

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Fever occurs in approximately half of all patients admitted to the intensive care unit (ICU) (1). The significance of fever varies in different clinical settings. Fever may arise as an adaptive response to infectious causes (2) or as a nonspecific finding along with a critical illness or inflammatory condition (3). An elevated body temperature within physiologically febrile range in infectious conditions has been shown to enhance host immune cell activity against pathogen (45) and confer a survival benefit in a number of animal models and in human data (67). However, fever may be a mediator of worsened clinical outcome in critically ill patients, and high or persistent fever has been associated with increased mortality (8910).
Among mechanically ventilated patients, fever could have a detrimental effect on gas exchange, and increases in cardiac output and oxygen consumption driven by fever tend to worsen hypoxemia (1112). Moreover, increased production of carbon dioxide may deteriorate minute ventilation requirements, resulting in failure to wean from mechanical ventilation (MV). Fever had been reported to worsen lung tissue injury by enhancing recruitment of neutrophils and oxygen toxicity in mechanically ventilated patients (1314), and exacerbate ventilator-induced lung injury (15). Taken together, cumulative data suggest that fever may have negative impacts on MV outcome, resulting in unfavorable consequences in critically ill patients. However, ventilator-associated infection complication (1617) accompanied by fever could be associated with increased ICU length of stay and mortality (1819). These findings urge us to investigate whether there is an independent association of fever and length of MV in mechanically ventilated patients.
Recently, in a cohort study of mainly septic patients with acute lung injury, fever was found to be associated with a prolonged duration of MV (20). However, another study on patients with acute respiratory distress syndrome reported contradictory results that fever in early phase may be an important factor in determining favorable outcome (21). Thus, the aim of our present study was to evaluate the association of body temperature with MV duration in a heterogenous cohort of mechanically ventilated patients.
MATERIALS AND METHODS
Study design and patients
The study population comprised consecutively enrolled patients in a previous prospective, multicenter observational study in Korea and Japan designed to evaluate the association of fever and the use of antipyretic therapy with mortality in critically ill patients with and without infection (22). That study included patients admitted to ICU for more than 48 hours from 1 September 2009 to 30 November 2009, and excluded cases with post-cardiac arrest or acute brain injury.
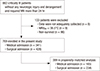
This study was focused on the impact of body temperature on duration of MV in patients admitted to the ICU. The enrolled subjects were 882 critically ill patients who required MV for more than 24 hours from 10 Korean and 15 Japanese ICUs. To determine the degree of body temperature changes during MV, we defined maximum body temperature (MAXMV) as the highest body temperature measured at any time under the support of MV. We firstly enrolled survived patients within 28 days after ICU admission and calculated total mechanical ventilation time (TVT) as the time from MV initiation up to 28 days after enrollment. As the effect of fever on TVT could be skewed by early deaths within 28 days, we enrolled survived patients within 28 days after ICU admission. We excluded those with MAXMV < 36.5°C, and those for whom data about MV were incomplete (Fig. 1). Mechanical ventilator-free day (VFD) was also compared depending on the presence of fever in all enrolled subjects including non-survivors.
Data collection
We recorded variables including age, gender, reason for ICU admission, duration of TVT, and the Acute Physiology and Chronic Health Evaluation II (APACHE II) scores. The category of ICU admission was classified as medical or surgical admission. The major reason of admission was categorized as cardiac or vascular disease, thoracic or respiratory disease, renal or metabolic disease, gastrointestinal tract disease, and other. We recorded four-hourly body temperature readings until either ICU discharge or 28 days after ICU admission. The measurement of body temperature was performed as previously described (22).
Statistical analysis
Descriptive statistics included means ± standard deviations for continuous variables and frequencies and percentages for categorical variables. Results were compared with t-test or Mann-Whitney U-test and the χ2 test or Fisher’s exact test as appropriate.
To evaluate whether high body temperature resulted in prolonged TVT, we compared TVT between patients with a MAXMV of 36.5°C to 37.4°C and those with a MAXMV ≥ 37.5°C in each of medical and surgical admission. Propensity scores for each subject were generated using logistic regression analysis model to compute the probability of MAXMV ≥ 37.5°C, compared to MAXMV of 36.5°C to 37.4°C, based on the following 10 clinically relevant covariates: gender, age, APACHE II score, height, weight, history of traumas, transplantation, readmission, sepsis within 24 hours of ICU admission, and reason for admission. Propensity score matching was performed by Greedy matching with using a caliper of 0.2 standard deviations of the logit of the propensity score. The selected patients formed well-matched 1:2 pairs in medical admission and 1:1 pair in surgical admission (patients with a MAXMV of 36.5°C to 37.4°C and those with a MAXMV ≥ 37.5°C). In the propensity score matched cohort, TVT between patients with a MAXMV ≥ 37.5°C and those with a MAXMV of 36.5°C to 37.4°C was compared with Wilcoxon signed rank test or linear mixed model that accounted for the clustering of matching 1:2 pairs.
We hypothesized that high body temperature could be related to prolonged TVT. As the relationship between body temperature and TVT may not be linear, we treated body temperature as a categorical variable, and MAXMV was analyzed in four range categories of 36.5°C to 37.4°C, 37.5°C to 38.4°C, 38.5°C to 39.4°C, and ≥ 39.5°C. Univariate and multivariate linear regression analyses were performed to examine how the severity of MAXMV affects TVT in each of medical and surgical admission. We selected significant variables using a stepwise backward elimination procedure in multivariate models. The TVT was subjected to logarithmic transformation to achieve a normal distribution before being entered into the linear regression model.
To verify the impact of fever on TVT, we additionally analyzed the association of MAXMV and VFD through multivariate analysis in all enrolled subjects including non-survivors. However, the distribution of VFD made it difficult to apply standard linear regression model, showing the high frequency of extreme outcome ( Supplementary Fig. 1). Quantile regression approach was fitted to better explain the effect of MAXMV on VFD. We performed quantile regression analysis at 0.25 quantile and median for medical admission and at 0.1 and 0.25 quantile for surgical admission. The goodness-of-fit of the model was assessed as the pseudo R2
. Variables were selected by backward elimination and standard errors for regression coefficients were obtained with the bootstrap method. All tests were two-sided, and a P value < 0.05 was considered significant. Data were analyzed using SPSS version 20.0 for Windows (SPSS Inc., Chicago, IL, USA) and SAS version 9.3 (SAS Institute, Cary, NC, USA).
Ethics statement
Data collection and data analysis for this study were approved by each of the local institutional ethics committees, and the institutional review board of Asan Medical Center approved this study (IRB No. 2009-0416). The requirement for informed consent was waived at each individual participating center.
RESULTS
Baseline characteristics of survived subjects with MV
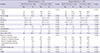
A total of 769 patients were firstly included in our present analysis (Fig. 1). The demographic and clinical characteristics of the unmatched survived patients in each of medical and surgical admission are listed in Table 1. A MAXMV ≥ 37.5°C was recorded in 283 (83.0%) patients among the 341 with medical admission, and in 301 (70.3%) among the 428 with surgical admission. Among patients with both categories of ICU admission, men were less frequently observed and the mean APACHE II score was higher in those with a MAXMV ≥ 37.5°C than in those with a MAXMV of 36.5°C to 37.4°C. There were no significant differences in other clinical variables between the patients with a MAXMV ≥ 37.5°C and a MAXMV of 36.5°C to 37.4°C in medical admission. In surgical admission cases, patients with a MAXMV ≥ 37.5°C were older, tended to be from Japan, and were more likely to be associated with sepsis in the first day of ICU admission, compared to those with MAXMV of 36.5°C to 37.4°C.
Table 1
Baseline characteristics in the unmatched, survived subjects
Baseline characteristics after propensity matching
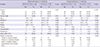
After propensity matching, 94.8% of patients with a MAXMV of 36.5°C to 37.4°C (n = 55) in medical admission were successfully matched 1:2 of patients with a MAXMV ≥ 37.5°C. In patients with surgical admission, suitable propensity 1:1 matching was found for 117 (92.1%) of the 127 patients with a MAXMV of 36.5°C to 37.4°C. Propensity matching successfully eliminated discordance that existed between the two temperature groups in this study (Table 2). As the only remaining unbalanced covariate was nationality, we performed additional propensity matching in survived subjects using all covariates including nationality (Supplementary Table 1).
Table 2
Baseline characteristics in the propensity-matched, survived subjects
Association of MAXMV with TVT
In Table 3, the TVT was separately assessed in medical and surgical admission according to the MAXMV value. In crude analysis, patients with a MAXMV ≥ 37.5°C had a significantly longer TVT irrespective of the category of ICU admission, compared to those with a MAXMV of 36.5°C to 37.4°C. After propensity matching, we found that the mean TVT of patients with a MAXMV ≥ 37.5°C was also significantly associated with a prolonged TVT by 5.4 days in medical admission and by 1.2 days in surgical admission compared to those with a MAXMV of 36.5°C to 37.4°C. We also performed propensity matching process using all covariates including nationality and obtained similar results, and patients with MAXMV ≥ 37.5°C was proven again to be significantly related to prolonged TVT (Table 3).
Table 3
Comparison of total mechanical ventilation time according to the MAXMV value in survived subjects
Independent predictors of TVT
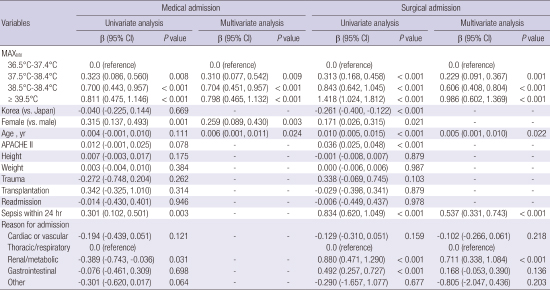
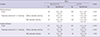
Univariate and multivariate predictors of prolonged TVT in the enrolled survived subjects are listed in Table 4. In univariate analysis, we obtained the mean estimated TVT by taking the antilog of the linear regression coefficient for the MAXMV. As body temperature was stratified by four categories according to the MAXMV values (36.5°C to 37.4°C, 37.5°C to 38.4°C, 38.5°C to 39.4°C, and ≥ 39.5°C), the mean estimated TVT in medical admission was 4.8, 6.6, 9.6, and 10.7 days, respectively. For the patients with surgical admission, we obtained values of 1.9, 2.7, 4.5, and 8.0 days, respectively, for the four categories of MAXMV.
Table 4
Univariate and multivariate models for total mechanical ventilation time in survived subjects

Multivariate analysis for predicting factors related to prolonged duration of TVT was performed, adjusting marginal and significant variables in univariate analysis. For the patients with medical admission, patients with fever within three categories of MAXMV of 37.5°C to 38.4°C, 38.5°C to 39.4°C, and ≥ 39.5°C sustained a significantly prolonged duration of TVT than those with MAXMV of 36.5°C to 37.4°C (β = 0.310, 0.704, 0.798, and P value = 0.009, < 0.001, < 0.001, respectively). Female gender (β = 0.259, P value = 0.003) and age (β = 0.006, P value = 0.024) were significantly associated with a longer TVT in medical admission. For patients with surgical admission, all three categories of fever (MAXMV of 37.5°C to 38.4°C, 38.5°C to 39.4°C, and ≥ 39.5°C) were also a significant predictor of increased TVT, compared to a normal MAXMV range (β = 0.229, 0.606, 0.986, and P value = 0.001, < 0.001, < 0.001, respectively). Older age (β = 0.005, P value = 0.022), the presence of sepsis developed within the first day of ICU admission (β = 0.537, P value < 0.001) and renal/metabolic causes (β = 0.711, P value < 0.001) taking thoracic/respiratory causes as a reference were significantly associated with longer TVT in surgical admission.
Association of MAXMV with VFD in all enrolled subjects
To clarify the impact of fever on TVT, we observed the relationship between MAXMV and VFD in all enrolled subjects with non-survivors. Propensity score matching was performed in all subjects using all covariates including nationality (Supplementary Table 2). In propensity-matched analysis, we found that patients with a MAXMV ≥ 37.5°C had significant shorter duration of VFD in both category of ICU admission, compared to those with a normal range of MAXMV (Supplementary Table 3).
Table 5 shows the estimated coefficients of clinical variables from multivariate quantile regression analysis at percentiles of 0.1, 0.25 and 0.5 considering the distribution of VFD in all enrolled subjects including non-survivors (Supplementary Fig. 1). The effect of MAXMV on VFD was significant at the twenty-fifth and fiftieth percentile in patients with medical admission. When all other covariates were controlled at the fiftieth percentile, patients with all three categories of fever (MAXMV of 37.5°C to 38.4°C, 38.5°C to 39.4°C, and ≥ 39.5°C) in medical admission had significantly decreased VFD than those with normal range of MAXMV, by 2.7 days, 8.3 days and 14.0 days, respectively (The model fit statistics Pseudo R2 was 0.131). In patients with surgical admission, higher range of MAXMV (38.5°C to 39.4°C, and ≥ 39.5°C) had a significant effect on decreased VFD at the twenty-fifth percentile relative to the reference range of 36.5°C to 37.4°C. In controlled condition of other covariates, patients with fever (MAXMV of 38.5°C to 39.4°C, and ≥ 39.5°C) in surgical admission had significantly decreased VFD than those with normal MAXMV range, by 4.0 days and 9.4 days at median quantile regression of VFD, respectively (Pseudo R2 = 0.196).
Table 5
Multivariate quantile regression analysis for patient variables at the quantiles of mechanical ventilator-free days in all enrolled subjects

The results shown are the obtained regression coefficients (β) with corresponding P values, which could be used to predict mechanical ventilator-free days at the distinct level of MAXMV. Variables including height, weight, post-transplantation and readmission that showed no statistically significance in the multivariate quantile regression analysis were not indicated.
MAXMV = maximum body temperature during mechanical ventilation, APACHE II = acute physiology and chronic health evaluation II, SE = bootstrapping standard error of regression coefficient in the multivariate quantile regression analysis.
DISCUSSION
This study showed that fever contributed to prolong TVT in our subjects regardless of ICU category. Fever was an independent predictor of prolonged duration of MV in two groups of survivors of both medical and surgical admission. In addition, fever was negatively associated with ventilator-free days in all enrolled subjects with non-survivors. These results suggest that fever should be considered a potential confounding factor on MV outcome to design future studies on the outcome of mechanically ventilated patients.
Similar to our present study, Netzer et al. (20) conducted a prospective cohort study on mechanically ventilated patients with acute lung injury. These authors demonstrated that an additional febrile day during the first week after acute lung injury was strongly related to delayed weaning from MV, but more than two thirds of the enrolled cases were related to sepsis. The strength of our investigation is that we confirmed the significant association of fever with prolonged TVT in heterogenous ventilated patients with diverse underlying conditions, almost unrelated to sepsis. We used propensity score matching to assess this issue in each category of ICU admission, as the type of ICU admission could influence the outcome. In addition, we demonstrated that the degree of body temperature in mechanically ventilated patients was significantly associated with a prolonged TVT. These are the main features of this study that deserve to be highlighted as they differentiate it from the study by Netzer et al. (20).
Moreover, to verify these findings, fever during MV was found to be related to worse MV outcome by decreasing VFD in mechanically ventilated patients even including non-survivors. Interestingly, the association of reduced VFD with fever was slightly clearer for ICU patients with surgical admission, showing higher pseudo R2, than those with medical admission. This finding might be related to the difference in the presence of sepsis in the first day of ICU stay between both categories of ICU admission. About three quarters of medical admission had sepsis at admission to the ICU, but only 10% of those with surgical admission were without sepsis. Recent studies have suggested fever may have different clinical implications for ICU patients with and without sepsis (222324). Lee et al. (22) showed that fever was associated with increased 28-day mortality in patients without sepsis but not in those with sepsis. Similar findings were observed in retrospective cohort study of Young et al. (23). High peak temperature in ICU patients without infection was associated with an increased risk of in-hospital mortality. These findings raised possibility that the presence of sepsis or infection may be an important determinant of ICU outcome. Although further studies on the impact of fever on MV outcome should be needed, it is important that our results confirmed significant association between fever and worse MV outcome including VFD regardless of ICU category.
As prolonged MV can lead to various potentially serious complications (25), reducing the time that ICU patients receive MV is crucial. However, to the best of our knowledge, no previous clinical trial has shown whether fever control could shorten the TVT and improve MV outcome. In a randomized trial, Bernard et al. (26) evaluated the effect of intravenous ibuprofen in 455 patients with severe sepsis. Reducing temperature in patients receiving MV resulted in decreases in heart rate and minute ventilation, although no survival benefit was seen. Moreover, antipyretic therapy using propacetamol reduced the energy expenditure index and oxygen consumption in a small study of mechanically ventilated patients with infection (11). A previous randomized trial also showed that patients receiving external cooling were more likely to have shock reversal and achieve hemodynamic stability, reducing the vasopressor dose by 50% in mechanically ventilated patients with septic shock, compared to control group (12). These results suggest that fever control may have beneficial impacts on MV outcome. A recent study of Young et al. (27) demonstrated that early use of acetamino-phen in critically ill patients with known or suspected infection did not show a benefit in terms of primary outcome; however, the length of ICU stay was reduced among survivors, in line with our results. However, the impact of fever control on MV outcome should be further elucidated in randomized trials on mechanically ventilated ICU patients.
Several limitations should be considered, because our analysis was conducted using data from a previous observational study (22). Although we found a significant relationship between fever and prolonged duration of MV, casual link cannot be assumed. Moreover, there was no standardization for protocols of weaning from MV contributing data to our analysis. Other potential factors also could affect the MV outcomes. Sepsis in the ICU setting is commonly accompanied with fever (28), which might increase the risk of organ dysfunction and critical illness polyneuropathy resulting in delayed weaning from MV (29). This pathologic condition could be the underlying cause of both MV duration and fever. Moreover, characteristics of fever including timing and duration of fever may also affect TVT and MV outcome (30). Interestingly, prolonged duration of MV has been also described for an independent risk factor for prolonged or long-lasting fever (10), which may explained in light of the high incidence of ventilator associated pneumonia (VAP). Previous literature reported that fever (≥ 38.0°C) in patients with VAP could persist for at least three days in more than one third of them (31), and the mean time to resolution of fever has been reported about 6 days (32). Thus, in evaluating the possible association of fever with MV outcome, the results should be interpreted with caution regarding the presence of VAP, which in turn, might prolong the need for MV. Meanwhile, body temperature measured in the present study could be influenced by various factors. More than half of ICU patients were treated with antipyretic therapy without specific protocols for treatment of fever across the participating ICUs. Additionally, about ten percent of enrolled ICU patients received lifesaving therapeutic modality including extracorporeal membrane oxygenation and renal-replacement therapy. These patients are more likely to experience heat loss through the extensive extracorporeal circuit, resulting in hypothermia (3334). We only measured MAXMV defined as maximal body temperature during MV, and did not cover if febrile-range MAXMV was related to development of VAP in the current investigation. Thus, further research by using etiology and characteristics of fever needs to be conducted to elucidate the impact of fever on MV outcome.
Our current observations indicate that febrile patients with respiratory failure may have a significantly prolonged TVT compared to those with body temperatures within the normal range, regardless of ICU category. We also demonstrate that fever in mechanically ventilated patients is an independent risk factor for prolonged TVT, highlighting the importance of fever on MV outcome. Thus, fever in critically ill patients with MV appears to be significantly associated with worse MV outcome. Clinical implication of our results is that fever under the support of MV should be considered to design future researches on outcome of mechanically ventilated patients.
 XML Download
XML Download