

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Postoperative dysphagia, which is usually temporary, is the most common complication after anterior cervical spine surgery, and incidence is 1%–79%, depending on the study design (12345678). On-going studies are being conducted to devise methods to reduce postoperative dysphagia, such as use of methylprednisolone, pressure control of endotracheal tube cuff, and metal bar selection. Nevertheless, their efficacy has not been established.
We performed a retrospective study previously to evaluate risk factors for dysphagia in patients who underwent anterior cervical spine surgery (6). As results, anterior cervical discectomy and fusion (ACDF), multi-level surgery, and surgery at a higher cervical level increased the risk for dysphagia. Moreover, patients who underwent multi-level surgery revealed thicker anterior soft tissue when measured within 48 hours after surgery. Hence, we hypothesized that prevertebral soft tissue thickness could be a cause of dysphagia after anterior cervical spine surgery.
However, our previous study was retrospective, and the risk for dysphagia was measured only using simple X-rays, and not with videofluoroscopic swallowing studies (VFSS). Therefore, we could not assess problems associated with each swallowing phase in the patients.
Herein, we performed a prospective study to assess the temporal, spatial, and kinematic indices associated with swallowing using pre and postoperative VFSS to verify the effects of ACDF on swallowing ability, and evaluate the factors associated with swallowing dysfunction after surgery.
MATERIALS AND METHODS
Subjects
Patients who underwent ACDF at our hospital were enrolled between July 2010 and June 2011. The exclusion criteria were: 1) dysphagia symptoms before surgery, 2) disorders of the central nervous system, such as stroke or traumatic brain injury, 3) previous neck surgery, 4) magnetic resonance imaging or radiographs were unavailable, and 5) refused participation in the survey.
Twenty (eight men and 12 women; mean age, 49.45 years) of 80 patients who underwent ACDF were recruited. Summary of surgical procedures concerned in the risk of dysphagia was 1) we made a horizontal skin incision about 2 inches at the target levels confirmed with intraoperative radiographic exams with C-arm, 2) we did not cut the platysma muscle horizontally but opened it vertically by a blunt manner, 3) the prevertebral fascia was dissected and opened in an extent as small as possible just for the discectomy and fixation, 4) we used the Atlantis plate (Medtronic, Memphis, TN, USA) for cervical fixation, which thickness is 2.5 mm, and 5) the complex of soft tissues and nerves of anterior neck was dealt with great care because injuries to the structures can cause dysphagia. In order to reduce the injuries to the structures, we tried to restrict the extent of dissection for the prevertebral fascia as small as possible according to the surgical need, not only longitudinally, but also laterally. The highest surgical level varied from C3 to C6. The C5 level had the most (n = 10) patients. The single level and multi-level groups had 10 patients each (Table 1).

VFSS
VFSSs were performed 1 day before surgery and within 1 week after surgery. The protocol from Logemann’s study was modified and used (9). Patients were given 5 mL diluted barium once to minimize radiation exposure. Labial closure, tongue movement, seal-off of the lateral sulcus, and posterior propelling of the bolus were analyzed during the oral phase. Swallowing reflex, closure of the velopharyngeal port, pharyngeal peristasis, laryngeal elevation, and closure were analyzed during the pharyngeal phase. Cricopharyngeal dysfunction was assessed during the esophageal phase, and the Penetration-Aspiration Scale was used to evaluate aspiration. We also evaluated the residue at the valleculae fossa and pyriform sinus. We measured time parameters, such as oral transit time (OTT), pharyngeal delay time (PDT), pharyngeal response time (PRT), and pharyngeal transit time (PTT). OTT is defined as the time elapsed since the bolus move backward until the head of the bolus reach to lower edge of mandibular lamus. PDT is defined as the time elapsed since oral transit time ends until laryngeal elevation begins. PRT is measured from end of pharyngeal delay time until the tail of bolus passes through the cricopharyngeal region, and PTT is defined as add PDT to PRT.
Significant residue in the valleculae or pyriform sinus (grade 2, > 10%), or overt penetration or aspiration (Penetration-Aspiration Scale score > 2) were defined as abnormal VFSS findings.
We traced movement of the hyoid bone using the Image J program. The baseline point was the anterior-inferior border of fourth cervical vertebral body, and the y-axis was created from a straight line between the anterior–inferior points of C4 and C2 (Fig. 1A). The x-axis was a perpendicular line from the anterior and inferior point of C4. We marked anterior displacement of the hyoid bone on the x-axis, superior displacement of the hyoid bone on the y-axis, and measured from where the hyoid bone starts until it returned (1011).
Fig. 1
Videofluoroscopic swallowing study (VFSS) measurements. (A) Prevertebral soft tissue thickness was measured from the anterior aspect of the cervical vertebra to the barium line inside the esophagus. The red lines are distance from each cervical vertebra to this barium line. (B) Hyoid bone displacement was measured from VFSS images, which were processed using the Image J program. The y-axis was created from a straight line between the anterior–inferior points of C4 and C2, and the x-axis was created as a perpendicular line from the anterior and inferior point of C4 (red long arrows). The position of the hyoid (red dot, indicated by the yellow arrow) was calculated as X and Y coordinates. (C) The opening of the upper esophageal sphincter was measured serially frame by frame, and the measurement point was 1.5 cm below the lower hypopharynx (indicated by yellow arrow).
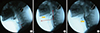
The upper esophageal sphincter (UES) measuring point was 1.5 cm below the lower end of hypopharynx (Fig. 1B). The UES opening distance during swallowing was measured as the length of the food passing through this point. Time to the widest opening of the UES and duration of UES opening were analyzed (12).
Thickness of prevertebral soft tissue was measured during resting phase of swallowing, from the anterior aspect of the cervical vertebra to the barium line inside the esophagus (Fig. 1C), which allowed us to exclude the anterior aspect of the esophagus and pharynx.
Dysphagia survey
We conducted a one-on-one survey to identify dysphagia severity using the dysphagia score at that time of VFSS. A telephone survey was conducted 1 month after surgery to characterize patients who had more than moderate dysphagia symptoms. Dysphagia survey was performed using dysphagia scoring system defined by Bazaz et al. (13), and this system is about subjective presence of dysphagia in solid and liquid food. The grading is “none (no presence of symptom),” “mild (rare presence of symptom in solid food),” “moderate (no symptom in liquid food whereas occasional symptom on solid food),” and “severe (symptom in liquid and most of the solid food)”.
Statistical analysis
We compared the kinematic and spatial indices before and after surgery using the Wilcoxon signed-rank test. The χ2 test was used to analyze the risk of dysphagia using factors related to the number of surgical levels and the highest surgical level. The Mann-Whitney test was used to verify changes in the swallowing parameters during the VFSS. A P value < 0.05 was considered significant.
RESULTS
Patients grouped by VFSS results and dysphagia symptoms
Eight patients showed normal postoperative VFSS results and 12 had abnormal results, including penetration or aspiration or a significant amount of residue. A greater (50%) percentage of patients in the group with abnormal VFSS findings had C3 or C4 as the highest surgical level compared to that in patients in the normal VFSS group. The number of surgical levels (single vs. multiple) and the presence of dysphagia symptoms 4 weeks after surgery were not different between the normal and abnormal VFSS finding groups (Table 2).
Table 2
Comparison between normal and abnormal VFSS group according to factors of surgery

None of the patients reported dysphagia symptoms before surgery. Twelve of the 20 patients have more than moderate dysphagia symptoms in dysphagia score right after surgery. Nine patients had moderate dysphagia symptoms (dysphagia group) at the 1-month follow-up, and 11 had no or mild symptoms (control group) (Table 2).
No difference in operation time was observed between the patient groups without and with dysphagia immediately after the operation, or at the 1-month follow-up (P = 0.445). In contrast, mean operation time in the patient group with abnormal results on a VFSS (n = 12) performed < 1 week postoperatively was 180.8 ± 114.3 minutes which was significantly longer than the patient group (n = 8) without abnormal VFSS results (103.8 ± 44.1 minutes) (P = 0.048).
Changes in VFSS time parameters
Mean preoperative OTT was 0.30 ± 0.16 seconds, PTT was 0.89 ± 0.27 seconds, PDT was 0.24 ± 0.35 seconds, and PRT was 0.65 ± 0.23 seconds. Mean postoperative OTT was 0.34 ± 0.14 seconds, PTT was 0.87 ± 0.33 seconds, PDT was 0.44 ± 0.48 seconds, and PRT was 0.42 ± 0.33 seconds. OTT and PTT did not change significantly (P = 0.390 and 0.656). PDT tended to increase postoperatively (P = 0.091), and PRT decreased significantly (P = 0.049).
Analysis of hyoid bone movement
No difference in hyoid bone movement was detected between the normal VFSS and abnormal VFSS finding groups or between patients with and without dysphagia symptoms both immediately after surgery and 1 month after surgery (P > 0.05).
Maximal preoperative anterior movement distance of the hyoid bone was 37.78 ± 6.12 mm, and maximal distance of superior movement was 23.57 ± 10.81 mm. These distances were 39.18 ± 4.17 and 22.50 ± 6.69 mm, respectively after the surgery. No significant differences in anterior or superior displacement were detected before and after surgery (P = 0.098 and 0.597). No significant difference in travel time of the hyoid bone was observed before (1.09 ± 0.29 seconds) and after surgery (1.19 ± 0.33 seconds) (P = 0.270).
UES measurements
Maximal UES opening distance was significantly decreased from 6.82 ± 1.87 mm before surgery to 5.61 ± 1.70 mm after surgery (P = 0.044). Duration of UES opening changed only slightly from 0.50 ± 0.07 seconds to 0.53 ± 0.12 seconds after surgery (P = 0.094). However, the time elapsed since the UES started to open until its widest opening changed significantly from 0.16 ± 0.04 seconds before surgery to 0.20 ± 0.05 seconds after surgery (P = 0.002).
Maximal postoperative UES opening distance in the patient group with dysphagia immediately after surgery showed greater decrease (16.93% ± 0.34%) compared with that of the group without dysphagia (2.70% ± 0.42%), although there was no statistical significance (P = 0.439). At 1-month after surgery, patients without dysphagia showed a decrease of 12.8% ± 0.33% in UES opening distance, and patients with dysphagia showed a 9.4% ± 0.43% decrease, without statistical significance (P = 0.846).
The same comparison was performed in the groups with normal and abnormal postoperative VFSS results. As a result, maximal UES opening distance showed no significantly different decrease between the two groups (8.25% ± 0.35% in the normal VFSS group and 13.3% ± 0.40% in the abnormal VFSS group (P = 0.771).
The percentage decreases in maximal UES opening distance in patients whose highest operative levels were C3, C4, C4, and C6 were 18.4% ± 45.4%, 49.3% ± 10.5%, −4.6% ± 36.2%, and 6.2% ± 24.8%, respectively. The higher the operative level, the more the maximal UES opening distance decreased (P = 0.026).
Prevertebral soft tissue thickness
Preoperative prevertebral soft tissue thickness was 3.11 ± 0.81 mm at the C3 level, 4.29 ± 1.41 mm at the C4 level, 5.10 ± 1.62 mm at the C5 level, and 4.80 ± 2.06 mm at the C6 level. Postoperative prevertebral soft tissue thickness was 6.37 ± 2.07 mm at the C3 level, 7.55 ± 2.52 mm at the C4 level, 8.05 ± 2.59 mm at the C5 level, and 7.80 ± 2.70 mm at the C6 level. The percentage of prevertebral soft tissue thickness tended to increase at all levels after surgery, such as 115.33% ± 77.30% at the C3 level, 81.80% ± 50.02% at the C4 level, 68.05% ± 57.28% at the C5 level, and 84.60% ± 76.14% at the C6 level (Fig. 2A). These differences were not significant between the dysphagia and non-dysphagia groups immediately after surgery (P value was 0.851 on C3, 0.271 on C4, 0.467 on C5, and 0.31 on C6) (Fig. 2B) or 1 month after surgery (P value was 0.114 on C3, 0.087 on C4, 0.493 on C5, and 0.918 on C6) (Fig. 2C). However, the increase in prevertebral soft tissue thickness at the C3 level was 63.11% ± 57.95% in the normal VFSS group and 150.14% ± 69.83% in the abnormal VFSS group, which was statistically significant (P = 0.008) (Fig. 2D). The degrees of increase at the C4 level was also significantly greater in the abnormal VFSS group (99.27% ± 55.16%) than that in the normal VFSS group (55.60% ± 26.47%) (P = 0.030). However, no difference was detected between the normal and abnormal VFSS groups at the C5 or C6 levels (P = 0.123 and 0.500).
Fig. 2
Analysis of prevertebral soft tissue thickness. Prevertebral soft tissue thickness increased at all cervical levels (C3–C6) after surgery, and the percentages of increase were 115.33% at C3, 81.80% at C4, 68.05% at C5, and 84.60% at C6 (A). The degrees of increase at each level were not significant between the dysphagia and non-dysphagia groups immediately after surgery (B) or 1 month after surgery (C). The increase in prevertebral soft tissue thickness at C3 and C4 was significantly greater in the abnormal videofluoroscopic swallowing study (VFSS) group than that in the normal VFSS group (D).

DISCUSSION
The prevalence of dysphagia following ACDF varies, but the possibility of dysphagia should always be considered because the surgery involves the prevertebral soft tissue and multiple cervical levels in many cases. Our previous retrospective study suggested that ACDF increases the risks for dysphagia compared to inserting an artificial disc, and that a higher segment operation level also increases risks. Moreover, operating on multiple segments reveals even higher risks for dysphagia and can result in thicker cervical soft tissue 48 hours after the surgery, indicating that prevertebral soft tissue swelling is a cause for dysphagia after ACDF. In our study, a large proportion of patients who underwent ACDF reported subjective dysphagia symptoms, and they actually showed abnormal VFSS results. Moreover, patients whose surgeries were at a higher cervical level showed a higher incidence of abnormal VFSS results. Therefore, we concluded that a higher cervical level operation is proportionally correlated with subjective symptoms of dysphagia and abnormal VFSS results.
Patients with subjective dysphagia symptoms did not have abnormal VFSS results compared to patients without symptoms, and patients who developed dysphagia and those with abnormal VFSS results did not coincide. Considering that each patient has different perceptions, subjective dysphagia symptoms can vary. Severe sensory dysfunction immediately after surgery which could result in silent aspiration, should be evaluated through objective test tools such as VFSS, rather than relying on the subjective dysphagia symptoms. However, dysphagia symptoms, such as ‘a sense of regurgitation’ and ‘burning sensation in the throat’, suggest that the symptoms of dysphagia not only included swallowing dysfunction symptoms but also symptoms due to other causes, such as gastroesophageal reflux disease (GERD) (14), and uncomfortable throat due to physical stimulation after intubation, irritation by nonsteroidal antiinflammatory drugs used for pain control after surgery, discomfort after uncommon neck positioning for the surgery, and feeling irritation after contacting artificial materials. In one study, the initial GERD score (GIS) after ACDF and dysphagia severity after surgery were significantly correlated. The mechanism of this GERD-like symptom was not clear but esophageal dysmotility observed on VFSS was suggested as a cause. Esophageal dysmotility occurs when there is excessive pressure on esophageal wall by retractors used during the operation, leading to transient ischemia, swelling, and dysmotility.
The VFSS results revealed no change in PTT, but two subsections composes of PTT, PDT, and PRT showed changes after surgery. PDT, which is the time from the start of pharyngeal swallowing to the beginning of laryngeal elevation, was relatively longer after surgery. As this is closely related with provocation of the swallowing reflex, a change in the sensory function of the pharyngeal wall may occur after ACDF. In contrast, PRT, which is the time measured from the beginning of laryngeal elevation until the food bolus passes the UES, or UES closure was significantly shorter. This phenomenon could be explained by the significant decrease in mean UES opening diameter after the operation. In other words, this finding could be due to a small change in distance of the UES after ACDF compared to that before surgery, which is due to decreased pharyngeal wall motion, including the UES, and suggests motor dysfunction. No other studies have identified changes in an objective swallowing index by VFSS after ACDF before and after surgery. Most studies simply reported dysphagia incidence and severity after ACDF (151617).
Hyoid bone movement did not change significantly after surgery, and no difference was observed according to the existence of dysphagia or abnormal VFSS findings after surgery. Hyoid bone movement directly forces opening of the UES. In a recent study, pharyngeal wall thickness increased in 67 subjects after cervical surgery, which was suggested as a cause for the decline in pharyngeal constriction (12), and the pharyngeal constriction ratio was increased significantly in surgical patients compared to that in normal subjects. In our study, prevertebral soft tissue thickness after surgery increased significantly compared to that before surgery, which could reflect abnormal VFSS findings. Particularly, increased prevertebral soft tissue thickness after surgery was detected significantly more frequently in patients who had surgeries at the C3 and C4 levels, which are located in the upper pharyngeal wall. This finding explains the high percentage (six of seven patients) of abnormal VFSS findings in patients with their highest surgery level at C3 and C4, and who also showed significant declines in maximal distance of UES opening compared to patients whose surgeries were at the C5 level. In other words, operating at upper cervical levels resulted in more abnormal VFSS findings after surgery, increased soft tissue thickness, and a decline in maximal UES opening distance.
We suggest relying on more objective data related with swallowing dysfunction, such as VFSS, to assess patients after ACDF. Patients with their highest surgery level at C3 and C4 showed more abnormal VFSS findings after surgery, significantly increased soft tissue thickness, and decreased maximal UES opening distance.
 XML Download
XML Download