

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The liver is an organ that plays an important role in hemorheology (12). It is widely known that the liver synthesizes plasma proteins, lipids, and coagulation factors, and controls the cellular composition of the blood, all of which are important determinants of hemorheology (13). In chronic liver diseases (CLDs), liver function is adversely affected, leading to hemorheological alterations (14). Since the blood vessels in the liver including sinusoid are small, the altered hemorheology disturbs the microcirculation in the liver. Hence, it is not clear whether the altered hemorheology is the cause or the result of the damaged liver.
Blood viscosity is a physical property of blood, representing the thickness or stickiness of blood. It is defined as the ratio of shear stress to shear rate (5). The shear rate is determined by the ratio of flow velocity to lumen diameter. Blood viscosity is the inherent resistance of blood against the flow within blood vessels, and is affected by factors such as hematocrit (Hct), deformability and aggregability of red blood cell (RBC), plasma proteins (i.e., fibrinogen, globulins, albumin), lipids, and plasma viscosity (5678). Traditionally, a rotational cone-and-plate viscometer was used to measure blood viscosity, but this has not been widely used in clinical practice because of the risk of blood contamination and the need to calibrate the spring sensor. Recently, a new scanning capillary tube viscometer with disposable U-tubes is introduced, which measures blood viscosity over a wide range of shear rates (i.e., 1–1,000 1/s) (9101112).
A number of studies have reported the hemorheology in various liver diseases. In alcoholic liver cirrhosis (LC) patients, both whole blood viscosity (WBV) and plasma viscosity as well as Hct and fibrinogen concentration were significantly lower compared to the controls (1213). On the other hand, in patients with nonalcoholic fatty liver disease (NAFLD), WBV was significantly higher than those in the control group (114151617). In addition, the WBV and RBC aggregation index were significantly higher in hepatitis B patients than those in the control group (13).
Although the previous studies clearly reported that WBV in the NAFLD and hepatitis B was significantly higher than those in the control, whereas WBV in the LC was significantly lower than those in the control (121314151617), these studies did not investigate the effect of gender. Since the effect of gender on the WBV is one of the most important variables, it is not clear whether or not the conclusions from the previous studies are valid for both genders. Thus, we aimed to examine WBV in patents with CLDs including NAFLD, chronic viral hepatitis (CVH) B and C, and LC using an automated scanning capillary tube viscometer to identify any gender effect of WBV on the types of liver diseases.
MATERIALS AND METHODS
Study patients and collection of clinical data
A total of 425 patients who underwent assessment for WBV at the clinic of liver disease, Seoul St. Mary’s Hospital, Catholic University of Korea between July 2015 and May 2016 were included by retrospective manner (Fig. 1). Patients without the clinical data of rheological parameters, including unknown Hct, mean corpuscular volume, lipid profile, and prothrombin time were excluded (n = 134). Patients with hepatocellular carcinoma were also excluded (n = 143).
 | Fig. 1Classification of patients with chronic liver disease who underwent whole blood viscosity test according to clinical and radiological diagnosis.
WBV = whole blood viscosity, NAFLD = nonalcoholic fatty liver disease.
|
The baseline clinical history and laboratory data of the 148 patients from medical records review were obtained. The baseline characteristics included age, gender, and body mass index (BMI), as well as history of alcohol, smoking, diabetes, hypertension, and cardiovascular disease. Diagnosis of CLD was based on clinical and radiologic findings measured by ultrasonography or CT and classified into three categories; NAFLD was defined that there is evidence of hepatic steatosis by radiologic tests and there are no causes for secondary hepatic fat accumulation such as significant alcohol consumption or viral hepatitis (n = 63) (18), CVH was defined as irregular and coarse hepatic parenchymal echogenicity with hepatitis B surface antigen or antibody to hepatitis C virus positive (n = 50), and LC was defined as nodular and very coarse hepatic parenchymal echogenicity (n = 35). Liver stiffness was measured by transient elastography using FibroScan®, and expressed in kilopascals (kPa). All included patients underwent blood sampling in the stable, sitting position, and the blood was stored in sterile ethyl-enediaminetetraacetic acid (EDTA)-treated plastic tubes. Hct; hemoglobin (Hb); mean corpuscular volume (MCV); international normalized ration (INR); Platelet (PLT) count; total/high/low density cholesterol (TC/HDL/LDL); triglyceride (TG); and liver function tests, including serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), and total bilirubin were determined through blood tests.
Measuring whole blood viscosity
In addition to the baseline blood tests, we measured WBV by using the automated scanning capillary tube viscometer (Hemovister, Ubiosis, Seongnam, Korea) at a low shear rate (5s−1) and a high shear rate (300s−1), respectively (9). WBV at a low shear rate reflects hemodynamical status with very low velocity as in microcirculation, in which RBCs can aggregate and thus increase the flow resistance at blood vessels. WBV at a high shear rate reflects hemodynamical status with high velocity as in a large artery. Therefore, WBV at a low shear rate indicate blood viscosity at the diastolic status, and WBV at a high shear rate indicate blood viscosity at the systolic status. The reference intervals for WBV were 3.36–5.16 cP at 300 s−1 and 8.25–14.28 cP at 5s−1 as previously described (9). Detail theory and operating principle of the automated scanning capillary tube viscometer are given elsewhere (10).
Statistical analyses
All categorical factors were analyzed using the χ2 test, and the Fisher’s exact test. Continuous variables were analyzed using the Mann-Whitney U-test, or the analysis of variance (ANOVA) test. The linear regression analysis was used to identify correlation between the value of transient elastography and WBV. Statistical significance was defined as a P value < 0.05. SPSS version 19 software (SPSS Science, Chicago, II, USA) was used for all analyses.
RESULTS
Baseline characteristics according to the liver parenchymal status and gender
The baseline characteristics of patients with CLDs are summarized in Table 1. Among the 148 included patients, 63 patients had NAFLD, 50 patients had CVH, and 35 patients had LC. The 148 CLD patients were composed of 73 males and 75 females. Patients with LC tended to be older in age. Patients with NAFLD had higher BMI than patients without NAFLD. Patients with LC had lower levels of albumin, Hct and PLT, and higher INR than patients without LC.
Table 1
Baseline characteristics according to diagnosis

All values are expressed as mean (± standard deviation) or number (%).
HBV = hepatitis B virus, HCV = hepatitis C virus, NAFLD = non-alcoholic fatty liver disease, BMI = body mass index, HTN = hypertension, DM = diabetes mellitus, CVD = cardiovascular disease, TE = transient elastography, kPa = kilopascals, TB = total bilirubin, Alb = albumin, INR = international normalized ratio, Hb = hemoglobin, Hct = hematocrit, MCV = mean corpuscular volume, PLT = platelet, TG = triglyceride, TC = total cholesterol, AST = aspartate transaminase, ALT = alanine transaminase, GGT = gamma-glutamyl transpeptidase, Cr = creatinine, ESR = erythrocyte sedimentation rate, CRP = C-reactive protein.
![]()
Whole blood viscosity in patients with chronic liver disease
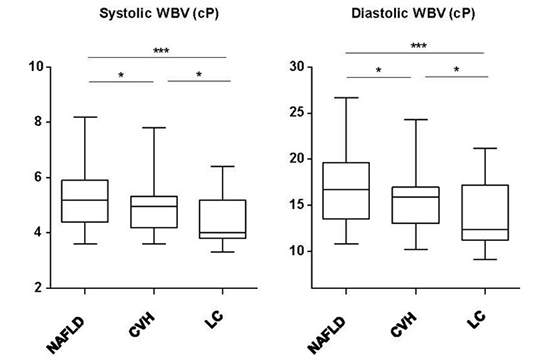
Next, we analyzed systolic and diastolic WBV according to the diagnosis and gender (Fig. 2). Systolic and diastolic WBV was significantly lower in total and male patients with LC than NAFLD and CVH. However, there were no statistically significant differences in systolic and diastolic WBV between liver diseases in female patients. Of note, systolic and diastolic WBV in patients with CLD enrolled in this study tended to be higher than those in healthy Koreans (systolic: median, 5.1 cP vs. 4.03 cP, diastolic: median, 15.8 cP vs. 10.63 cP) (9). These findings suggest that patients with CLD have higher blood viscosity than healthy controls, indicating the disturbance of microcirculation in liver; however, WBV decreases with progression of liver fibrosis. This change in blood viscosity was found to be affected by gender, which have distinct clinical and rheological characteristics. For example, in female patients, there was no significant difference in both systolic and diastolic WBVs among NAFLD, CVH, and LC. The significant difference in WBV between NAFLD/CVH and LC reported by all the previous studies (1291416171819) was only found in male patients, not in female patients in the present study.
 | Fig. 2Total (A), male (B) and female (C) systolic and diastolic whole blood viscosity according to diagnosis. The boxplots show systolic and diastolic whole blood viscosity are significantly lower in patients with liver cirrhosis than other patients. Median (range) values of total, male and female whole blood viscosity according to diagnosis; systolic and diastolic whole blood viscosity (D).
cP = centipoises, NAFLD = nonalcoholic fatty liver disease, CVH = chronic viral hepatitis, LC = liver cirrhosis, WBV = whole blood viscosity.
*P < 0.05, †P < 0.001.
|
Correlation between transient elastography and whole blood viscosity
The level of liver stiffness measured by transient elastography using FibroScan® became higher in patients with CLD along with the progression of the liver fibrosis (median, NAFLD: 5.6 kPa, CVH: 7.2 kPa, LC: 27.3 kPa). Using correlation analysis, we found that there was statistically significant, inverse correlations between both systolic and diastolic WBV and liver stiffness (Fig. 3).
 | Fig. 3Correlation between transient elastography and whole blood viscosity; systolic (A) and diastolic (B) whole blood viscosity. The linear regression analyses show that there are weak inverse correlation between liver stiffness and whole blood viscosity, both systolic and diastolic.
WBV = whole blood viscosity, cP = centipoises, kPa = kilopascals.
|
DISCUSSION
In this study, we found that the WBV was highest in NAFLD patients, and it was relatively low in LC patients particularly in male patients. WBV also observed to decrease in LC patients with more severe fibrosis. Among the three groups, patients with NAFLD had the highest blood viscosity, and this is consistent with the results of previous studies (1617192021). It is commonly known through many previous studies that increased blood viscosity is related to increased incidence and mortality of cardio-cerebrovascular disease (2223242526272829).
In this study, among the three different CLD, the LC group had the lowest values for WBV. In addition, WBV negatively correlated with transient elastography using FibroScan®, and decreased as fibrosis progressed. As White blood cell, RBC, Hct, PLT and albumin levels decrease in these patients, WBV is also expected to decrease (30). Liu et al. (31) reported that Hct levels and PLT count decreased in patients with advanced cirrhosis, and cirrhosis patients with esophageal variceal hemorrhage accompanied by shock had lower WBV values than patients who had hemorrhage without shock. Therefore, WBV values can be used to classify the severity of cirrhosis (32), and also to make a prognosis for esophageal hemorrhage.
In this study, men tended to have higher WBV values than women for all types of CLD, and this is consistent with results of previous studies (9333435). In a study by Jung et al. (9) involving 297 healthy Korean subjects, men showed higher WBV at all shear rates than women, and showed a significant difference in Hct levels. The big question is why both systolic and diastolic WBVs in LC are not significantly different from those in NAFLD/CVH in female patients. Conversely, one can ask why the WBVs in LC are significantly lower with the progression of liver disease than those in NAFLD/CVH in male patients. One can speculate that in male NAFLD/CVH patients, WBV is significantly elevated (Fig. 2B), leading to the disturbance of microcirculation such that the normal function of liver to generate plasma proteins and lipids is compromised. Subsequently, with the progression of disease to LC, the WBV significantly decreases. On the other hand, in female NAFLD/CVH patients, WBV is not significantly elevated (Fig. 2C), such that the normal function of liver is not compromised compared to male patients. Subsequently, with the progression of disease to LC, the WBV does not significantly decrease.
The limitations of this study are that the patient sample size was small, and it is retrospective study. In addition, since we did not measure the levels of plasma proteins, it was difficult to evaluate the impacts of these proteins on blood viscosity. Moreover, it was impossible to exclude bias since we did not include healthy controls in our study.
In conclusion, WBV values varied across the CLD patients depending on gender, the different types and etiologies of the disease. We suggest that a WBV test can become a useful tool for classifying CLD and determining the prognosis for different types of CLD particularly in male patients.
 XML Download
XML Download