

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In general, falling is an important problem among the elderly. In previous studies, one-third of persons aged over 65 years and half of those aged over 80 years experienced at least one fall during a 1-year period (123). Muscle weakness, postural imbalance, loss of visual or auditory acuity, cognitive dysfunction, female gender, increasing age, fear of falling and polypharmacy are known falling risk factors (45). A recent study reported that living alone, living in an urban area, poor self-rated health and high stress were also significantly associated with the risk for falls in the older Korean adults (6). An estimated 10–20 million people worldwide had contracted poliomyelitis and are still alive, including 60,000–80,000 in Korea (78).
Decades after an acute paralytic poliomyelitis infection, many people experience new symptoms or impairments, which are referred to as late effects of polio or post-polio syndrome (9). Late effects of polio are one of the most common neuromuscular conditions that can lead to a disability. They include a variety of new musculoskeletal, neurological, and systemic symptoms, such as muscle weakness, muscle or generalized fatigue, and pain during activity and cold intolerance (10). Among them, muscle and joint pain, cold intolerance and fatigue may contribute to the occurrence of falls for polio survivors (11). Previously published studies have shown that 50%–84% of persons with late effects of polio reported at least one fall during the past year (12). This year-fall incidence is considerably higher than that in elderly people, in whom it is 17%–23% for people over 55 years of age and 32%–42% for those over 75 years of age (13). Polio patients with late effects experienced a fracture as a consequence of their falls 35%–40% of the time (1314).
Despite the fact that falling and the consequences thereof are clinically important and significant health issues among polio survivors, those problems have been underrated and few studies have investigated the frequency of falls and factors associated with falls in this population. Most reports dealing with fall incidence and risk factors have utilized European and American polio survivor populations (121315). To our knowledge, detailed findings regarding falls and fall-related features of polio survivors in sufficiently large samples have not been reported previously in an Asian country, including Korea. An increased knowledge of falls, fear of falling, and factors associated with falls could facilitate design of individually targeted rehabilitation interventions to reduce falls and fear of falling in persons with late effects of polio.
The purpose of this study was to determine the incidence of, and consequences and factors associated with falls among Korean polio survivors.
MATERIALS AND METHODS
Subjects
The subjects consisted of persons previously diagnosed with poliomyelitis or poliomyelitis with post-polio sequelae. They were identified by searching the medical records of Seoul National University Bundang Hospital, Seoul National University Hospital, SMG-SNU Boramae Medical Center, National Rehabilitation Center, Chonnam National University Hospital, Gyeongsang National University Hospital, Ewha Womans University Hospital (EWUH), Hwaseong City Health Center (HCHC) and Jeongnip Welfare Center, from which contact information—such as names, addresses, telephone numbers, etc.—was obtained. When patients were contacted to obtain consent for study participation, the past medical history of infection of poliomyelitis was confirmed again before asking them to participate. Following agreement to participate in the study, a structured questionnaire was administered to the subjects over the telephone. All participants completed a questionnaire including fall history, symptoms related to post-polio syndrome (PPS) and other information through telephone interview.
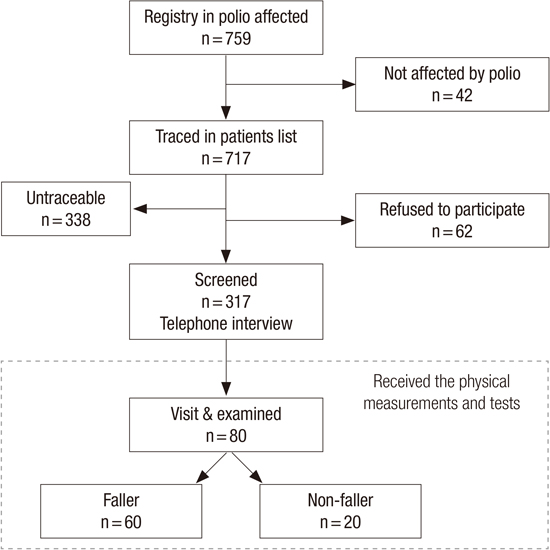
A total of 759 polio survivors was registered in our database. This number represents approximately 1% of estimated polio survivors extracted from the database of the ‘National Survey of Persons with Disability 2011’, which is a survey conducted by the Korean government every 5 years. However, 42 persons were considered to not fit the diagnostic criteria for poliomyelitis after the initial review of medical records. Three hundred and thirty-eight subjects could not be contacted because of inaccurate or old telephone numbers in the records. Sixty-two persons declined to participate in the interview. As a result, a total of 317 polio survivors completed the questionnaires by telephone interview (response rate, 83.6%). The flow chart for identifying patients affected by a fall is shown in Fig. 1.
During the interview, we informed participants of the purpose of this study: to establish a middle-aged cohort for late effects of polio survivors in Korea. Among the participants who responded to the telephone interview, 80 polio survivors visited our clinic to receive the additional physical measurements and tests such as anthropometric measurements, musculoskeletal examinations and various functional evaluations related to late effects of poliomyelitis.
Telephone questionnaire
A structured questionnaire was administered by trained interviewers. The questionnaire was developed by modifying and integrating several previous questionnaires used to assess post-polio syndrome, late effects and fall history and fall consequences (1617).
The polio-specific questionnaire administered to participants in this study contained detailed questions about the onset age of poliomyelitis and whether upper and/or lower limb(s) were paralyzed. Participants were also asked about the presence or absence of newly developed symptoms that reduced physical function, such as fatigue, weakness, and/or pain related to post-polio syndrome (PPS), and when those symptoms began. In this way we determined the interval between onset of acute poliomyelitis and that of symptoms related to PPS. Use of orthotics or walking aids, current ambulatory functions, the disability rating registered to national welfare system, past medical history including surgical treatments, and medical comorbidities were evaluated.
In fall-related questionnaire, a fall was defined as an unexpected event that resulted in the participant coming to rest on the ground, floor, or a lower level. The participants were asked whether they had experienced a fall to the floor, ground, or a lower level in the previous 1 year. We also asked fallers how many incidents there had been during the past year and the causes of the incidents (e.g., a slip, trip, or collision). Fallers were also asked what they were doing at the time of the fall, where they were, and injury types and injury sites.
The questionnaire on general health and socioeconomic status included self-reported health status and socioeconomic status such as marriage, cohabitant, residence, religion, academic background, monthly family income and occupation. It consisted of 39 questions. Some patients declined to answer some of the questions despite having consented to participate in this study. Those answers were categorized as missing values. The diagnostic criteria for PPS, adopted from the European Federation of Neurological Societies (EFNS), were as follows: 1) prior paralytic poliomyelitis with evidence of motor neuron loss, as confirmed by history of acute paralytic illness, etc.; 2) a period of partial or fairly complete functional recovery after the acute paralytic poliomyelitis, followed by an interval (usually of 15 years more) of stable neurological function; 3) gradual or sudden onset of progressive and persistent muscle weakness or abnormal muscle fatigability (decreased endurance) with or without generalized fatigue, muscle atrophy, weakness in the limb(s), or muscle and joint pain; 4) symptoms persisting for at least 1 year; and 5) no other possible causes that could be producing PPS symptoms (18). Subjects who met all of these criteria were categorized into the PPS group. Subjects who had cerebrovascular diseases were excluded from the PPS group because their newly developed symptoms might not be related to PPS.
Physical and functional evaluation
Physical and functional parameters were evaluated for 80 polio survivors who agreed to visit the clinic. As basic anthropometric assessments, height, weight, body mass index and average bone density (by Dual-energy X-ray absorptiometry [DXA]) were measured. We identified leg-length discrepancy with measurement from the anterior superior iliac spine (ASIS) to the distal tip of the medial malleolus (SMD) and from the umbilicus to the same distal leg point (UMD) with the standard tape measures.
Short Performance Physical Performance Battery (SPPB)
SPPB was used to assess physical performance. The SPPB consists of three basic items: balance, walking velocity, and sit to stand. Participants were first asked to balance in standing positions with their feet side-by-side, semi-tandem, and fully tandem for 10 seconds each. Participants were then asked to walk a distance of 4 m at their usual pace. Finally, participants were asked to stand from a sitting position in a chair and return to the seated position five times as quickly as possible while keeping their arms folded across their chest. Based on normative data, each of these tasks was scored on a scale from 0 to 4. The sum of the three sub scores yielded the total SPPB score, ranging from 0 (worst) to 12 (best function).
Activity confidence
The Activities-specific Balance Confidence Scale (ABC) was designed to evaluate confidence in activities related to balance (1920). Balance confidence represents an important assessment because the balance function is essential in daily activities. The ABC scale, presented in questionnaire format, is used to investigate balance confidence in community-dwelling elders. This includes 16 items representing basic tasks involved in daily living (walking around the house and going up and down stairs) and more difficult tasks.
Knee strength
The isokinetic muscle strength of the knee extensors and flexors was measured at an angular velocity of 60°/second using an isokinetic dynamometer (Biodex Isokinetic Tester, Biodex Medical Systems, Shirley, NY, USA). Participants were asked to perform two sets of five repetitions with a 30-second rest between sets. They were asked to perform the test by exerting maximum pressure on the isokinetic arm through the entire range of movement. The concentric peak torque values (N·m) obtained from five torque-angle curves in each set were used to evaluate the flexion/extension muscle strengths of knee joints.
Statistical analysis
All statistical analyses were performed using IBM SPSS Statistics version 20 (IBM Corporation, Armonk, NY, USA). Missing or unclear answers in the questionnaires and rating scales were amended by telephone interviews when possible. Demographic data and clinical characteristics were presented as means and standard deviations (SD), or medians and interquartile ranges. Main outcome measures were fall frequency, situations, causes, circumstances relating to falls, injuries sustained during a fall, and scores on the SPPB, confidence using ABC, BDI, BMD, isokinetic muscle strength and leg length using SMD and UMD. Differences in the variables and rating scales between persons who did and did not fall were subjected to multivariate linear regression analysis. Results are presented as odds ratio (OR) with 95% confidence intervals (CIs). We also evaluated possible multiple collinearities between covariates by correlation analysis and collinearity statistical tests (tolerance and variance inflation factor tests), as suggested for logistic regression. Significance level was set at P < 0.05.
Ethics statement
The protocol of this study complies with the Declaration of Helsinki. All participants were fully informed regarding study participation and provided written informed consent. The study including this consent procedure was approved by the institutional review board of Seoul National University Bundang hospital (IRB No: B-1112-142-003).
RESULTS
Demographic characteristics
The demographic and etiologic characteristics of participants are summarized in Table 1. The mean age of polio survivors was 51.2 ± 8.2 years (median 52, range 19–80) and 190 (59.9%) were over 50 years old; 177 (55.8%) were female. The mean age at onset of polio symptoms for the entire population of subjects was 2.4 ± 1.8 years (median 2, range 0–12). More than half, 167 (52.7%) of the subjects suffered from acute poliomyelitis at or before 2 years old. However, 10 subjects did not remember the onset of poliomyelitis and 4 subjects were not diagnosed as having had poliomyelitis when they had acute infection; their infection was diagnosed during the stable period after recovery from the acute stage.
Table 1
General characteristics of study participants
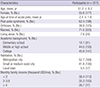
A total of 62.4% of the subjects (n = 198) met the adopted diagnostic criteria for PPS of the European Federation of Neurological Societies (EFNS), commonly used to diagnose PPS (18). A total of 38.8% of the subjects (n = 123) used orthoses. Regarding social characteristics, the majority of participants were married (71.0%), and a few were living alone (7.6%).
Among the respondents, 45.9% of the subjects received college education or higher education. About half of the subjects lived in a metropolitan city (52.7%) and the rest lived in a small or medium sized city or a local town. Monthly family incomes were found to vary among the subjects. About two-fifth of their families made less than one thousand USD per month (38.4%).
Incidence and consequences associated with falls in Korean polio survivors
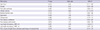
Fall-related features among Korean polio survivors are summarized in Table 2. Among a total of 317 polio survivors, 217 subjects (68.5%) reported at least one fall in the past year. Of the 217 fallers, 90 subjects (42.5%) experienced at least one fall during one month, 50 (23.6%) did at least once during one week and 11 (5.2%) did at least once during one day. Most falls occurred during ambulation (76.6%) and outside (75.2%). Of the fallers, 76.6% reported that they had fallen while flatland walking. There were only a few falling situations, usually occurring when climbing stairs up and down, using a walker, using a wheelchair, sitting up and down and riding a bike. The rate of falls experienced outside was threefold higher than that inside. As a cause of fall, the subjects reported slipping down (29.7%), spontaneous leg weakness (29.0%), tripping (25.2%), misstep (8.4%), collision (1.3%) and others (6.5%).
Table 2
Fall-related features in polio survivors: frequency, situation, environment, cause, consequences and type of injuries

In addition, 45.0% of the polio survivors who experienced a fall in the past year had been injured as a consequence of the fall. The common sites of injury were lower extremities (61.8%), upper extremities (24.5%), lower back (4.5%), chest (2.7%), abdomen and pelvis (2.7%), face (2.7%), and head (0.9%). The type of injury most commonly reported after the falls was bruises, which were reported by more than one quarter of the injured. Individuals with bony fractures comprised 23.3% of the injured cases and 9.7% of the fallers. Other injuries included abrasion (13.3%), sprain (10.0%), and laceration (3.3%). Of the fallers, 10.8% experienced serious injuries, such as a fracture or large laceration that required hospital care.
Factors associated with falls
The data from 80 participants who underwent physical measurement and functional evaluation were used to determine the risk factors associated with falls in polio survivors. In Table 3, the data for the ‘fallers’ (i.e., those that reported at least one fall during the past year) and ‘nonfallers’ (i.e., those that did not report any falls during the past year) are presented. There were no significant differences between fallers and non-fallers in age, gender, proportion of post-polio syndrome, physical performance score by SPPB, Beck depression index and modified Barthel index score.
Table 3
Demographics and characteristics of ‘fallers’ and ‘non-fallers’ among 80 participants who received additional physical measurements and tests

The percent use of orthoses user among the fallers was 45.4%, compared to 25.0% among the non-fallers (P < 0.05). Orthotic devices used widely among polio-survivors were crutches (35.7%) and knee-ankle-foot-orthoses (35.7%). The ABC score of fallers (55.0) was slightly lower than that of non-fallers (61.4).
The knee extension peak torque of the uninvolved limb in fallers was 37.9 N·m, and of the involved limb was 9.1 N·m. The knee extension peak torque of the uninvolved limb in non-fallers was 42.9 N·m, compared to 14.7 N·m in the involved limb. In both cases, the peak torque of the knee extensor in fallers was slightly less than that of non-fallers.
The average bone marrow density in fallers (n = 59) was -0.34, but that in non-fallers (n = 20) was -0.43. Among the fallers, 14 subjects (23.73%) were diagnosed with osteoporosis (T-score equal or less than -2.5), compared to 6 (30%) among non-fallers.
Leg length was measured by SMD and UMD. By SMD, the faller’s limb length discrepancy was greater, 3.8 cm (4.9% of the long leg) compared to 1.4 cm for the non-fallers (1.9% of the long leg). By UMD, the faller’s limb length discrepancy was 2.1 cm (2.5% of long leg), but that of the non-fallers was 1.6 cm (1.9% of the long leg). Limb length discrepancy measured by SMD was significantly greater in fallers than non-fallers (P = 0.026).
Risk factors associated with falls in polio survivors
Multiple logistic regression analysis of risk factors for falls in Korean polio survivors is shown in Table 4. No significant collinearity was identified for any of the covariates in statistical tests of collinearity. Only leg-length discrepancy using SMD was significantly associated with falls in polio survivors. Female sex, old age, low BMD, the presence of symptoms related to PPS, poor balance confidence, short physical performance battery and weak muscle strength of knee extensor were not significantly associated with falls, after adjusting for the influence of multiple confounding variables. The odds ratio of leg-length discrepancy was 3.30 and 95% confidence interval was 1.62-6.71.
Table 4
Multiple logistic regression analysis of risk factors for falls in Korean polio survivors
DISCUSSION
This study is the first to report the frequency and characteristics of falls and to analyze risk factors associated with falls in Korean polio survivors. Over two thirds (68.5%) of patients reported at least one fall during the past year and a total of 42.5% of polio survivors experienced a fall more than once per month. Most falls occurred during flattened walking (76.6%), outside (75.2%) and by slipping down (29.7%). These findings indicate that the issues of fall and fall consequences that polio survivors experienced should not be overlooked among the health problems in persons with disabilities. Among polio survivors with recent experience of fall, 45.0% reported that they experienced injury from the fall and 23.3% reported falls resulting in bony fracture. In the multiple logistic regression analysis, leg-length discrepancy using SMD was found to be significantly associated with falls in polio survivors.
The high fall frequency in our population is in agreement with other studies (12132122), in which it was noted that 50%–84% of persons with late effects of polio report at least one fall during one year. Thus, the frequency of falls in persons with late effects of polio seems to be three- to four-fold higher than that in patients with neurodegenerative diseases, such as chronic stroke, Parkinson’s disease, and multiple sclerosis (12). Compared with the rate of fall in community-indwelling Korean elderly from the data of one study (23), the incidence of fall was up to five-fold higher in polio survivors (68.5% vs. 13.0%). Most falls occurred while walking outdoors. Similar findings were described by Bickerstaffe et al. (13), who found that most of the falls occurred in a familiar environment, during ambulation, and in the afternoon. About one quarter of fallers experienced a fall at least once per week and 20% of them fell at least once per day. It appears that recurrent fall frequency is a serious problem and can lead to multiple sequelae from minor trauma to severe injuries, such as fractures.
The most commonly reported injury after falls was minor trauma (bruises, lacerations, sprains, and contusions); however, only 9.7% had sustained a fracture. Bickerstaffe et al. (13). also found that two thirds of the fallers in their population had sustained a minor injury (such as bruises, scrapes and sprains), whereas 7% had sustained a fracture. Hill and Stinson (22) reported that bruises or grazes (44%) were the most common injuries after falls and that fractures were uncommon. However, decreased mineral bone density and osteopenia are present in polio survivors with late effects of polio (14). Therefore, persons with late effects of polio could be considered at high risk for fractures. Moreover, this study shows that fracture occurred among 23.3% of the injured. In comparison with the community-indwelling Korean elderly persons studied by Lim et al. (23), the incidence of fall was considerably higher in polio survivors (23.3% vs. 16.7%, respectively). Although 20 of the 79 subjects in whom BMD was evaluated (25.3%) were diagnosed with osteoporosis, the majority had low mineral density only in their polio-related hip. The average spine T-score was -0.51, but that of the hip was -1.51 in the 79 polio survivors. Similar results were described by Chang et al. (24), who found that men with poliomyelitis had significantly lower femoral neck BMD in both legs, and femoral neck BMD was lowest in their shorter legs.
In our study, we found that limb-length discrepancy was a significant risk factor for fall in polio survivors. The rate of falling was threefold higher when the leg-length discrepancy increased beyond 1 cm (OR, 3.30; 95% CI, 1.62-6.71). This is the first report that limb length discrepancy is a risk factor for fall in polio survivors. One study reported 32 skeletally mature poliomyelitis patients managed using the Ilizarov technique and external fixation for limb lengthening (25). Lengthening did not change the functional mobility score used to assess ambulation before lengthening and at the final follow-up. Although the correction of unequal limb length did not enhance gait performance and mobility function, it may contribute to preventing falls and fall-related injuries. Limb length discrepancy can be divided into 2 etiological groups: true limb length discrepancy, defined as those who are associated with shortening of bony structures, and apparent limb length discrepancy, defined as those who are the result of altered mechanics of the lower extremities (26). True or anatomical limb length discrepancy is usually measured with SMD and apparent or functional limb length discrepancy is determined with bilateral difference of UMD (27). Limb-length discrepancy of fallers by SMD was significantly greater than that of non-fallers by SMD and UMD, but there were no meaningful differences between SMD and UMD in non-fallers. As apparent limb length discrepancy is compensated by pelvic obliquity and functional scoliosis, it may have relatively small range of interpersonal differences compared to true limb length (SMD). Greater SMD difference requires higher compensation which can lead to make functional lumbopelvic deformity worse. Therefore, above findings may be the reason why the discrepancy of SMD was more significant risk factor of fall than that of UMD. Reducing the faller’s discrepancy in SMD (3.8 cm), which can be achieved by shoe modification, may be an effective management strategy. In general, leg length discrepancies of less than 0.5 inch do not need correction and the total discrepancy is never corrected. At most, 75% of the leg length discrepancy should be corrected. The first 0.5 inch of the discrepancy can be managed with a heel pad or insole. Additional correction requires the heel to be built up externally. The sole should also be built up proportionally when the heel is built up externally to provide a comfortable, stable gait (2829).
In the present study, balance confidence was assessed using the ABC score (19), which contributed significantly to the prediction of falls with 89% sensitivity and 96% specificity (30). Our results showed that the fallers worried more about balance loss than did the non-fallers when performing daily activities, such as walking on a slippery or uneven surface, up or down a slope, or up or down stairs. However, overall ABC score was not statistically significantly different. In previous studies using the fall efficacy scale (FES) in persons with late effects of polio, fear of falling was commonly reported during activities related to walking but also when taking a bath/shower, cleaning the house, and other activity of daily livings (1213). In addition, we investigated how leg strength determined quantitatively by isokinetic test was related to falls in polio survivors because the knee extensor strength has been a well-known factor for fall prevention. However, knee extensor peak torque was not a significant factor after controlling for the effects of confounders. According to our results, both faller and non-faller group had very weak muscles at the affected limbs. This could be the reason why two groups had no significant difference of knee strength. The causes of fall in polio survivors are multifactorial. There have been several studies reporting risk factors of fall in polio survivors such as muscular weakness of weaker leg, fear of falling, maintaining balance, self-reported impairments and walking limitations (121331). Our study suggests that there may be an additional role of malalignment between the paralytic and non-paralytic limb length in the occurence of falling. Nevertheless, in previous studies (121331) balance and knee extensor strength have been shown to exacerbate the risk of falling, and therefore it is still important clinically to emphasize balance training and knee extensor strengthening exercise in persons at risk for falls.
The major limitation of this study was that the results of the survey were obtained via a telephone interview. The average time to complete a survey for each subject was ~30 minutes. This may have affected the compliance of participants in the survey. In addition, given the cross-sectional design of this study, its ability to determine a causal relationship between risk factors and fall history is limited. However, because there are some factors (i.e., leg-length discrepancy) existing obviously prior to fall experience, we were able to address the causality of the relationship despite the limitations of cross-sectional evaluation.
This study showed that falls were common in persons with late effects of polio, and that falls occur mostly during even-surface walking outdoors. Reducing falls of this population were formerly a main target of rehabilitation professionals, but lack of knowledge of the effectiveness of various fall management programs has been a major barrier in this population. In elderly persons (32), multifactorial interventions targeting strength, balance, home hazards, vision, footwear, drugs, cognition, and education may reduce falls and/or risk of falling. In patients who have had a stroke and are living in the community (33), interventions such as task-specific exercise programs to improve balance and walking ability have been shown to reduce the number of falls. However, designing fall management programs for persons with late effects of polio is challenging. We have found that conventional balance and strength training is less effective for paralyzed lower extremities. Given the multifactorial nature of many falls, a multidisciplinary approach would be more effective in terms of reducing impairments, activity limitations, and participation restrictions. Moreover, appropriate orthotics, such as insoles or shoe modifications, are essential to prevent falls and fall-related injuries. The design, implementation, and outcome of fall management programs in this population should be further investigated.
Fall prevention strategies in polio survivors should focus specifically on the mechanisms of fall. Reducing falls and the risk factors thereof, including leg length discrepancy, using multidisciplinary fall management programs will enable persons with late effects of polio to maintain a healthy lifestyle and increase their physical activity.
 XML Download
XML Download