

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Renal cell carcinoma (RCC) accounts for 3% to 6% of all adult malignancies and 85% of malignant kidney tumors (1). Similar to other tumor entities, RCC presents with significant clinical heterogeneity and ranges from indolent to highly aggressive (2). The identification of accurate predictors of clinical outcome is imperative to determine individualized follow-up strategies and to facilitate counseling regarding adjuvant therapy. Many clinical and histological factors, including TNM stage, nuclear grade, histological type, and performance status, have prognostic implications for RCC (345).
Younger age is a significant prognostic factor for survival in numerous malignancies, such as breast cancer, thyroid carcinoma, and cervical and ovarian carcinoma (67891011). The role of age at diagnosis in the prognosis of RCC has been researched extensively; however, the prognostic significance of age in RCC is a subject of debate and remains to be clarified. Previous studies reported contradictory findings on the role of age as a prognostic factor in patients with RCC. One study reported that young RCC patients had unfavorable histologic features and better survival, whereas other studies reported that younger patients had a favorable histological subtype and pathological features, and better survival than older patients (12131415). Several studies failed to detect a significant association between age and prognostic features (161718). In addition, the small number of patients with early onset RCC is a limitation of most previous studies (19). RCC develops predominantly in the sixth decade of life and is rare among young adults, which account for 3%–5% of all RCC cases. Current evidence of the prognostic impact of age in RCC is drawn from approximately 1,500–2,000 patients reported in the literature; therefore, further data are needed.
The aim of the present multi-institutional study was to assess the influence of age on the pathological features of RCC and to determine whether age is an independent prognostic factor for survival in a large cohort of patients with RCC, including 541 cases of early onset RCC.
MATERIALS AND METHODS
Study population
Approval for the study was obtained from the relevant institutional review boards of the eight participating centers. A database of 7,047 patients with RCC who were treated surgically between 1999 and 2011 at eight academic centers was reviewed. The database listed patient clinicopathologic characteristics including age at diagnosis, gender, body mass index (BMI), comorbidities (diabetes and hypertension), Eastern Cooperative Oncology Group (ECOG) performance status, surgical approach (open vs. laparoscopic), clinical tumor characteristics (tumor location, cTNM stage), tumor pathology (histologic tumor size, pTN stage, Fuhrman nuclear grade, histologic subtype, lymphovascular invasion, and surgical margin status), disease recurrence and site of recurrence (local or metastatic), and information on deaths and their causes (20). Patients with an incomplete data set (n = 1,457) and those with non-RCC pathology or pediatric RCC patients (younger than 18 years) (n = 412) were excluded; the final study group comprised 5,178 patients.
Protocols for surgery and pathologic evaluation
The surgical procedures performed included pure laparoscopic, hand-assisted laparoscopic, robot-assisted, and open approaches. Surgical modality and approach were decided by each surgeon according to the individual clinical situation. All surgeries were performed by skilled surgeons using standard methods. Surgical techniques varied widely and were heterogeneous because eight academic centers were included in the retrospective review. All surgical specimens were processed according to the standard pathologic procedures at each institution. Pathological staging was performed based on the 7th edition of the American Joint Committee on Cancer classification system, and histological differentiation was graded according to the Fuhrman nuclear grading system (2122).
Follow-up protocol
After surgery, each patient was monitored according to standard guidelines(34). In general, patients were followed-up every 3–6 months. Follow-up consisted of history, physical examination, routine blood and serum chemistry lab work, chest radiography, and abdominal computed tomography (CT). Elective bone scan or magnetic resonance imaging or positron emission tomography-CT was performed when clinically indicated. Recurrence was defined as local relapse, lymph node metastasis, and distant metastasis.
Statistical analysis
Patients were categorized into three groups according to age at diagnosis as follows: a young age group (< 40 years, n = 541), a middle-age group (≥ 40 and < 60 years, n = 2,551), and an old age group (≥ 60 years, n = 2,096). Clinical and pathological features were compared between the age groups using the χ2 test for categorical variables and ANOVA with Bonferroni’s post-hoc test for continuous variables. Kaplan-Meier analyses with log rank tests were then used to compare survival rates between the different groups. A Cox proportional hazards model was used to assess the independent prognostic value of age and to determine the hazard ratios of patients according to age category. Differences were considered significant at P < 0.05, and all reported P values are two-sided. Analyses were performed using SPSS 20.0 software (IBM Corp., Armonk, NY, USA).
Ethics statement
The study was carried out in agreement with the applicable laws and regulations, good clinical practices, and ethical principles as described in the Declaration of Helsinki. The institutional review board of Chungbuk National University approved this study protocol (approval number: GR2014-12-009). Informed consent was waived by the board.
RESULTS
Comparison of clinical, operative, and pathologic variables according to age at diagnosis
Table 1 lists the demographic and clinical features of patients in the different age categories. Tobacco exposure was more common in the young age group than in the other groups (P < 0.001). The male to female ratio was lower in the old age group than in the young and middle-age groups (P = 0.010). The prevalence of diabetes or hypertension increased significantly with age, and a better performance status was observed in the young and middle-age groups (P < 0.001, each). Incidental tumor detection was more common in the middle-age group than in the young and old age groups (79.3% vs. 76.1% and 75.4%, respectively, P = 0.007). Nephron sparing surgery was more frequent in the young and middle-age groups with more imperative indication than in the old age group (P < 0.001, P = 0.049, respectively).
Table 1
Baseline characteristics of the study cohort according to age in patients with surgically-treated renal cell carcinoma

Regarding pathologic features, the young age group had tumors of lower stage and nuclear grade, and had a lower proportion of lymphovascular invasion than the other age groups (P < 0.001, P = 0.003, and P = 0.031, respectively). Additionally, there were significant differences in histologic type according to age (P < 0.001). The young age group had a lower incidence of clear cell RCC and a greater incidence of Xp11.2 translocation RCC than the other age groups. The proportions of other histologic subtypes were similar between the three groups (P < 0.001). However, no differences in operative methods, tumor laterality, mean tumor size, or positive surgical margin rate were observed between the groups (Table 2).
Table 2
Comparison of operative and pathological variables between age groups in patients with surgically-treated renal cell carcinoma

Survival analysis according to age at diagnosis
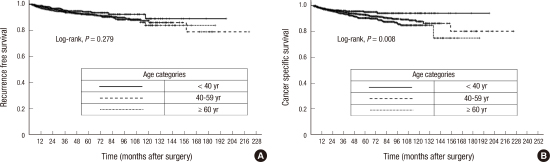
A total of 4,588 patients (88.6%) who were followed for ≥ 3 months (median: 37.0 months, range: 3–225 months) were included in the survival analyses. Evaluation of the influence of age at diagnosis on recurrence-free survival (RFS) or cancer-specific survival (CSS) in the young, middle, and old age groups showed 5-year RFS rates of 93.4%, 92.3%, and 91.8%, respectively, with no significant differences according to age (P = 0.279; Fig. 1A), and 5-year CSS rates of 94.2%, 92.9%, and 90.2%, respectively. Kaplan-Meier analysis showed that the CSS was longer in the young age group than in the other age groups (P = 0.008; Fig. 1B).
Fig. 1
Kaplan-Meier survival curves. (A) Recurrence-free survival, (B) Cancer-specific survival according to age categories in patients with surgically-treated renal cell carcinoma.

A multivariate Cox regression analysis was performed by including significant factors from the univariate analysis, which showed that the presence of diabetes, preoperative BMI, TNM stage, Fuhrman grade, lymphovascular invasion, and chromophobe tumor histology were independent predictors of CSS. However, age at diagnosis was not an independent predictor of CSS as a categorical variable (Table 3) or a continuous variable (data not shown) on multivariate analysis.
Table 3
Univariate and multivariate Cox regression models for the prediction of cancer-specific mortality in patients with surgically-treated renal cell carcinoma
DISCUSSION
The current study assessed the prognostic impact of age at diagnosis in a large, multi-institutional cohort of patients with surgically-treated RCC in Korea. Our results indicated that young age at diagnosis is closely related to favorable pathologic features and prolonged CSS; however, age was not an independent prognostic factor for CSS in RCC.
Well-known anatomical and clinicopathological features, including TNM stage, Fuhrman nuclear grade, histologic subtype, and performance status have been implicated for RCC prognosis (3421). The prognostic significance of age at diagnosis was also suggested in RCC; however, there are conflicting reports about the impact of age on tumor aggressiveness or oncological outcomes in patients with RCC (1121823). In a surgical series of 89 patients including young adults (≤ 40 years), no significant difference in CSS was detected between the different age groups (18). Similarly, Gillett et al. (23) compared CSS rates between 124 patients aged 18–40 years and 1,067 patients aged 60–70 years, and failed to detect significant differences between the groups. However, contemporary series in the literature reported favorable histological subtypes and pathological features, and better survival rates, in young RCC patients than in older ones (112141519242526). Sánchez-Ortiz et al. (12) compared the clinicopathological features and prognosis of 106, 14–40-year-old patients with those of 145, 58–61-year-old patients. These authors found that younger patients had unfavorable histological features and a higher incidence of lymph node metastasis at presentation than older patients, whereas they showed better disease-specific survival and RFS on multivariate analysis (12). Two recent large multicenter studies that included 93 and 288 young (≤ 40 years) RCC patients reported that age is an independent prognostic factor for CSS (114). In addition, despite differences in age cut-offs and study design, other studies also noted that age is an independent predictor of CSS (152425). Hakim et al. (27) postulated the underlying immunosenescence theory (progressive decline in immune function that develops with age), by which immunological alterations may account for poor survival in elderly RCC patients. This may explain the favorable histological features and better prognosis of the young age group. On the other hand, considering the unfavorable outcomes of elderly RCC patients, these patients might require more aggressive treatment and surveillance, or may be more likely to benefit from adjuvant therapy than patients with early onset RCC. Although our results were similar to those of previous studies in which RCC in young adults was more often localized and had a better prognosis than the disease in older patients (114), age was not an independent prognostic factor on multivariate analysis. This finding suggests that the favorable effect of age at diagnosis on prognosis is minimal and should not be regarded as a crucial determinant for the treatment of RCC.
Previous conflicting results may be partially explained by the small sample size or the heterogeneity of the study cohort. Current evidence of the prognostic impact of age in RCC is drawn from approximately 1,500–2,000 patients reported in the literature. To the best of our knowledge, the present study is the largest published series of young RCC patients, with the inclusion of 541 cases with early onset RCC. Detailed demographic and pathological information was available for most participating patients. Another notable finding of the present study was that patients younger than 40 years were less likely to have clear cell RCC and more likely to have translocations involving chromosome Xp11.2, which result in gene fusions involving the TFE3 (transcription factor E3) gene (28). Xp11 translocation RCC occurs predominantly in children and young adults, and accounts for approximately one-third of pediatric RCC cases (29). Although limited data are available to date, this type of RCC is believed to be rather indolent, associated with advanced stage at presentation, and associated with a poor prognosis (30). On the other hand, papillary and chromophobe RCC, which have a better outcome than conventional RCC or aggressive subtypes such as Bellini carcinomas, sarcomatoid differentiation, or nonclassified carcinomas, occur with the same frequency in the different age groups (114). Although the combined analysis of different histologic subtypes may have affected our results, the preliminary analysis did not show any differences in prognosis according to histologic subtype (data not shown). Further studies are needed to confirm whether the effect of age on prognosis differs according to histologic subtype.
Our study had several inherent weaknesses. The retrospective design of the study suggests the presence of sampling bias. Standardization of surgical techniques or practice guidelines such as adjuvant treatment and follow-up protocols was not possible because of the multi-institutional collaboration. The lack of a central pathology review may have introduced interobserver biases. Since this was a surgical series, older patients with comorbidities were not included; this could have introduced bias and our results may not be reflective of all patients with RCC. Despite these limitations, the present study is the largest population study of young RCC patients and is a nationwide multicenter study that provides a highly generalizable insight into age-specific pathological features and survival in patients with surgically-treated RCC.
In conclusion, young age at diagnosis was closely related to favorable pathologic features and prolonged CSS, although it was not an independent prognostic factor for survival in RCC. This finding suggests that the favorable effect of age at diagnosis on prognosis is minimal and should not be regarded as a crucial determinant for the treatment of RCC.
 XML Download
XML Download