

 PDF
PDF ePub
ePub Citation
Citation Print
Print




INTRODUCTION
Facial dyspigmentation is a frustrating disorder to patients, particularly in Asian countries (12). Topical agents inhibiting synthesis or transfer of melanin, as well as enhancing exfoliation of preexisting melanin pigment have been used as the first-line treatment (34567). Lasers and light-based devices working on pigment have been used with variable success (8). However, certain type of acquired facial hyperpigmentation shows different clinical features and unexpected responses to conventional treatment (9). Multiple laser treatments combined with topical whitening agent may not be effective, with clinical aggravation even after the multiple treatments (3).
Recently, we have experienced patients with distinctive bilateral or symmetric hyperpigmentation often extending to neck, which failed to respond conventional treatment for hyperpigmentation. To provide clarification, clinical characteristics, histopathological features, and other diagnostic examination as well as responses to treatments were evaluated in this study.
MATERIALS AND METHODS
Patients
We conducted a retrospective review of 31 patients with similar clinical findings who were seen from January 2012 to May 2014. All patients presented with unusual reticular hyperpigmentation on the face and neck. Patients professed no preceding erythema or itching before hyperpigmentation. Possible causes of associated conditions with abnormal skin hyperpigmentation, such as thyroid disease, hepatitis, and Addison’s disease, were excluded in all patients. We analyzed gender, age, histopathologic findings along with other laboratory findings when available. We also assessed for possible triggering factors.
Patch test
Standard thin-layer rapid use epicutaneous (TRUE Test®; Smart-Practice, Phoenix, AZ, USA) were conducted on 20 patients at the first visit. The patch tests were applied on the back for 2 days and interpreted according to International Contact Dermatitis Research Group scoring scale (ICDRG) guideline at 48 and 96 hours as described previously (10).
Skin biopsy
A 2-mm punch biopsy was performed on the very hyperpigmented lesion and peri-lesional normal skin, at least 3 cm apart from the lesion. Specimens were routinely processed by fixation in formaldehyde embedded in paraffin, sectioned and stained with haematoxylin-eosin and assessed with light microscopy. Immunohistochemical staining including HMB-45, S-100, and Melan-A were performed in both lesion and peri-lesional normal skin. Histopathologic findings were assessed by two skilled examiners and graded using a semi-quantitative score system: 0, none (normal); 1, minimal (equivocal); 2, mild; 3, moderate; 4, severe.
Statistical analyses
Statistical analyses were performed using SPSS Statistics for Windows, version 20.0 (IBM, Armonk, NY, USA). The mean scores of each histopathologic finding in two groups were compared with using t-test. And the χ2 test was used to analyze the qualitative differences between lesion and peri-lesional normal skin. Statistical significance was established at P < 0.05.
Ethics statement
This study was performed under institutional review board approval in Samsung Medical Center (2014-02-035). This was a retrospective chart review study, which waived informed consents regarding to this study. All medical records including medical photographs, patch test results, punch biopsy results, and treatment outcomes were reviewed by the institutional review board. All of the patients agreed publishing of the photographs of their face.
RESULTS
Patient demographics and clinical features
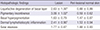
A total of 31 patients (3 males and 28 females) were enrolled in this analysis (Table 1). Age at presentation ranged from 24 to 77 years (mean 52.3 years, median 51 years). All patients presented with varying degrees of unusual brown to greyish mottled patches distributed over face and/or neck (Fig. 1). In 28 patients with facial dyspigmentation, both the lateral face and peri-oral area were more commonly affected (22/28, 78.6%) than the lateral face alone (2/28, 7.1%) or the peri-oral area alone (4/28, 14.3%). Three patients showed neck dyspigmentation without facial lesion, and 18 patients showed both facial and neck dyspigmentation.
Table 1
Clinical characteristics of the 31 patients

Fig. 1
Clinical photographs. Pigmentation was prominent on lateral face, perioral and neck. (A) M/51 Brownish mottled patch developed on face and neck 6 months ago. (B) F/55 Slate-greyish colored patch developed for 12 months on lateral face and neck. (C) F/33 Grey colored patch slowly developed over 5 years.

The average duration of the lesions was 2 to 120 months (mean 24.2 months, median 12 months). The patients were otherwise healthy and had no relevant medical history. No one had additional pigmentary changes on the trunk or extremities. There was no family history of similar pigmentary alteration. Twenty-two patients had received multiple laser treatments including intense pulsed light and low fluence Q-switched Nd:YAG laser before visiting our clinic. The treatments had all failed.
Patch test and laboratory findings
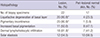
Patch test in 25 patients showed positive result in 17 (68.0%) and negative in 8 (32.0%) patients. The most common allergen was nickel sulfate (7 cases), followed by Fragrance mix (5 cases). Potassium dichromate was positive in 3 cases, and colophony in 2 cases, thiomerosal in 2 cases, and cobalt, dodecyl gallate, quanternium-15, and Carba mix in one case each (Table 2). All laboratory findings were within normal limit, except for one patient (case No. 22) with elevated immunoglobulin E (IgE).
Table 2
Frequency of detected allergens in patch test


Histopathology
The general histopathological features of lesional skin (22 cases) were compared with those of peri-lesional skin (17 cases). The major histopathological finding was basal layer degeneration and pigmentary incontinence, which was observed in all 22 lesional skin cases (Fig. 2). All lesional biopsy specimens showed various degrees of liquefactive basal cell degeneration, pigmentary incontinence, increased basal pigmentation, solar elastosis, and perivascular lymphohistiocytic infiltration in the upper dermis. No obvious spongiosis were observed. Only liquefactive change, pigmentary incontinence and dermal lymphohistiocytic inflammation was significantly increased in lesional skin compared with peri-lesional normal skin (Table 3). Distinctive (over grade 2+) liquefactive basal layer change was obvious in lesions of 20 cases (20/22, 90.9%), while it was noted in only 4 cases of peri-lesional normal skin (4/17, 23.53%) (P < 0.001) (Fig. 3). Distinctive pigmentary incontinence also more frequently observed in the lesions (20/22, 90.9%) than in peri-lesional normal skin (1/17, 5.9%) (P < 0.001). Lesional biopsy showed prominent dermal lymphohistiocytic infiltration in 18 specimens (81.8%) and solar elastosis in 12 cases (54.5%). However, there are no statistical differences compared with peri-lesional normal skin (Table 4).
Fig. 2
Histopathological evaluations of lesion and peri-lesional normal skin. Marked vacuolar degeneration of basal layer and melanin pigment deposition are found in lesional skin biopsy (A, B). (A) Haematoxylin and eosin staining × 200, (B) HMB45 immunostaining × 200.

Table 3
Comparison of histopathologic scores (mean ± SD) of biopsy specimens from patients
0, none (normal); 1, minimal (equivocal); 2, mild; 3, moderate; 4, severe.
Histopathologic findings of each group (Lesion vs. Peri-lesional normal skin) were compared using semi-quantitative score. Liquefactive degeneration, pigmentary incontinence, dermal lymphohistiocytic inflammations were significantly increased in lesion group in t-test.
*P < 0.001 compared with peri-lesional normal skin; †P < 0.05 compared with peri-lesional normal skin.
Fig. 3
Histologic evaluation of lesion (A) and perilesional normal skin (B). Distinctive (over grade 2+) liquefactive degeneration of basal layer is observed in lesion (A) compared with peri-lesional normal skin (B). (A, B) Haematoxylin and eosin staining × 200.

Table 4
Comparison of the number of biopsy specimens showing definitive histopathological change (over grade 2) in Lesion vs. Peri-lesional normal skin
The frequency of liquefactive degeneration, pigmentary incontinence, dermal lymphohistiocytic infiltrate were significantly increased in Lesion group compare to Peri-lesional normal skin (χ2 test).
*P < 0.001 compared with peri-lesional normal skin; †P < 0.05 compared with peri-lesional normal skin.
Follow-up and management
The mean follow-up period was 12.2 months in total 31 patients (range, 1 to 41.6 months). Among 31 patients, 19 patients who had been treated and followed-up over 6 months were analyzed for optimal treatment modalities and strategy.
Seven patients had only applied topical anti-inflammatory agents (topical tacrolimus 0.1% or pimecrolimus 1%) and used recommended moisturizers containing epidermal growth factor and ceramide as active ingredients. The moisturizers recommended to patients during treatment do not have any fragrance or paraben. Two of the 7 patients showed considerable improvement after continuous uses of topical anti-inflammatory agents with moisturizers (mean application period 4.2 months) and the rest 5 patients were satisfied with the treatment results of topical application and agreed to continue topical treatments (Fig. 4). The mean follow-up period of these 5 patients was 11.7 months.
Fig. 4
Clinical photographs (patient No. 14). This female, 45-year-old patient developed hyperpigmentation on lateral face and chin about 12 months ago. Moderate degree (grade 3) of basal layer liquefaction was evident in the biopsy specimen. Topical agent without laser therapy was used. Considerable improvement in pigmentation was noticed in the comparison before treatment (A) and 6 months later (B).

Twelve patients were first treated with topical agents with anti-inflammatory agents and moisturizers. After at least 3 months of topical treatments when hyperpigmentary lesion did not seem to extend, laser treatments were added for these patients. For the improvement of superficial pigmentation, fractional 1,927 nm laser (Fraxel Dual, Solta Medical, Heyward, CA, USA) was used first with the parameter of 5 to 10 mJ, coverage 35 to 40% (level 3–4), 4–8 passes). Low fluence QS Nd:YAG laser treatment (RevLite Cynosure Inc., Westford, MA, USA: 8 mm, 2.0 J/cm2, 10 Hz, 3 to 6 passes) was followed for the control of pigmentation in the dermis. Two to 4 times of fractional 1,927 nm laser treatments with or without 4–6 times of low fluence QS Nd:YAG laser treatment was performed on patients. The mean follow-up period in these patients was 21.3 months. Topical agent has been used for 5.5 months on the average (range, 3 to 10 months) before beginning laser therapy. All 12 patients showed clinical improvement and reported that they were very or extremely satisfied with the treatment (Fig. 5).
Fig. 5
Clinical photographs of patients 6 and 10. These patients were treated with topical tacrolimus 0.1% for 6 months due to vacuolar degeneration of basal layer at initial work-up. Laser treatment was subsequently added. (A, D) Before treatment in patient 6 and 10, respectively. (B, E) Six months after topical tacrolimus 0.1%, same respective order. (C, F) Eighteen months after treatment (topical tacrolimus 0.1% 6 months followed by laser for 12 months), same respective order.

DISCUSSION
All 31 patients presented with distinctive bilateral or symmetric bizarre hyperpigmentation of face and/or neck. Most of the patients were elderly with female preponderance, along with chronic or refractory course of disease (mean duration; over 2 years). Pigmentation generally manifested as brown to slate-grey color with ill-defined margin. The lateral face (forehead and both cheeks) was uniquely involved and hyperpigmentation affected both sun-exposed and non-exposed area in neck. Perioral accentuation of pigmentation was another noticeable finding.
All enrolled patients were initially diagnosed as melasma at other clinics and most underwent multiple laser treatments before visiting our clinic. Melasma is usually pronounced in mid face, as a malar prominence or peri-ocular in middle aged women (6). Also it is associated with pregnancy, ultraviolet exposure, oral contraceptives and endocrine dysfunctions (11), which were not found in our patients. Histopathologically, melasma shows increased epidermal melanin, rather than dermal melanin (12). Distinctive liquefactive degeneration of basal laser is not a common finding in the lesion of melasma. These clinical and histopathological findings of our patients suggest a disease entity other than melasma.
Lichen planus pigmentosus (LPP) or Ashy dermatosis (AD: erythema dyschromicum perstans) should be taken into account for this clinical condition. LPP and AD commonly presented as ill-defined oval, greyish brown pigmentation on the face and neck or trunk and limbs without an inflammatory phase. Clinical manifestation of our patients was different from LPP and AD. No patients showed any truncal involvement. Lichenoid lympho-histiocytic infiltration or colloidal body in the epidermis was not prominent in the histopathological examination, which is the characteristic feature of two similar pigmentary disorders of LPP and AD (13).
The vacuolar change of basal layer without spongiosis accompanying dermal melanin deposition, implies the possibility of similar underlying pathomechanism as seen in pigmented contact dermatitis (PCD), also known as Riehl’s melanosis (14). PCD is a rare variant of non-eczematous contact dermatitis, which is believed to be caused by repetitive contacts with very small amounts of allergens, such as washing powder, fragrance or cosmetics (1516). The small amount of allergen induces spongiosis in epidermis, rather than the classical symptoms of contact dermatitis that include erythema, edema and vesicle formation. On the contrary, as subclinical damage persists, vacuolar change of basal layer results in pigmentary incontinence. Clinically, melanin pigment in upper dermis is so slowly absorbed that the hyperpigmentation appears to persist or worsen over time if consistent contact of possible allergens happens (17). Riehl’s melanosis, first described by Riehl as “war melanosis” in 1917, similarly affects the face, and is related with nutritional factors and sensitizing chemicals in cosmetics (181920). Riehl’s melanosis is considered synonymous with PCD, with the common allergen being fragrances and chemicals in cosmetics (19). Clinical and histological manifestation of our patients looked similar to that of PCD. Presently, 19 patients were presumed to involve personnel causative allergens including hair dyes (63.2%, 12/19 cases) and cosmetics (36.8%, 7/19 cases); however, no patient showed positive in the “as is” test with suspected product. Some patients (17 out of 25 patients) demonstrated positive result in T.R.U.E test, but their clinical relevance is doubtful due to lack of prolonged use of personnel cosmetics or fragrances based on their personal history. None of patients recalled any preceding erythema or itching which can be a possible sign of contact dermatitis. We did not perform photopatch test on these patients. For patients who presented with skin lesion especially on sun exposed area, photopatch test can be helpful for the exact diagnosis (21). However, patients in this analysis did not show definite photo-related skin lesion. Photos from Fig. 1 demonstrated prominent pigmentary disturbance on perioral and lateral face rather than on the central area. The central neck area especially right under the chin is usually spared in photo-related disease unlike our patients who showed whole neck involvement of skin lesion. Laboratory tests, such as IgE or eosinophil cationic protein (ECP), which reflect allergic tendency, were not increased except one patient (22). The histological findings of our patients, which included basal layer disruption without spongiosis, suggest underlying subclinical inflammatory process as seen in PCD, which are not preceded by an obvious inflammatory injury. Therefore, the most plausible diagnosis would be PCD in our patients, although there was no definite relation of causative allergens with skin lesion found through all examination.
Considering that most of our patients had tried repetitive laser treatments, it is possible that basal layer disruption is caused by unknown inflammatory causes as well as subclinical wounding incurred during laser treatments. The clinical course in which dyspigmentation worsens in many patients after the application of multiple laser treatments supports the possibility that repetitive laser treatments might play a role in disease progression. This hypothesis needs more study.
The bizarre pigmentation in our patients was primarily due to dermal melanin deposition, mainly in dermal melanophages. Melanophages are primarily the result of cutaneous inflammatory process that affects the dermo-epidermal interface leading to deposition of pigment within dermis (23). Thus, the control of cutaneous inflammatory process should be prioritized in this condition, especially before laser treatment, which can cause superimposed subclinical inflammation, leading to secondary hyperpigmentation or pigmentary worsening. The triggering factors of inflammation are usually deducted by knowledge of a patient’s history and location of inflammation. But, for some diseases like PCD, which feature barely distinguishable inflammation, thorough history-taking and patch test should be done to identify any possible causative allergen. Histologic evaluation of pigmented lesion (skin biopsy) provides a diagnostic clue and valuable information of depth of pigment location and distribution as well as dermal nature which requires for optimal treatments. Punch biopsy of pigmentary lesion (2 to 3 mm) is sufficient with minimal risk of scarring. Concurrent evaluation of peri-lesional normal skin can provide better precise information in interpreting pathologic change of dyspigmentation (12). However, facial hyperpigmentation of women, especially middle aged Asians, are frequently considered as melasma, whether it is or not. Sometimes, active laser therapy is tried based on this tentative diagnosis without suspicion of other disorders. However, this approach is unsatisfactory as there are many pigmentary disorders that clinically mimic melasma and the distinction between them invariably requires astute histopathological evaluation and subsequent clinical correlation (3).
When it comes to the optimal treatment modalities in these patients, laser therapy for hyperpigmentation should not be the first choice if there is a severe basal layer disruption and solar elastosis. Presence of liquefactive degeneration of basal layer and dense inflammatory cell infiltration in dermis suggests accumulative inflammatory damage (16), therefore topical agents of anti-inflammatory activity, not depigmenting or whitening agents should be used first. According to this well-defined step-by-step approach, among 12 patients who suffered with refractory, long-lasting dyspigmentation was considerably improved (Figs. 4 and 5). This approach is summarized in Fig. 6. Two of 7 patients who used only topical anti-inflammatory agents and moisturizers achieved excellent clinical improvement.
Fig. 6
Step-by-step approach for refractory facial hyperpigmentation. In step 1, underlying allergic tendency is checked by with thorough history-taking and/or blood work. In step 2, the degree of inflammation and resiliency of dermis are determined. In step 3, the topical agent is used to reduce inflammation for at least several months. In step 4, possible adequate methods for removal of remnant pigments are considered.

The histopathologic findings and the prolonged course of the hyperpigmentation in our cases were both suggestive of a preceding causative subclinical inflammatory process. The underlying cause remains uncertain and multiple factors may have produced this clinical feature. When approaching to this long-lasting or refractory facial dyspigmentation, clinicians should consider a step-by step approach. Step 1 involves checking the underlying allergic tendency with thorough history taking and/or blood lab. Step 2 involves determining the degree of inflammation and resiliency of dermis whether it could be properly restored after laser treatments. Step 3 is the application of a topical agent capable of reducing inflammation for at least months. Step 4 should consider possible adequate methods for removal of remnant pigments as the last step of treatment.
We present 31 patients with peculiar clinical feature and long-lasting course hyperpigmentation on the face and neck. The use of a systematic step-by-step approach with appropriate therapeutic modality can provide clinical benefit.
 XML Download
XML Download