

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Upper urinary tract calculi (UUTC) are common. In the US, the lifetime risk of UUTC exceeds 12% in men and 6% in women, and the prevalence has increased in recent decades (12). The estimated lifetime prevalence rate in Seoul, Korea, was reported to be 3.5% in 1998 (6.0% in men and 1.8% in women) (3). In 2009, the annual incidence of UUTC in Korea was estimated to be 457 per 100,000 population, with 589.1 per 100,000 men and 326.6 per 100,000 women (4). Because of an increasingly Westernized diet, more sedentary lifestyle, and increase in obesity, the prevalence of UUTC in Korea is likely to increase.
Treatment options for UUTC range from conservative management to active surgical intervention depending on stone factors, patient characteristics, and doctor attributes (56789). UUTC are a highly prevalent and important healthcare problem, and recent studies in Western populations have examined treatment patterns and time trends (910111213). In contrast, despite the high prevalence of UUTC, similar studies in Asian population are lacking. In this study, we investigated national practice patterns and time trends in treatment of UUTC in Korea using a nationwide, population based cohort, and also assessed the impact of sociodemographic factors on primary treatment choices.
MATERIALS AND METHODS
Data sources and study population
Virtually all South Koreans (97%) are covered by National Health Insurance (NHI) (14). The Korean NHI Corporation recently established a research database with a 2% sample of the Korean population (> 1 million people), that was randomly selected after stratifying socioeconomic parameters (age, sex, income, residential area, etc.) (15). The Korean NHI database provides de-identified claims data from 2002 to 2013 regarding disease diagnosis, imaging and laboratory tests, and treatments (both medical and surgical), in addition to socioeconomic parameters.
Patients with codes for UUTC disease (N20, N20.0, N20.1, N20.2, N20.9, and N23) according to the International Classification of Diseases, 10th edition (ICD-10), were identified (n = 41,450). Patients who did not undergo active treatment for UUTC (n = 26,715) were excluded. In addition, to minimize confounding effects due to pre-diagnosed UUTC, those with claims submitted for UUTC in 2002 were excluded (n = 453). Thus, a total of 14,282 patients who had received active treatment, including shock wave lithotripsy (SWL), ureteroscopic surgery (URS), percutaneous nephrolithotomy (PNL), and uretero/pyelolithotomy (UPL), for newly diagnosed UUTC constituted the study population.
Treatment pattern and operational definition
We analyzed patterns for both primary treatment and all treatment cases. For these analyses, we examined the administration and timing of additional treatment after primary treatment. Because retreatment for residual or recurrent stones is common after initial primary treatment, we operationally defined recurrence by limiting the interval between 2 urolithiasis treatments to more than 180 days, as described in another study (16). Thus, if the interval between initial and subsequent treatment was less than 180 days, the subsequent treatment was regarded as additional treatment for residual fragments, which is an extended part of primary treatment. Additionally, to minimize possible bias due to our operational definition, we analyzed national trends of all treatment cases, including treatments beyond primary treatment.
Outcome variables and statistical analysis
Primary outcome variables were annual time trends in primary treatment and all treatment cases. Secondary outcome variables included association of sociodemographic factors with treatment choice. Patient sociodemographic parameters included age, sex, income class, and residential area. Patient age at diagnosis was divided into 5 categories (< 30, 30–39, 40–49, 50–59, and ≥ 60 years). Income class was divided into 5 categories, by 20th percentiles. Residential area was divided into 3 categories (metropolitan, urban, and suburban/rural) based on population density.
Descriptive statistics were used to characterize trends in treatment of UUTC over time. Pearson χ2 tests were used to determine whether there was a significant difference between the groups in terms of variable frequencies. Annual P for trend was determined by a Wilcoxon-type test for trend across ordered groups. Multivariable multinomial logistic regression analysis was used to determine the adjusted odds ratios (aOR) and 95% confidence intervals (CI) of sociodemographic factors that were significantly associated with treatment choices (based on the SWL group). Recurrence-free survival (RFS) after primary treatment was also analyzed according to the operational definition, where recurrence was defined as treatment beyond 180 days since first treatment date. To show descriptive RFS, Kaplan-Meier curves were generated with the log rank test. All tests were two-tailed, with P < 0.05 considered significant. Statistical analysis was performed using Stata/SE software, version 12.1 (Stata Corporation, College Station, TX, USA).
RESULTS
Characteristics of the study population
Table 1 summarizes the patient sociodemographic factors. Mean age at diagnosis was 40.4 years (standard deviation [SD], 13.9 years), and 69.1% were male. There were 1,934 patients (13.5%) in the lowest income classes (class 0–2), and the greatest percentage (27.8%) was in the highest income classes (class 9–10). About half (48.9%) of the patients lived in urban areas, and 32.4% lived in suburban or rural areas. The majority (92.4%) of patients underwent SWL as primary treatment, while 6.4%, 0.8%, and 0.4%, respectively, underwent URS, PNL, and UPL as primary treatment (Table 1). There was a significant difference in primary treatment according to age, sex, and region (all P < 0.001).
Table 1
Basic characteristics of study population
SWL = shock wave lithotripsy, URS = ureteroscopic surgery, PNL = percutaneous nephrolithotomy, UPL = uretero/pyelolithotomy.
*P values determined by χ2 test.
![]()
Treatment pattern and annual trends
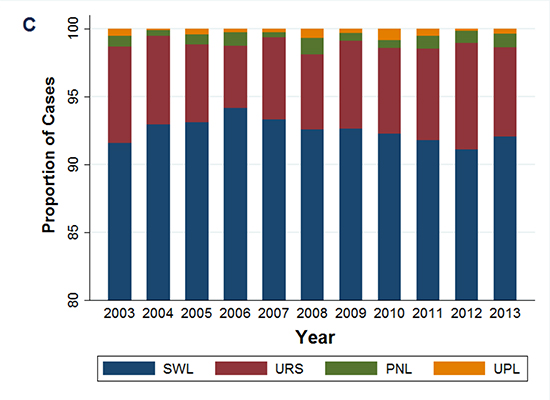
The overall number of primary treatments for UUTC increased from 1,010 in 2003 to 1,444 in 2013, corresponding to an increase of 43% in 10 years (Fig. 1A). Patients undergoing SWL, URS, PNL, and UPL as primary treatment increased by 43.7%, 31.9%, 87.5%, and 0%, respectively, between 2003 and 2013 (Fig. 1A, P for trend = 0.035, 0.085, 0.201, 0.719, respectively). Similarly, the number of all treatment cases increased from 1,036 in 2003 to 2,106 in 2013, corresponding to an increase of 103.3% (Fig. 1B). Total cases of SWL, URS, PNL, and UPL increased by 102%, 110%, 180%, and 0%, respectively, between 2003 and 2013 (Fig. 1B, P for trend ≤ 0.001, 0.001, 0.087, 0.357, respectively).
 | Fig. 1Time trends of upper urinary tract calculi in Korea’s primary treatment (A) and all treatment cases (B) for Time trends for the relative proportions of primary treatments (C) and all treatment cases (D) are also shown.
SWL = shock wave lithotripsy, URS = ureteroscopic surgery, PNL = percutaneous nephrolithotomy, UPL = uretero/pyelolithotomy.
|
While the number of primary treatments and all treatment cases, particularly SWL and URS, significantly increased (Fig. 1A and B), the relative proportion of each treatment remained roughly constant over 10 years (Fig. 1C and D); thus, SWL, URS, PNL, and UPL accounted for > 90%, 4.5% to 7.8%, 0.4% to 1.0%, and < 0.4%, respectively, of active treatments throughout the study period.
Association between sociodemographic factors and treatment modality choice
As shown in Table 2, age > 40 years (compared to < 30 years) was significantly associated with URS (aOR = 1.27 to 1.92), PNL (aOR = 2.67 to 7.46), and UPL (aOR = 4.85 to 15.98), rather than SWL. Female gender was significantly associated with URS rather than SWL (aOR = 1.58, 95% CI 1.38–1.82), whereas income levels was not associated with treatment choice. Patients living in urban or suburban/rural areas (compared to metropolitan) were significantly less likely to undergo URS (aOR = 0.54 to 0.56) and PNL (aOR = 0.41 to 0.61), and those living in suburban/rural areas were significantly less likely to undergo UPL than SWL (aOR = 0.42, 95% CI 0.20–0.89).
Table 2
Association of sociodemographic factors with primary treatment modality for upper urinary tract calculi (compared to SWL Group)
Analyzed by multinomial regression analysis with SWL group as reference group, adjusted by year of primary treatment.
SWL = shock wave lithotripsy, URS = ureteroscopic surgery, PNL = percutaneous nephrolithotomy, UPL = uretero/pyelolithotomy, aOR = adjusted odds ratio, CI = confidence interval.
![]()
Stone recurrence after initial treatment
Median follow-up period of the study population was 45.7 months. Among 14,282 patients, 2,662 (18.6%) experienced stone recurrence at a mean of 24.7 months (interquartile range 11.5 to 46.9 months). In the entire cohort, RFS rates at 2, 5, and 10 years were 89.0%, 78.1%, and 65.4%, respectively (Fig. 2A). According to treatment modalities, 5-year RFS rates were 78.1%, 79.7%, 59.6%, and 86.7% for SWL, URS, PNL, and UPL groups, respectively. Patients who underwent PNL had significantly lower RFS rates than those who underwent other treatments (log-rank P < 0.001, Fig. 2B).

DISCUSSION
To our knowledge, this is the first study to investigate national treatment patterns and time trends in patients with UUTC over a 10-year period in Korea. UUTC is highly prevalent in Korea and its prevalence is likely to increase (34). As in Western studies (101112), the number of patients undergoing active treatment for UUTC significantly increased over a 10-year period in Korea. As shown in Fig. 1A and B, primary treatment and all treatment cases increased by 43% and 103.3%, respectively.
There were 2 main findings regarding treatment patterns for UUTC and time trends in Korea: the majority (> 90%) of Korean patients underwent SWL as primary treatment for UUTC, and the predominant use of SWL remained steady over 10 years (Fig. 1C and D), although the number of all URS cases significantly increased (P for trend = 0.001). SWL is an acceptable first-line treatment for UUTC requiring stone removal (56). Similarly, in a US study based on data from the American Board of Urology, SWL was the most commonly performed procedure for UUTC between 2003 and 2008 (8). Notably, the predominant use of SWL throughout the study period (2003 to 2013) is a unique finding in Korea. In contrast to a prior study (8), recent US studies have shown increased use of URS for UUTC and a corresponding decrease of SWL over time (1213). Seklehner et al. (12) showed that URS for the treatment of ureteral calculi increased from 2001 to 2010, while the use of SWL declined. Oberlin et al. (13) showed that from 2003 to 2012, there was an increase in URS for the treatment of UUTC from 40.9% to 59.6%, and a corresponding decrease in SWL from 54% to 36.3%.
Several recent studies investigated treatment patterns of UUTC and changing trends over time. Table 3 summarizes the results of published studies. Although the aforementioned 2 US studies have shown that SWL is gradually being replaced by URS over time as a primary treatment for UUTC (1213), an Australian study showed an increased use of URS and steady use of SWL from 1995 to 2010 (10). Meanwhile, a UK study showed an increase in both SWL and URS use for the treatment of UUTC between 2000 and 2010 (11). Discrepancies in time trends for UUTC treatment among countries may reflect differences in health care systems, availability of medical services, financial barriers, differences in patient perception, and provider behavior (1217). Although the results are slightly different among studies (Table 3), most Western studies have shown that the role of URS as a primary treatment for UUTC has become increasingly more important than SWL. The main reason for this trend is probably associated with higher and faster stone-free rates and lower retreatment rates with URS than with SWL (51819), although other studies have shown conflicting results regarding treatment outcomes after URS (202122).
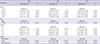
Table 3
Summary of published studies that investigated treatment patterns for urinary lithiasis and time trends

| References | Year | Nation | Subjects | Study period | Main findings of the study |
|---|---|---|---|---|---|
| Matlaga et al. (8) | 2009 | USA | UUTC (data from American Board of Urology) | 2003–2008 | *Provider specific attributes affect treatment choice. |
| Scales et al.(9) | 2011 | USA | UUTC (Medicare 5% sample) | 1997–2007 | *Nonclinical factors are associated with the use of URS or SWL. |
| Lee and Bariol (10) | 2011 | Australia | UUTC (Medicare Australia and Australian Institute of Health and Welfare databases) | 1995–2010 | An increase in URS, Steady use of SWL. |
| Turney et al. (11) | 2012 | UK | UUTC (data from the Hospital Episode Statistics website) | 2000–2010 | An increase in both SWL and URS use. |
| Seklehner et al. (12) | 2014 | USA | Ureter calculi only (5% Medicare Public Use Files) | 2001, 2004, 2007, and 2010 | The use of URS increased over time, while the use of SWL declined. |
| Oberlin et al. (13) | 2015 | USA | UUTC (data from American Board of Urology) | 2003–2012 | An increase in URS and a corresponding decrease in SWL over time. |
| Present study | - | Korea | UUTC (2% random sample from Korean National Health Insurance database) | 2003–2013 | Dominant use of SWL remained steady. |
UUTC = upper urinary tract calculi, SWL = shock wave lithotripsy, URS = ureteroscopic surgery.
*No data regarding time trends (cross-sectional finding only).
![]()
The predominant use of SWL as primary treatment for UUTC in Korea may be attributable to various factors. First, significant proportions of patients with UUTC in Korea are primarily treated by urologists in private practice, most of whom own an SWL instrument but do not perform URS. Similar to this finding, Childs et al. (18) reported that urologists reporting SWL ownership were 3–4 times more likely to select SWL for UUTC compared with urologists who did not own a lithotripter. Secondly, because the SWL fee reimbursed by the Korean NHI is relatively higher than that for URS, doctors are likely to choose SWL as primary treatment. Thirdly, patient preference may also affect treatment patterns in Korea. In prior studies including ours (623), patient-reported satisfaction was higher after SWL than URS, although routine stenting after URS might partly account for lower patient satisfaction. Consistent with prior studies demonstrating that economic, doctor, and patient attributes affect treatment choice for UUTC (8923), we believe that such nonclinical factors may be, at least in part, responsible for treatment patterns in Korea.
Our results show that sociodemographic factors do affect primary treatment choice for UUTC. Several sociodemographic factors (i.e., age, sex, and residential area) affected treatment choice even after adjusting for other parameters (Table 2). The finding that age older than 40 years was significantly associated with URS, PNL, and UPL compared to SWL may indicate the presence of larger and more complicated stones in those patients, compared to patients younger than 30 years. Female gender was significantly associated with URS compared to SWL, consistent with a previous study (12). Interestingly, patients living in urban or suburban/rural areas were significantly less likely to undergo endourologic treatments such as URS and PNL, compared with patients living in metropolitan areas. This finding may be due to differences in instrument availability and preferred treatment method according to region. Similarly, geographical variation was reported to affect preferred treatment methods for UUTC in US studies (1217).
We found that Korean patients with UUTC frequently experience stone recurrence, with 5- and 10-year RFS rates of 78.1% and 65.4%, respectively (Fig. 2A). As expected, patients who underwent PNL had significantly lower RFS rates than those who underwent other treatments (Fig. 2B), indicating that PNL was more likely to be used for larger, multiple, and more complicated stones, with a greater likelihood of recurrence.
We acknowledge several limitations of our study. Because the NHI data did not include such information, we could not assess treatment patterns according to stone characteristics (size, location, and composition, etc.). For the same reason, caution is needed in the interpretation of our stone recurrence data after primary treatment. Our study lacked data regarding conservative management including medical expulsive therapy, which is a reasonable treatment option for small UUTC. However, our data were based on a nationwide, randomly selected population-based cohort, thus making our results generalizable to the entire Korean population. Inclusion of all active treatment modalities (SWL, URS, PNL, and UPL) and analysis based on longitudinal follow-up is another strength. As the results for all treatment cases showed similar time trends, possible bias associated with our operational definition of primary treatment, based on a 180-day cut-off (16), is most likely to be minimal.
In summary, the majority of Korean patients underwent SWL as primary treatment for UUTC, and the predominant use of SWL remained steady over a 10-year period. Sociodemographic factors affected the primary treatment choice for UUTC. Better understanding of patterns of care will provide more insight into the current status of treatment of Korean patients with UUTC. Our results will be valuable in examining treatment patterns and time trends in Korean UUTC patients.
 XML Download
XML Download