuous values of one quartile change. We performed this analysis using the original height value (cm); the relationships between shorter maternal height and LBW were also found in both of these analyses (P < 0.01).
Table 3
Adjusted odds ratios and confidence intervals for the relationship between maternal height and LBW (n = 17,150)
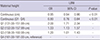
The model adjusted for maternal age, maternal BMI at baseline (BMI before pregnancy), maternal smoking habits, maternal alcohol habits, and maternal occupation status (the ORs and CIs for the covariates are not shown). Maternal age was entered into the model in 2 ways: (1) individual age minus the mean age of the group and (2) (individual age minus the mean age of the group)2. Q, quartile; NICU, neonatal intensive care unit; LBW, low birth weight; SGA, small for gestational age; OR, odds ratio; CI, confidence interval.
Maternal height and NICU admission
With regard to the risk of NICU admission, crude ORs with 95% CIs were estimated using logistic regression (model 1, Table 4). The shortest maternal height quartile (Q1) and the second shortest maternal height quartile (Q2) were related to NICU admission (1.47 [1.27, 1.69] and 1.17 [1.02, 1.35], respectively). However, maternal height of the Q3 group was not related to NICU admission. In model 2, adjusted ORs and 95% CIs between maternal height of Q1 and Q2 and NICU admission remained related (1.48 [1.27, 1.71] and 1.20 [1.04, 1.39], respectively); however, no relationship was found for Q3.
Table 4
Odds ratios and confidence intervals for the relationship between maternal height and NICU admission in 3 models (n = 17,150)
Model 1: maternal height adjusted for maternal age. Model 2: maternal height adjusted for maternal age, maternal BMI at baseline (BMI before pregnancy), maternal smoking habits, maternal alcohol habits, and maternal occupation status. Model 3: in addition to model 2, adjusted for LBW. Maternal age was entered into each model in 2 ways: (1) individual age minus the mean age of the group and (2) (individual age minus the mean age of the group)2. In model 3, the ORs and CIs for covariates are not shown (with the exception of LBW). Q, quartile; NICU, neonatal intensive care unit; LBW, low birth weight; SGA, small for gestational age; OR, odds ratio; CI, confidence interval.
Model 3 was conducted to investigate the relationship between maternal height and NICU admission. When the model was adjusted for LBW, the ORs between maternal height in Q1, Q2, and Q3 and NICU admission were decreased, and there was no relationship between maternal height and NICU admission.
DISCUSSION
The current study found that among mothers who had full-term births (birth after the 37th gestational week), shorter maternal height was associated with LBW. This relationship was stronger among the quartile of mothers with the shortest height. A relationship between maternal height and NICU admission was also found in this study. However, this relationship was fully attenuated when the statistical model was adjusted for LBW. Therefore, LBW is involved in the relationship between maternal height and NICU admission. The relationship between maternal height and LBW was strong. This finding suggests that smaller newborns are more likely to be admitted to NICU and that the association between maternal height and NICU admission is not direct.
Witter and Luke (5) reported that shorter women are more likely to have smaller newborns than taller women. This previous study was conducted with participants in the United States; the results are consistent with our study results. Wills et al. (4) demonstrated a relationship between parental height and fetal growth in the United Kingdom. However, there was no clear association between maternal height and lower birth weight. Nutritional status is similar in these three countries; food supplies in the United States, the United Kingdom, and Japan are stable at the national level. Therefore, shorter height may not be a proxy for undernutrition; rather, it is more influenced by heritable factors or other environmental factors.
Mothers who are short in height may have a narrow pelvis, resulting in limited intrauterine space. This may restrict intrauterine fetal growth (171819). Differences in the size of the pelvis depend on differences in individual body size, and this mechanism may be common in any setting. However, this is insufficient to explain the mechanism of the relationship between maternal height and LBW. There may be other reasons why the growth of newborns is restricted.
One strength of our study is that we investigated all of the deliveries at one hospital during the period of 1997 to 2010 and had more than 17,000 participants, which may reduce selection bias. Furthermore, the large sample size should provide sufficient power to detect clinically relevant associations. Another strength is that the definition of LBW (birth weight < 2,500 g) is common and easy to compare with other study results. Additionally, the measurement of maternal height and LBW rarely induce misclassifications because of accurate measurement tools for body size in Japan; this advantage expands the comparability of our study results.
There were also some limitations. First, this study was conducted using a dataset from one regional hospital in Japan, Seirei Hamamatsu General Hospital. Additionally, the hospital provides advanced medical intervention and typically accepts high-risk pregnant women and patients in emergency situations. This situation can cause bias. Therefore, the generalizability of this study is limited. Second, NICU admission was a substitute indicator of poor birth outcome (i.e., poor condition of newborns). The reasons for NICU admission are varied and may differ at the hospital/institute level or physician level. This leads to non-differential misclassification, with odds ratios toward the null value. However, there is no exact classification for the indication of NICU admission. Therefore, this misclassification could happen by chance in any setting and would not cause significant bias. Third, the Japanese universal health care system is unique, and each country has different health insurance options for maternity care. However, we could not consider the effect of health insurance in this study. Furthermore, we did not consider the effect of undernutrition alone in this study because Japan is a developed country with a stable food supply. Generally, undernutrition status is related to household income (i.e., low-income status in Japan); other reasons for undernutrition involve individual diseases, including gastrointestinal disease, cancer, and eating disorders. However, we did not obtain information on household income or disease status. Only occupational status was used as a measurement of SES. Additionally, information regarding dietary habits was not collected in this study. Thus, we could not consider the effect of these variables related to individual nutrition status. Therefore, we could not draw conclusions about the effects of short stature on birth weight or nutritional status.
In conclusion, our findings may suggest that being born small in Japan is more reflective of genetics/biology than social factors such as nutrition status. Shorter mothers in developed countries (who are likely not short due to nutritional deficits) provide a useful prenatal target to anticipate and plan for subsequent LBW and NICU admission. Maternal height as a screening measurement may become a useful indicator in developed and developing countries.
 XML Download
XML Download