

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Non-cardiac chest pain (NCCP) is angina or chest pain that is diagnosed as not occurring due to ischemic heart disease by a physician (1). Chest pain is a common reason for referral to pediatric cardiologists, and it impacts patients’ quality of life (12). In a previous study on cardiology consultations for pediatric patients, the clinical concerns included chest pain in 107 of 2,071 cases (5.2%), and the incidence of cardiac pathology within this patient group was low (11%) (3). Despite a low proportion of cardiac disease, patients with chest pain often have to endure the costly burden of cardiologic evaluation to rule out cardiac abnormalities.
In patients without cardiac disease, the esophagus is the most common cause of NCCP. Gastroesophageal reflux disease (GERD) is thought to be a major cause of NCCP in adults (45). Studies on adults with NCCP showed that nearly 25%–60% of patients with NCCP had abnormal findings on ambulatory pH monitoring (6). Additionally, Asian patients with NCCP showed a lower prevalence of GERD ranging from 41%–44.8% (57). The diagnosis of GERD often requires invasive methods, including a barium swallow, esophagogastroduodenoscopy (EGD), an ambulatory pH (with or without impedance monitoring), and a proton pump inhibitor (PPI) therapeutic trial. However, all diagnostic methods have limitations, and there is no gold standard for diagnosing GERD. The dilemma for clinicians is identifying which patient’s presentation may potentially point to GERD. Previous studies have suggested that typical reflux symptoms such as heartburn, postprandial pain, and regurgitation can be used to distinguish adult patients with GERD related-NCCP from patients with non-GERD related-NCCP (58). Since it is difficult to enforce invasive tests in children with chest pain, GERD evaluations of NCCP in children have not been fully explored. Most previous studies on chest pain in childhood have broadly reviewed causes, including musculoskeletal, respiratory, psychological, cardiac, traumatic, and gastrointestinal problems (2910). However, a steady increase in the prevalence of GERD during childhood has been recognized (11). In addition, some studies have found that there is a positive association between the duration of gastroesophageal reflux (GER) and the occurrence of complications such as Barrett’s esophagus and esophageal carcinoma (1213). These data demonstrate that the early detection of GERD in a pediatric population was required to prevent long-term sequelae of chronic esophagitis. Therefore, the purposes of this study were to clarify the clinical characteristics of erosive esophagitis (EE) in children with NCCP and to help clinicians diagnose and treat GERD earlier.
MATERIALS AND METHODS
Participants
We reviewed the records of outpatients aged 3–15 years who had a primary complaint of chest pain and were admitted to CHA Bundang Medical Center between January 2011 and December 2013. We identified and reached 123 potential patients with chest pain as the major diagnosis code. All patients were initially evaluated by a pediatric cardiologist. Among them, five patients (4%) had the following abnormal cardiovascular findings: arrhythmia, four; and mitral valve prolapsed with mitral valve regurgitation, one. The remaining 118 (96%) patients had NCCP. Of these 118 patients, 6% (n = 7) had been diagnosed with asthma and/or a chronic upper respiratory infection. The remaining 111 patients (94%) were referred to a gastroenterologist. Exclusion criteria were a gastric or duodenal ulcer, esophageal stenosis, esophageal varix, eosinophilic esophagitis, a Helicobacter pylori infection, a food allergy, a history of gastrointestinal surgery, and previous use of a PPI. Ultimately, 99 children who had undergone EGD with their parents’ consent were enrolled. The study protocol was approved by the institutional review board. Written informed consent was obtained from all patients or their caregiver(s) or legal guardian(s).
Questionnaires
The demographic and clinical characteristics were obtained from all the participating patients and their caregivers. All patients and/or their caregivers completed a detailed questionnaire about the characteristics of their chest pain (relationship to food intake, exercise, and sleep), the presence of possible symptoms of GERD (epigastric pain, heartburn, nausea, vomiting, and/or regurgitation), and associated gastrointestinal symptom such as diarrhea and constipation. They were asked to note a known family history of GER symptoms. To determine unfavorable dietary habits, all subjects provided detailed information about their dietary habits such as overeating; eating heavy foods; eating at night; consuming greasy food, salty, or spicy food; and drinking soda. More than one answer was applicable.
EGD
Enrolled patients underwent EGD. Patients with erosive esophagitis detected on EGD were classified as having EE-related NCCP. During EGD, the presence and grade of EE was categorized according to the Los Angeles classification.
Statistical analyses
Values are expressed as mean ± standard deviation. Statistical analysis was performed using an independent t-test or chi-square test as appropriate. Differences with a P value < 0.05 were considered statistically significant. Univariate and multivariate logistic regression models were used to identify the predictive symptoms of EE-related NCCP. Odds ratios (ORs) and their 95% confidence intervals (CIs) were estimated to measure the strength of the association between each covariate and EE-related NCCP. All statistical analyses were performed using SPSS, version 22 (IBM, Corp.).
RESULTS
The NCCP group included 49 girls and 50 boys. Subjects’ average age was 9.55 ± 2.95 years. The flow chart summarizes the classification of patients with EE-related NCCP (Fig. 1). Prevalence of EE was 35% (42/118). According to the LA classification system, LA-A in 69% (29/42), LA-B in 28% (12/42), and LA-C and D in 1 subjects. A comparison of the demographic and clinical characteristics of the EE- and non-EE-related chest pain groups is provided in Table 1. Patients in the EE-related NCCP group were significantly older than patients in the non-EE-related NCCP group (mean age: 10.9 ± 2.54 years vs. 8.52 ± 2.83 years, P < 0.001). The two groups did not differ significantly with regard to sex and the mean body mass index (BMI). Patients in the EE-related NCCP group had epigastric pain (P < 0.001); and nausea, vomiting, and/or regurgitation (P < 0.001) significantly more often than those in the non-EE-related group. Patients with EE-related NCCP significantly presented with unfavorable dietary habits (P = 0.01). A family history of GERD was also observed more frequently in patients with EE-related NCCP (P = 0.005).
Fig. 1
Flow chart of the study population. CP, chest pain; EE, erosive esophagitis; NCCP, non-cardiac chest pain.

Table 1
Patients’ demographics and clinical characteristics
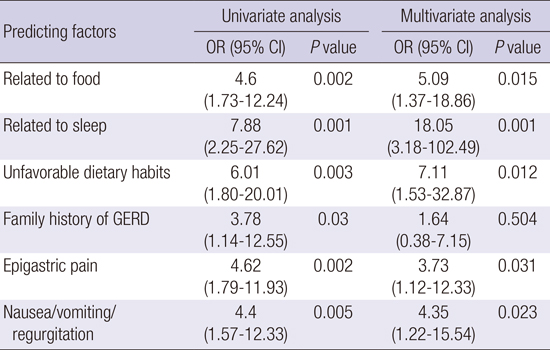
Characteristics of patients’ chest pain are shown in Fig. 2. Chest pain related to food or sleep was significantly more frequent in the EE-related NCCP group than in the non-EE-related group. Univariate logistic regression analysis identified the following as predictors for EE-related NCCP: chest pain related to food; chest pain related to sleep; unfavorable dietary habits; associated symptoms with epigastric pain; and nausea, vomiting, and/or regurgitation. Multivariate logistic regression analysis confirmed that chest pain related to sleep (OR = 18.05, 95% CI: 3.18–102.49); unfavorable dietary habits (OR = 7.11, 95% CI: 1.53–32.87); chest pain related to food (OR = 5.09, 95% CI: 1.37–18.86); associated symptoms of nausea, vomiting, and/or regurgitation (OR = 4.35, 95% CI: 1.22–15.54); and epigastric pain (OR = 3.73, 95% CI: 1.12–12.33) were predictive factors of EE-related NCCP (Table 2).
Fig. 2
Characteristics of patients’ chest pain. Chest pain related to food or sleep is significantly more frequent in the erosive esophagitis (EE)-related non-cardiac chest pain (NCCP) group (P < 0.05). However, chest pain related to exercise is not significantly different between groups.
Table 2
Predictors of erosive esophagitis (EE)-related non-cardiac chest pain (NCCP) according to univariate and multivariate logistic regression analyses
DISCUSSION
In several studies on the prevalence of GERD in older children and adolescents (age range, 13–20 years) in the United States, the prevalence of GER symptoms ranged between 18.8% and 56%, with Asians having the lowest prevalence, but this difference was not statistically significant (1415). As such, it has been reported a wide range of the prevalence about GERD in children. Diagnostic assessment of GER in pediatric population is restrictive, not only due to difficulty to enforce invasive tests in infants and children, but also because of lacking data in different age groups. In adults, various tools including combined pH-multichannel intraluminal impedance monitoring, symptom index, the symptom sensitivity index and symptom association probability have sensitivity for the detection of reflux events, only few data are available in children (161718). Moreover, few studies on the relationship between GERD and NCCP in young children have been published to our knowledge. Therefore, we attempted to estimate the prevalence of EE in children with NCCP. In addition, we attempted to investigate predictive factors for EE among them. Our study found that the prevalence of EE using EGD in children with NCCP was 35%, with no differences in sex. The prevalence of reflux symptoms during childhood after infancy may tend to increase with older age in childhood. In the present study sample, the mean age of EE-related NCCP was older than that of non-EE related NCCP (10.95 ± 2.54 years vs. 8.52 ± 2.83 years).
In the present study, we found no significant association between EE and an increasing BMI in children. In adult patients, several cross-sectional studies have proven that there is a positive relationship between obesity and the prevalence of GERD (1920). Knowledge on the association between obesity and GERD in children is scarce and controversial. Okimoto et al. (11) showed that a higher prevalence of GERD was closely associated with the BMI level in adults but not in patients aged < 20 years. Quitadamo et al. (21) proposed that central body fatness, measured by the waist circumference (WC), is also a risk factor for symptoms of GERD in children. Recent recommendations by experts demonstrated that WC may be more important than BMI as an index of abdominal obesity. In children with GERD symptoms, the evaluation of WC may be recommended in the near future.
In addition, an association between unfavorable dietary habits and EE in children was found in this study. It can be assumed that children who have unfavorable dietary habits, particularly foods with a high fat and energy rich content, have a greater risk of obesity as they age. Thus, if these unfavorable dietary habits continue into adulthood, obesity in adults may be a risk factor of GERD. In addition, Lee et al. reported that the dietary patterns of Korean children with GERD included overeating; eating heaving foods; eating at night; consuming greasy food, salty, and spicy food; and drinking soda (from 18.6–65.1%) (22). Such dietary habits (i.e., foods with high fat and salt content) are known to cause a decrease in the lower esophageal sphincter (LOS) pressure and an increase in the frequency of transient LOS relaxations, thereby increasing the risk of reflux disease (23). Furthermore, GERD symptoms and unfavorable dietary habits were significantly correlated to sleep disturbance, which impacts patients’ quality of life (24). The EE-related NCCP group had a significantly greater number of sleep-related reflux events compared to the non-ERD-related NCCP (8.8% vs. 35.7%). Sleep-related reflux has been associated with prolonged acid mucosal contact time, which increases the risk of esophagitis (25). These reports were well correlated with our finding that chest pain related to sleep and/or an unfavorable dietary habit is the most reliable predictor of EE in NCCP children.
In studies on adult patients with NCCP, the presence of typical reflux symptoms such as heartburn, regurgitation, postprandial chest pain, and the use of anti-reflux drugs for pain relief can imply a diagnosis of GERD (8). In our study, we found that a number of pediatric EE cases showed similar characteristics, except for heartburn, to NCCP in average aged patients. Since it is generally difficult for younger children to describe the symptom of heartburn, it cannot be a representative symptom of GER in children. Additionally, heartburn usually presents after prolonged regurgitation. This explains why there was no difference between groups regarding heartburn in the present study.
Several studies have suggested that genetic factors may be important in GERD, and GERD symptoms commonly cluster in families (262728). Genetic modeling for monozygotic twins confirmed the independent additive genetic effects of GERD (262930). Familial concordance of GERD symptoms may indicate genetic factors and shared environmental influences among family members such as food habits or lifestyle (27). It was not surprising that approximately 30% of children with EE in our study had a family history of reflux symptoms. This suggests the importance of checking for a family history when examining patients with NCCP. We propose that children with EE-related NCCP require more positive lifestyle modifications accompanied by family involvement instead of pharmacologic therapy to avoid the possible complications of GERD.
There are some important limitations to our study. First, the diagnosis of GERD was based on EGD findings without pH monitoring or esophageal manometry. Non-erosive esophageal reflux disease (NERD) could have been missed on EGD. Thus, our study had estimated the incidence of EE within this pediatric population. Second, the number of subjects in our study was relatively small. Future studies using representative samples of the pediatric population are needed to confirm these findings.
This study is important because few studies have reported on young patients with EE and NCCP. Our findings showed that children with chest pain in outpatient clinics had a low prevalence of cardiac abnormalities, and a considerable number of patients with NCCP in this pediatric population had GERD. Our findings proved that there were strong positive correlations with EE-related NCCP and an older age; a family history; unfavorable dietary habits; chest pain related to food; chest pain related to sleep; epigastric pain; and nausea, vomiting, and/or regurgitation in children. Therefore, our up-to-date findings provide the clinical characteristics of EE-related NCCP in children, and this may be useful information to primary clinicians. The early detection and proper treatment of EE in children can lead to fewer complications and an improved quality of life. Children with EE-related NCCP require pharmacological treatments and lifestyle modifications for their dietary habits.
In summary, we suggest that pediatric patients with chest pain should be adequately evaluated by pediatric gastroenterologists for GERD.
 XML Download
XML Download