

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Marfan syndrome is an autosomal dominant connective tissue disorder characterized by a mutation in the fibrillin I gene (1). Its prevalence is approximately 2-3 per 10,000 individuals (1). The phenotype of Marfan syndrome varies widely to include many organs including the eyes, heart, aorta, skeleton, skin, and lung (2).
Two common features of Marfan syndrome include excessive linear growth and tall stature. Excessive linear growth starts prenatally. Patients with Marfan syndrome then have an earlier, and more rapid puberty-associated growth spurt compared to the general population (3). This rapid growth is of clinical concern because it can aggravate aortic dilatation (4) and is also associated with a high prevalence of scoliosis development (5). Excess growth can also impair physical and psychological well-being in affected adolescents and adults. Therefore, it is necessary to seek methods by which this growth can be controlled.
Treatment with high dose estrogen has been shown to slow linear growth in constitutionally tall girls (678). Similarly, efforts have been made to control linear growth using sex steroids in Marfan syndrome. However, there are limited published data regarding height control with high dose estrogen in Marfan syndrome (9101112), and ethinyl estradiol was used in most studies. Although the types and doses of estrogens vary in the literature (91012), 50-300 µg of ethinyl estradiol per day is commonly used for height control in girls with Marfan syndrome (1112). Unfortunately, however, ethinyl estradiol has a strong metabolic effect. Therefore, there are some concerns regarding its use, especially at high doses. Estradiol valerate is more physiologic than is ethinyl estradiol (13). In addition, ethinyl estradiol is only available in combination with progestin in Korea.
The aim of this study was to evaluate the efficacy of a stepwise increasing regimen of estradiol valerate for height control in girls with Marfan syndrome.
MATERIALS AND METHODS
Patients
Patients who were diagnosed with Marfan syndrome according to the revised Ghent criteria (14) and who had visited an adolescent gynecologic clinic at Samsung Medical Center for height control between October 2004 and May 2014 were considered for inclusion. Patients were excluded if they were still undergoing estrogen treatment, did not reach their final height during the study period, or were lost to follow-up during treatment. Ultimately, eight patients were included in the data analysis.
Estrogen treatment
In every case, the decision for treatment was made based on the preferences of the patients, their caregivers, and advice from pediatricians. Before treatment, patients were educated regarding the predicted adult height, expected range of height reduction, and the potential side effects of treatment. The age of treatment initiation was determined on a case-by-case basis at the earliest opportunity when both the patient and parents agreed.
Initially, estradiol valerate (Progynova®, Bayer Schering pharma AG, Berlin-wedding, Germany) was administered orally at a dose of 2 mg/day for 6 months. After the first six months, the dose was increased every 2 months by 2 mg/day. The dose was adjusted until the height increment was <1 cm for 2 months. This final dose was then maintained until the patient reached her final height. Once a patient reached 4 mg/day of estradiol valerate or if breakthrough bleeding occurred, 10 mg/day of oral medroxyprogesterone acetate was added to the treatment regimen for days 1-12 of each calendar month. Addition of progestogen was delayed to allow for normal breast and uterine development. One patient was already Tanner stage 3 at the start of the study. In this case, estradiol valerate was initiated at a dose of 4 mg/day, and then was increased according to the same stepwise schedule. When a girl was suspected to have reached her final height, x-rays were used to confirm fusion of the epiphyseal plate. After this confirmation, the dose of estradiol valerate was gradually reduced. Fig. 1 illustrates the treatment schedule.
Measurements
A stadiometer was used to measure standing height at the start of the study, and then every two months (GL-310P, G-tech international, Uijungbu, Korea). The Korean Marfan syndrome-specific growth curve (growth curve) (15) was used to calculate each patient's initial height percentile. The projected final height (PFHt) was estimated by the height at 16 years old using the same baseline percentile on the growth curve, because the height at this age represents the maximum point on the curve (gcPFHt). The PFHt was also estimated using the baseline bone age before estrogen treatment (baPFHt). The final height (FHt) was defined as that when the bone age was at least 15 years old. When a patient had reached her FHt, the difference between the PFHt and FHt was calculated. Tanner staging was used to measure puberty (16). The initial serum estradiol level was also measured. The Greulich and Pyle method was used to measure bone age before starting treatment and after reaching the final height (17).
RESULTS
The patients' baseline clinical features are shown in Table 1. Five of the 8 patients had one or more relatives affected by Marfan syndrome. Seven of the patients had the fibrillin I gene mutation. Six had skeletal problems including scoliosis or chest wall deformities. Seven patients had either aortic root dilatation or ectopia lentis. None of the patients had undergone menarche, and all but one patient were in Tanner stages 1 or 2.
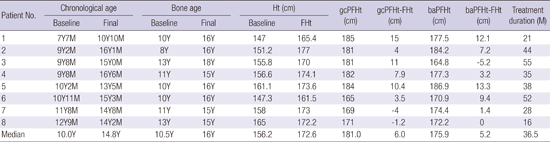
The changes in height parameters after estrogen treatment are presented in Table 2. The median baseline chronological age and bone age were 10.0 (ranged 7Y7M-12Y9M) and 10.5 (ranged 8-13Y) years, respectively. After a median of 36.5 months (ranged 16-55 months) of estrogen treatment, the median FHt (172.6 cm) was shorter than were the median gcPFHt (181.0 cm) and baPFHt (175.9 cm).
The median chronological age and bone age of patients who began the estrogen treatment before the age of 11 (patient no. 1-6) were 9.8 years (ranged 7Y7M-10Y11M) and 10 years (ranged 8-13Y), respectively. After a median of 41 months (ranged 21-55 months) of treatment, the FHt (median: 171.8, range: 161.5-177 cm) was shorter than were the gcPFHt (median: 181.5, range: 165-185 cm) and baPFHt (median: 177.4 cm, range: 164.8-186.9 cm). The median differences between the FHt and gcPFHt and baPFHt were 9.2 cm (ranged 3.5-15 cm) and 8.3 (ranged -5.2-13.3 cm), respectively. In patients who started treatment after the age of 11 years (patient No. 7 and 8), the differences between FHt and gcPFHt and baPFHt after treatment were -4 and 1.4 cm (patient No. 7) and -1.2 and 0 cm (patient No. 8), respectively.
Fig. 2 shows annual percentile change plotted on growth curve. In five patients (patient No. 1-5) who were in 80 or more percentile (median, 85; range, 80-92 percentile) on growth curve before treatment, percentile decreased to 47 percentile in median after treatment. In contrast, in two patients who started treatment after the age of 11 (patient No. 7 and 8), percentile on growth curve did not decrease with estrogen treatment.
DISCUSSION
This study evaluated the efficacy of estrogen for height control in girls with Marfan syndrome, and revealed that a stepwise regimen of estradiol valerate may be an effective option. The median difference between the predicted and actual final height after estrogen treatment was 6.0 cm by disease specific growth curve, and 5.2 cm by bone age. In the six girls who started estrogen treatment before the age of 11 years, the median difference was 9.2 cm by disease specific growth curve and 8.3 cm by bone age. These results are similar or more favorable to those of previous studies that compared the heights of treated and untreated girls with Marfan syndrome (1112).
In this study, we sought to start estrogen treatment as early as possible. The mean chronological age at treatment initiation was 10 years. The mean final height was 172.6 cm. In two previous studies, the ages at treatment initiation were 12.4 (11) and 11.4 years (12). The mean final heights in these studies were 184.1 (10) and 181.5 cm (11). The mean final height in our study was shorter than that of other studies. This increased height control may be a result of earlier treatment initiation in our study, compared to in others. Similarly, we found that there was remarkable final height reduction in girls who started treatment before the age of 11; however, those who started after age 11 did not experience any height reduction. This finding is consistent with that of a previous study, which reported that estrogen treatment was effective in four girls who started treatment at a mean age of 10.0 years old (mean final height: 174.3 cm) (12). In constitutionally tall girls, high dose estrogen treatment is most efficacious for height reduction in the youngest girls (18). In Marfan syndrome, puberty-associated growth peaks approximately 2.2 years earlier than it does in girls without Marfan syndrome (3). Given this phenomenon, it seems appropriate to start estrogen treatment before 11 years old in this population. However, since ethnic difference can be important in height growth, further studies are needed to draw a general conclusion about the age at starting estrogen.
Estradiol valerate was used for height control instead of ethinyl estradiol in this study. Introducing estradiol valerate in a stepwise fashion is also relatively physiologic because it induces secondary sexual characteristics without abruptly exposing the patient to high dose estrogen. Fortunately, there were no severe side effects observed in this study. There is no standard protocol for height control in girls with Marfan syndrome. However, given our results, a stepwise regimen of estradiol valerate may be an attractive option.
The exact mechanism of estrogen-mediated height control is not fully understood. However, there are two possible mechanisms by which estrogen limits linear growth. Estrogen suppresses somatomedin, thereby reducing the growth-promoting effects of growth hormone (19). Estrogen also increases the rate of skeletal maturation by acting directly on the epiphyseal cartilage (20).
This study has several advantages. For one, both the Marfan specific growth model and bone age were used for evaluation. The Marfan syndrome-specific growth curve is necessary to understand the growth patterns and to predict adult height in Marfan syndrome (21). Most prior groups used conventional height prediction models based on skeletal age (such as the Tanner Whitehouse and Bayley-Pinneau [91011]) to estimate adult height in girls with Marfan syndrome (9101112). However, because these models are based on growth data derived from normal children, their precision may be low in patients with growth abnormalities, such as those with Marfan syndrome (11). This study is also advantageous for its physiologic use of a stepwise regimen of estradiol valerate. In addition, this study presents a unique treatment regimen which was not previously reported.
However, this study has limitations. Marfan syndrome is not a common disease; therefore, we had only a small sample size of patients. Another limitation is that we did not include untreated girls as a control, and for comparison to the treated girls.
In conclusion, estrogen treatment via a stepwise regimen of estradiol valerate may offer effective height control in girls with Marfan syndrome. This regimen may be more efficacious when it is initiated in girls younger than 11 years old. In the future, large-scale research is warranted to substantiate these findings.


 XML Download
XML Download