

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Approximately one-third of patients with newly-diagnosed renal cell carcinoma (RCC) have an advanced disease state, and a significant proportion of these patients are inoperable, which results in a dismal prognosis, as surgical removal of the renal tumor is the only proven therapy for complete remission (1). However, the emergence of new antiangiogenic therapies has improved the prognosis of patients with metastatic RCC (mRCC), and targeted therapies (TT) can now be integrated with surgical treatment to optimize outcomes for patients with inoperable advanced RCC (1). The potential tumor shrinkage may also permit easier surgical resection. Neoadjuvant therapy (NT), which refers to presurgical treatment for unresectable cancer, may be useful for decreasing the tumor’s volume to increase resectability. Furthermore, NT may improve outcomes in patients with renal cancer by reducing the risk of postoperative recurrence, eradicating micrometastatic disease, increasing the likelihood of curative therapy, maximizing nephron sparing and renal function, and enhancing the molecular effects of TT to overcome drug resistance (2,3).
The concept of NT was not prominent in the era of cytokine-based systemic therapy for mRCC. Furthermore, these treatment regimens are relatively ineffective for managing metastases as long as the primary tumor remains in situ, and the cytokine-based therapies did not provide a significant reduction in the primary tumor’s size (4). However, during the current era of TT, NT strategies have regained the attention of oncologists, and several trials of NT for RCC and mRCC have recently been completed or are ongoing (567). Some trials have established the safety and response rates of NT with several agents, but there is no consensus in the literature regarding the effectiveness, safety, and clinical utility of NT (8). Therefore, the possible or conceivable indications for neoadjuvant TT now include the treatment of 1) large unresectable advanced tumors to facilitate surgery, 2) imperative indications to enable a nephron-sparing procedure, and 3) high-level vena cava thrombi involvement to achieve downsizing and facilitate the use of simpler surgical techniques that are associated with lower morbidity rates. However, there are no consensus indications for NT in RCC.
In the present study, we prospectively enrolled 14 patients with mRCC from 5 academic hospitals to evaluate the response of the inoperable primary tumor to 2-cycle neoadjuvant sunitinib therapy (NST). The objective for this study was to evaluate the treatment’s efficacy, safety, and tolerability (including changes in quality of life [QoL]). Sunitinib was chosen as the targeted agent because it is the most extensively investigated TT agent, and is likely the most suitable agent for NT, given its ability to shrink the primary tumor (6,9).
MATERIALS AND METHODS
Between June 2009 and September 2012, 14 patients with inoperable clear cell mRCC were enrolled from 5 Korean academic hospitals (National Cancer Center, Seoul Samsung Medical Center, Kyung Hee University Hospital at Gangdong, Kyungpook National University Hospital, and Chungbuk National University Hospital). These patients all received 2-cycle sunitinib (50 mg/day for 4 weeks, followed by a 2-week hiatus) as neoadjuvant TT. The decision to administer NST was made on an individual basis at the discretion of the treating urologist, and was not prospectively specified at the participating institutions. The patients’ baseline clinical data were prospectively collected (Table 1), and included the Memorial Sloan Kettering Cancer Center (MSKCC) risk stratification (10), pathological data with the 2010 TNM stage (11) after percutaneous biopsy, and adverse events based on version 4.0 of the NCI Common Terminology Criteria for Adverse Events (CTCAE) (12). Quality of life was evaluated before and after the NST according to the specific domains of the European Organization for the Research and Treatment of Cancer (EORTC) Quality of Life Questionnaire (QLQ)-C30 (a 30-item questionnaire that is available at: http://groups.eortc.be/qol/eortc-qlq-c30) (13).
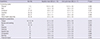
Table 1
Baseline demographics (n = 14)

ECOG = Eastern Cooperative Oncology Group, MSKCC = Memorial Sloane Kettering Cancer Center, BUN = blood urea nitrogen, AST = aspartate aminotransferase, ALT = alanine aminotransferase, TNM = tumor-node-metastasis, RECIST = Response Evaluation Criteria In Solid Tumors.
![]()
All subsequent imaging results underwent a central review at each institution to detect any change in the size of the primary tumor. The tumor thrombus level was defined according to Novick’s classification (14). The objective clinical response of the primary tumor and the overall disease response were assessed according to the Response Evaluation Criteria In Solid Tumors criteria (RECIST version 1.0) by the treating physician and the central review, using findings from computed tomography (CT), magnetic resonance imaging, or 18-fluoro-2-deoxyglucose positron emission tomography/CT. The follow-up protocol was the same for all participating institutions, and included a physical examination, blood analyses, and abdominal imaging using ultrasonography, CT, and whole-body positron emission tomography/CT at the end of each cycle.
The median times to disease progression or death were assessed from the diagnosis date to the date of disease progression, or to the date of cancer-specific death or last follow-up, respectively. A Wilcoxon signed rank test was used to compare the summary scores from before and after NST. All analyses were performed using Stata software (version 9.2; StataCorp, College Station, TX, USA), and a P value of < 0.05 was considered statistically significant.
Ethics statement
This study’s design was approved by each institution’s ethical review board, and by the ethical review board of the Research Institute and Hospital National Cancer Center (IRB No. NCCTSC09414, Clinical trial registry 1041140-1). All patients provided their voluntary written consent to participate in this study, and their records/information were anonymized and de-identified prior to the analysis. All study protocols complied with the ethical guidelines of the Declaration of Helsinki.
RESULTS
The patients’ characteristics and adverse events are described in Table 1. Among the 14 patients, 5 patients (35.7%) did not complete the treatment due to disease progression (n = 1, 7.1%; death occurred at 2.2 months after enrollment), voluntary withdrawal (n = 1, 7.1%), or grade 3 adverse events (n = 3, 21.4%), which included 2 cases of hypertension and 1 case of hand-foot syndrome (Table 1).
The 9 patients (64.3%) who completed treatment exhibited 2 partial responses (22.2%) and 7 stable overall diseases (77.8%), based on the RECIST criteria. These patients were considered inoperable at enrollment due to the presence of stage II or III intra-vena cava thrombi with either a large tumor burden or invasion of the neighboring vital organs. At the end of the study, 7 patients (77.8%) were converted to an operable status, and 4 of these patients (28.6%) ultimately underwent surgery, including 2 patients who underwent successful partial nephrectomy.
The median baseline primary tumor diameter was 10.3 cm (range: 6.6–15.8 cm), and the median reduction was −13.5% (range: −20% to 0%). The baseline CT images revealed 18 measurable metastatic lesions and 15 unmeasurable lesions. The 18 measurable lesions included 2 unresponsive lesions and exhibited a median reduction of −20.2% (range: −101% to 0%), and the 15 unmeasurable lesions decreased or disappeared (Fig. 1, Table 2).

Table 2
Tumor responses after sunitinib therapy (n = 9)

PR = partial response, SD = stable disease, CR = complete response, RECIST = Response Evaluation Criteria In Solid Tumors.
![]()
For the QoL assessment, only 7 patients (77.8%) completed the questionnaires after the NST, and their composite QoL scores are presented according to the specific domains in Table 2. The mean baseline global QoL score for the cohort was 8.3 ± 4.6, which significantly decreased to 8.0 after the NST (P = 0.019), although significant increases were observed for fatigue, nausea and vomiting, and the financial effect of NST (all, P < 0.05).
DISCUSSION
Cytoreductive nephrectomy or metastasectomy, as either primary therapy for a limited metastatic burden or as part of a surgical consolidation strategy after a partial response to systemic NT, is associated with an improved prognosis (15). However, the surgical benefits after NT in mRCC have generally been observed during the immunotherapy era. While the use of preoperative TT in the setting of locally advanced or metastatic RCC (mRCC) remains in its preliminary stages, with only a few retrospective studies and case reports (2161718), there is a growing body of evidence that may support its role in a select group of patients (8). Therefore, the present study is significant because few studies have evaluated neoadjuvant TT in Asian populations (19), and, to the best of our knowledge, this is the first and only study of NT using a targeted agent in Korean patients with mRCC.
Previous reports of successful TT as NT have confirmed its efficacy in RCC and other malignancies, such as colorectal, pancreatic, and urothelial cancers (6920). Although it is clear that both surgery and NT have a role in the management of mRCC, the optimal integration of these 2 modalities remains unclear (especially when TTs are used as NT). Nevertheless, recent studies of NT have provided evidence that it can provide real-time clinical feedback regarding the patient’s responsiveness (e.g., overall tumor burden) to a specific TT before performing surgical procedures that may be associated with a high risk of morbidity or mortality. Thus, NT could be useful to downstage the primary tumor, reduce the complexity and risk of surgical removal, eliminate micrometastatic disease, and ultimately reduce the postoperative risk of metastatic progression (921).
In the present study, 2-cycle sunitinib therapy was selected to evaluate the tolerability and efficacy of NT (31617). No cases of perioperative morbidity or major intraoperative complications were observed during this study. However, this treatment was unsatisfactory, based on a tolerability of 64.2% (n = 9) during the NST and a drop-out rate of 28.6% (n = 4) because of disease progression and adverse events. Furthermore, 21.4% of the overall adverse events during the NST were grade 3 hypertension or grade 3 hand-foot syndrome, which resolved after sunitinib discontinuation and adequate medical treatment.
The RECIST criteria are most suitable grading system for a global assessment of the best overall response in tumor burden, especially for primary renal tumors, which tend to be large and exhibit a relatively small decrease in size after treatment, compared to the responses of metastases (32223). In the present study, NST provided an unsatisfactory partial response rate of 22.2%, despite the disease control rate of 64.3% among the 9 patients who completed treatment. For the primary tumor, we observed a median diameter reduction of 1.3 cm (range: 0.1–2.8 cm) and a burden reduction of 13.5%, as well as diameter reductions of 0.2–0.8 cm and burden reductions of 20.2% for the metastatic lesions. These results are similar to the findings of previous studies, which revealed a limited overall response rate (7%–30%), a progression rate of 11%–27.3%, and that only 10%–57.9% of cases exhibited a reduction in the primary tumor’s size (6232425). In addition, 7 patients (50.0%) from the present study were considered operable after the NST, although only 4 patients (28.6%) underwent successful nephrectomy. This finding is consistent with the surgical success rates of 10%–57.9% from previous series (6).
We observed median overall survival times of 12.2 months from treatment initiation (range: 5.8–21.3 months) and 6.2 months from treatment completion (range: 0.7–16.2 months) (Table 1 and data not shown). At the end of the study, 5 of the 9 patients (55.6%) who completed the treatment remained alive, although there were no significant differences in the survival outcomes for patients who underwent nephrectomy (n = 4) or who did not undergo nephrectomy (n = 5) (11.7 months [range: 1.7–13.9 months] vs. 5.9 months [range: 0.7–16.2 months], respectively; P = 0.082). Nevertheless, this trend towards an increased survival after nephrectomy has also been reported by Wood and Margalis (31.1 months vs. 27.7 months, respectively; P = 0.697) (21). Furthermore, 2 of the 4 patients who underwent nephrectomy subsequently received adjuvant sunitinib therapy (7.4 months and 5.5. months), which resulted in a median progression-free survival of 12.2 months (range: 5.8–21.3 months) until the end of the study.
The effect on tumor thrombi in 2 patients exhibited a good response, with safe resectability after undergoing NST in this study. These patients successfully underwent inferior vena cava thrombectomy, although the changes in the dimensions of the thrombi were not calculated. Nevertheless, it is intriguing to consider the use of TT to achieve operable tumor status or to promote the regression of regionally advanced tumor thrombi. A previous study of 25 patients who received NT reported a 44% reduction in thrombi height above the renal vein after NT, as well as a 48% reduction in the primary thrombus mass (24). However, the median decrease in the thrombus diameter was < 1 cm, and downstaging of the thrombus was only achieved in 3 patients (12%). Furthermore, previous studies have reported progression of a local tumor or tumor thrombus in approximately 20%–25% of patients during NT, which would indicate that NT should only be considered in exceptional cases or in patients who are deemed absolutely inoperable (6).
The current study also evaluated patients’ quality of life using the EORTC QoL-questionnaire, which is used for a variety of malignancies and incorporates several distinct domains regarding symptoms (nausea, vomiting, pain, and fatigue) and functional status (physical, social, emotional, and cognitive functioning) (13). The questionnaire results revealed that the patients’ general health status improved significantly (P = 0.019), although fatigue, nausea and vomiting, and the financial effect of NST were the most significant detrimental factors that affected patients’ QoL during 2-cycle NST (Table 3, all, P < 0.05).
Table 3
Changes in quality of life during therapy, as assessed using the Korean version of the EORTC QLQ-C30 questionnaire (n = 13)
Scores range from 1 to 4, with a higher score representing a higher level of functioning and symptoms.
EORTC = European Organization for the Research and Treatment of Cancer, QLQ = quality of life questionnaire.
![]()
This study contains several limitations that warrant consideration. First, we only evaluated a small number of patients, and our results should not be extrapolated to other patients and populations. Second, we observed a limited completion rate (64.3%), which limits our ability to draw positive conclusions regarding the efficacy of NST, as cytoreductive nephrectomy was infrequently performed despite the conversion to operable status after NST. Third, it is possible that our findings were influenced by subjective policies when the physicians evaluated the tumors’ operability at the participating institutions.
Conclusively in this study, two-cycle NST provided disappointing efficacy and tolerability, with limited clinical benefits, for select patients with inoperable mRCC. However, a small subset of patients experienced conversion to an operable status, without disease progression and with few side effects and satisfactory safety. It is important to consider perioperative morbidity when selecting patients with mRCC for NST.
 XML Download
XML Download