

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Hand-foot syndrome (HFS) is a relatively frequent (7.3%–63%) dermatologic toxic reaction to certain anti-cancer chemotherapeutic agents (12). Patients with HFS usually present with a spectrum of symptoms ranging from burning, tingling, and skin erythema to pain, edema, and ulcerations in the extremities. The lesions can interfere considerably with even the simplest daily activities, such as walking or gripping objects (3). The drugs associated with HFS are not only chemotherapeutic agents (5-fluorouracil, pegylated liposomal doxorubicin, paclitaxel, docetaxel, doxorubicin, and capecitabine), but also emerging target therapies such as multikinase inhibitors (MKI; sorafenib, pazopanib, regorafenib, axitinib, and sunitinib) (4).
Most treatment recommendations for the management of HFS are based on case reports, case series, and personal experience rather than on the data from randomized controlled trials (5). One of the reasons for this is the lack of validated questionnaires for use in clinical trials to aid the early recognition of the symptoms, to assess the effectiveness of agents for the treatment of HFS within clinical studies, and to evaluate the impact of these treatments on HFS-associated patients’ health-related quality of life. In 2015, Anderson et al. (6) developed the hand-foot skin reaction and quality of life (HF-QoL) questionnaire, which simultaneously measured the extent of HFS symptoms and their effects on daily activities. However, the HF-QoL instrument has not yet been translated into the Korean language. Given the growing number of cancer patients and the resulting increase in the administration of chemotherapeutic agents, convenient and effective methods for measuring the symptoms and quality of life associated with HFS are required. Therefore, the aim of this study was to develop and validate the Korean version of this instrument (HF-QoL-K) in cancer patients.
MATERIALS AND Methods
Participants
The present study was performed at 4 institutions between August 2015 and March 2016 (Chonnam National University Hwasun Hospital, Hwasun; Kangbuk Samsung Hospital, Seoul; National Cancer Center, Goyang; Samsung Medical Center, Seoul, Korea). Participants were recruited from the Department of Obstetrics and Gynecology of each institution and were included consecutively.
The inclusion criteria were as follows: 1) patients were diagnosed with gynecologic cancers such as cervical, endometrial, uterine corpus, vulvar, vaginal, ovarian, fallopian, and primary peritoneal cancer; 2) patients receiving chemotherapy including 5-fluorouracil, pegylated liposomal doxorubicin, paclitaxel, docetaxel, and doxorubicin; 3) patients aged 18 years or older; and 4) patients able to speak and understand Korean. Patients who were not able to understand the questionnaire or refused to participate were thus excluded from the study. The institutional review boards of each participating institution approved the study, and all participants provided written informed consent.
Original HF-QoL questionnaire
The HF-QoL instrument comprised of a 20-item symptom domain and an 18-item daily activity domain (6). Each item was rated on a 5-point scale from 0 (not at all) to 4 (always or extremely). Therefore, the maximum possible score for HF-QoL was 152 points, with higher scores indicating worse quality of life or greater symptom burden.
Procedure
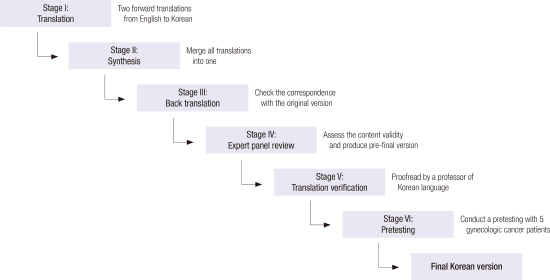
We obtained permission from Roger T. Anderson on September 4th, 2015 to use the questionnaire that he developed (6), and two forward translations from English to Korean were performed by two independent translators who spoke English as a first language and were fluent in the idioms and colloquial terms in Korean (Fig. 1). A meeting was convened between the translators and another person who was not involved in the translation procedures to obtain a unified Korean version of the two forward translations. Subsequently, an independent translator (a Korean-American with a medical degree) back translated the unified version of the questionnaire. The backward translations were then reviewed again by the two bilingual authors of this article. At the commencement of the present study, we organized a panel of five experts to assess the content validity for each item on the Korean version of the HF-QoL and confirmed that the internal validity index was ≥ 0.90. This pre-final version was proofread by a J.S. Kim (Professor of Korean language and literature at the Kyung Hee University) to check for spelling, grammar, and formatting mistakes. A pretesting of the Korean version of HF-QoL was performed on five gynecologic cancer patients with HFS, at the Kangbuk Samsung Hospital between September 2015 and October 2015. Any misunderstandings were not reported. Therefore, this version of the questionnaire was finalized.
 | Fig. 1The translation and the linguistic validation process (The six stages involved in the translation of the original English HF-QOL into Korean one).
|
The final version of the HF-QoL-K was presented to the participants using an interviewer-assisted self-report questionnaire at the hospital (Supplementary Fig. 1). In order to assess the test-retest reliability, the same questionnaire was given to the same patients after 3 weeks.
Data analysis
Because the required sample size for testing the reliability and validity of a measuring tool is generally 5 times the number of the items in the tool (7), the sample size calculated for the HF-QoL-K (38 items) was 190 subjects. When a 10% dropout rate was included in this calculation, the final sample size was determined to be 209 subjects.
All statistical analysis was performed using the SPSS software version 18.0 (SPSS Inc., Chicago, IL, USA) and STATA software version 13.1 (Stata, College Station, TX, USA) to test the validity and reliability of the HF-QoL-K. Qualitative data were presented as the frequency (percentage). In case of quantitative variables, after checking for the normality of the data, mean ± standard deviation and median (interquartile range [IQR]) were used to describe normal and non-normal distribution, respectively. The validity was assessed by the content validity, which was determined using the internal validity index. Reliability was assessed by the internal consistency reliability and test-retest reliability. Internal consistency reliability was determined using the Cronbach alpha coefficient. Test-retest reliability was determined using the intra-class correlation coefficient (ICC), the Bland-Altman plot, and scatter plot. All reported p values were two-sided, and P values < 0.05 were considered statistically significant.
Results
Patient characteristics
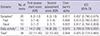
During the study period, 209 gynecologic cancer patients undergoing chemotherapy relating HFS, were invited to participate in the present study. After the exclusion of 15 patients who did not provide HF-QoL-K data at baseline or at 3 weeks, the final study population was 194 patients. The demographic and clinical characteristics of these 194 patients are listed in Table 1. The mean age and body mass index were 54.3 ± 9.7 years and 22.6 ± 3.0 kg/m2, respectively. While ovarian, fallopian, or peritoneal cancers constituted 75.8% (n = 147) of the study population, cervical and endometrial cancers constituted 11.9% (n = 23) and 10.8% (n = 21) of the population, respectively. Ninety-three (47.9%) patients were receiving primary adjuvant or neoadjuvant chemotherapy at the time of study, while 101 (52.1%) patients were receiving chemotherapy for recurrent cancer. Among the 194 patients, 68% of the patients were treated using chemotherapy that mainly included paclitaxel, whereas 22.2%, 3.6%, 3.1%, and 3.1% of the patients were treated with pegylated liposomal doxorubicin, doxorubicin, docetaxel, and 5-fluorouracil, respectively. At the time of study, only 68 (35.1%) patients received medications (gabapentin, pregabalin or duloxetine hydrochloride) for HFS.
Table 1
Demographic and clinical characteristics of the study population (n = 194)

SD = standard deviation, DM = diabetes mellitus, HFS = hand-foot syndrome, ECOG = Eastern Cooperative Oncology Group.
*This is a multiple choice question; †Other chemotherapy regimens included capecitabine and multikinase inhibitors (particularly sorafenib, pazopanib, regorafenib, axitinib and sunitinib); ‡The ECOG Performance Status Scale are widely used methods of assessing the functional status of cancer patients (16).
![]()
Validity and reliability of HF-QoL-K
The median total score for the HF-QoL-K was 22 (IQR, 11–40) at the first assessment (Table 2); the median score for symptom domain was 6 (IQR, 2–12), and the median score for daily activity domain was 14 (IQR, 7–28). The Cronbach alpha coefficient for consistency was 0.958 for the HF-QoL-K, suggesting a high internal consistency. The Cronbach alpha coefficients for the symptom domain, foot subdomain, hand subdomain, and daily activity domain of the HF-QoL-K were 0.911, 0.856, 0.822, and 0.970, respectively. The ICC for the test-retest analysis was 0.825 (95% confidence interval [CI], 0.774–0.865) for the HF-QoL-K, which suggested a strong correlation between the two. The ICC for the symptoms and daily activity domain were 0.789 (95% CI, 0.729–0.837) and 0.837 (95% CI, 0.790–0.875), respectively. The scatter plots of the linear association between the test and retest are shown in Fig. 2. The Pearson correlation coefficients for the scatter plots were high, ranging between 0.789 for the daily activity domain and 0.837 for the symptom domain. The Bland-Altman plots for measuring the agreement with the repeated measures are shown in Fig. 3. The mean difference between the test and the retest total scores was −1.180 (95% CI, −3.195–0.834); and the upper and lower limits were 27.274 and −29.634.
Table 2
The HF-QoL-K domain characteristics
Data are expressed as number, median (IQR) or median (95% CI), as appropriate.
HF-QoL-K = Korean version of the hand-foot skin reaction and quality of life, ICC = intra-class correlation coefficient, IQR = interquartile range, CI = confidence interval.
*Symptom domain consists of 20 items having a score range of 0–80. A higher score indicates more symptom burden; †Daily activity domain consists of 18 items having a score range of 0–72. A higher score indicates more disability; ‡The complete HF-QoL-K questionnaire consists of 38 items. The maximum score that can be achieved on HF-QoL-K is 152 points, with higher scores indicating more severe forms of the hand-foot syndrome.
![]()


Discussion
The aim of the present study was to produce the Korean version of the HF-QoL by translation and cultural modifications. Owing to the growing number of cancer patients (89) and the resulting increase in the administration of chemotherapeutic agents, developing or introducing a scale with HFS for the measurement of the symptoms and quality of life has become crucial. Therefore, the development and validation of the Korean version of the HF-QoL was required. In the present study, we confirmed that the Korean version of the questionnaire showed a similar reliability and validity to the original version of the HF-QoL.
HFS, referred to as hand-foot skin reaction, palmar-plantar erythrodysesthesia, chemotherapy-associated acral erythema, and the Burgdorf reaction, constitutes a spectrum of diseases with varying clinical appearances and pathogenesis (10). Two different types of HFS are found at either end of this spectrum, representing the extremities: chemotherapy-related HFS and MKI-related HFS (10). While chemotherapy-related HFS is more diffuse, MKI-related HFS is localized at the pressure points (5). Before the commencement of the drug regimen for any cancer therapy that is associated with HFS, the patient should be thoroughly informed on what to do in the event that symptoms of HFS appear. In patients with skin disease affecting the hands and feet, dermatological treatment is imperative. The only recommended management techniques for HFS are the discontinuation or dose modification of treatment (11). Cold compresses, application of emollients, topical corticosteroids or dimethylsulfoxide have been used, but with no definitive results (12). Oral or topical pyridoxine (vitamin B6) has been successful in some instances (13).
Although oncologists have evaluated on symptoms of HFS according to the National Cancer Institute-Common Terminology Criteria for Adverse Events (NCI-CTCAE) grading system (14), the NCI-CTCAE reports were made from the physician’s perspective and thus might not fully capture the patient’s HFS symptom burden. Before the commencement of this study, two validated questionnaires that measured the symptoms and quality of life of HFS were available (615). We chose to translate the HF-QoL questionnaire to the Korean language instead of translating the HFS-14. The reason for this was that the HFS-14 (15) solely assesses the functional implications of HFS, including pain, but not the wider symptom burden associated with the condition, while the HF-QoL assesses both. Moreover, the HF-QoL instrument could provide more information about the HFS to the clinician, as compared to the HFS-14, because the HF-QoL instrument had two distinct domains (symptom domain and daily activity domain) and two specific subdomains (foot subdomain and hand subdomain).
Compared to the original HF-QoL, few minor modifications were applied to HF-QoL-K during the translation process. First, a subdomain term was changed from “hands or fingers” to “hands.” Second, 18 items in the daily activity domain were not subclassified into specific subdomains for developing a more intuitive and concise questionnaire, although daily activity domain had four subdomains in the original HF-QoL. Third, the term “sensitive to pressure” in question 4 of the foot and hand domains was translated as “feel painful when touched” in Korean. Fourth, the term “fork” in question 10 of the daily activity domain was translated as “spoon and chopstick” in Korean, because the undertone of a given word can be quite different in different cultures. Lastly, the term “downhearted and sad” in question 17 of daily activity domain was translated as “tired and sad.” We believe that these modifications in the HF-QoL-K reflect the Korean culture and communication style used with the patients in Korea.
There were several limitations to the present study. First, the main limitation of this study is that it was only conducted in gynecologic cancer patients. Second, patients who were treated with MKIs were not included, because the therapeutic role of MKIs was not proved in gynecologic cancers. Therefore, further studies are required to determine the effectiveness of the HF-QoL-K instrument for the assessment of other conditions and therapies. Third, the correlation between patient-reported outcome (HF-QoL) and physician-rated outcome (NCI-CTCAE) was not assessed in this study. However, each scale demonstrated excellent measurement properties and discriminated between HF-QoL score and NCI-CTCAE grade with large effect sizes in the original version (English language) of the HF-QoL by Anderson et al. (6). Meanwhile, the strength of this study is that the questionnaire was translated with a rigorous procedure, which includes permission acquisition from the original developer, translation verification by a professor of Korean language, and pretesting before the start of the field-testing. The comprehensive and rigorous translation procedure ensured that the Korean version of HF-QoL was scientific and convincing.
In conclusion, the final Korean version of the HF-QoL showed adequate reliability and validity among Korean cancer patients with HFS. Therefore, this version will be a useful instrument in the clinical trials investigating chemotherapy-induced HFS and/or potential neuroprotective agents in Korean cancer patients. Further research is warranted to investigate the non-gynecologic cancer and chemotherapy regimens by using the HF-QoL-K.
 XML Download
XML Download