

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Hepatitis A virus (HAV) infection is a self-limiting disease and asymptomatic in approximately 70% of children aged < 6 years, but it can result in a serious illness with risks of morbidity and mortality, particularly among susceptible older adults (12). HAV is transmitted primarily through person-to-person contact via the fecal-oral route or through the ingestion of contaminated food or water (23). Therefore, the incidence and prevalence of HAV infection are influenced by general hygiene and the socioeconomic status of countries (345). Hepatitis B virus (HBV) infection is transmitted perinatally from infected mothers to neonates in high prevalence areas such as sub-Saharan Africa and East Asia, while in low prevalence areas such as North America and Western Europe, sexual contact and unsafe injection are the major transmission modes (67). Since HBV infection can cause chronic disease and put people at high risk of death from cirrhosis and liver diseases, it is considered to be a major global health problem (67). Both HAV and HBV infections have decreased in incidence and prevalence with the improvement of socioeconomic status, sanitation, and use of effective vaccines worldwide (8). Although vaccination strategy and policy are variable among countries, vaccinations against HAV and HBV infection are recommended before travel to an endemic area (91011)
In addition, immunoglobulin G (IgG) therapy is used for susceptible people to prevent HAV and HBV infections both following exposure to HAV and HBV, and before traveling to an area of endemic infection (12). Moreover, IgG replacement therapy and post-exposure IgG treatment are important for patients with primary antibody deficiency (PAD), who can only obtain antibodies against various microorganisms by IgG replacement therapy because they have a defect in the production of antibodies in response to natural antigens or vaccination (1314). Currently, both intravenous IgG (IVIG) and subcutaneous IgG (SCIG) are available, but IVIG therapy is more common than SCIG therapy (15). IVIG is usually recommended at a dose of 400–600 mg/kg every 3 or 4 weeks, and it is considered that an IgG level greater than 500 mg/dL might reduce infection and improve clinical outcomes in patients with PAD (161718).
Because IVIG is manufactured from pooled plasma, both the concentration of total IgG and that of specific antibodies in IVIG products vary depending on the immune status of blood donors. Since the incidence of HAV and HBV infections and vaccination strategy differ among regions or countries, the proportions of antibodies against HAV and HBV in IVIG products are variable (192021). The proportions of antibodies against HAV and HBV can also vary within the same region among plasma samples collected at different times.
However, until now, few studies have analyzed the concentrations of antibodies against HAV or HBV in commercially available IVIG products (1322). Therefore, this study was performed to evaluate and compare the titers of specific antibodies against HAV and HBV in commercial IVIG products from several countries.
MATERIALS AND METHODS
Commercial intravenous immunoglobulin G (IVIG) preparations
Nineteen lots of IVIG products from five manufacturers in three countries were analyzed in this study. Ten lots (product A) and six lots (product B) of IVIG products were obtained from two manufacturers in Korea, one lot was prepared from each of two manufacturers in Japan (product C and product D), and one lot was prepared in the USA (product E). Products A, B, and E were treated with cold ethanol solvent/detergent and products C and D were treated with polyethylene glycol for the purification of IVIGs. All IVIG products contained 50 mg/mL IgG. Products A, B, and D, which were formulated as liquids, were divided into 1.5 mL aliquots. Products C and E were formulated as lyophilizates, and they were divided into 0.5 mL and 1.5 mL aliquots, respectively, after dissolving the lyophilizates with water for injection according to each manufacturer’s protocol. All aliquots were stored at −80°C until use.
Analysis of the titers of antibodies against HAV and HBV
The anti-HAV antibody titers of all IVIG preparations were determined by electro-chemiluminescence immunoassay using an Elecsys Anti-HAV II kit and a Cobas 8000 e602 analyzer (Roche Diagnostics, Mannheim, Germany). Anti-hepatitis B surface (anti-HBs) antibody titers were measured by chemiluminescent microparticle immunoassay using an ARCHITECT Anti-HBs Reagent Kit and an ARCHITECT i400 immunoassay analyzer (Abbott Laboratories, Lake Bluff, IL, USA). These experiments were performed by Seegene Medical Foundation (Seoul, Korea). The lower limits of detection for anti-HAV and anti-HBs antibodies were 3 mIU/mL and 10 mIU/mL, respectively, in this assay system.
Estimated trough titers of specific antibodies against HAV and HBV in the recipients’ serum
The estimated trough titers of specific antibodies against HAV and HBV in the recipients’ serum were calculated using the following formula, assuming that 400 mg/kg of IVIG is infused to patients with PAD (23).
Estimated trough titer of specific antibody = 0.5 × 0.4 × 0.2 × antibody titer
The factor 0.4 assumes the presence of 40 mL/kg plasma and 40% immunoglobulin in the intravascular compartment and that these numbers are at equilibrium.
Here, we briefly explain the components of this equation. The estimated trough value of each specific antibody = 0.5 × level at equilibrium, which assumes that the half-life of each IVIG preparation is 22 days and that the trough level would be reached at 26–27 days after the last infusion. In addition, the level at equilibrium = 0.4 × the peak value after intravenous infusion, where the peak value = N/[(40 mL plasma/kg) × patient mass in kg] = [(8 mL/kg) × antibody titer]/[(40 mL plasma/kg) × patient mass in kg] = 0.2 × antibody titer because N is the total dose infused into patient (400 mg/kg of IVIG preparation) and the concentration of each IVIG preparation examined in this study is 50 mg/mL.
Statistical analysis
Geometric mean titers (GMTs) and two-sided 95% confidence intervals (CIs) of anti-HAV antibody and anti-HBs antibody were calculated for products A and B since the number of lots of each IVIG products from other countries (i.e., products C, D, and E) was too small to perform statistical analyses. Statistical analyses were performed using IBM SPSS Statistics v23 software (IBM Software, Armonk, NY, USA). Calculations of P values were performed using the Mann-Whitney U test to compare the GMTs of antibodies between products A and B.
RESULTS
Titers of antibodies against HAV and HBV in commercial IVIG products
Anti-HAV antibody titers in IVIG products ranged from 1,888 mIU/mL (product C) to 8,927 mIU/mL (product A). The GMTs of anti-HAV antibody in products A and B were 5,667 mIU/mL (95% CI, 4,489–7,154) and 5,814 mIU/mL (95% CI, 5,143–6,572), respectively, and there was no significant difference between the anti-HAV antibody titers of products A and B.
Anti-HBs antibody titers ranged from 123 mIU/mL (product D) to 1,945 mIU/mL (product E). The GMTs of anti-HBs antibody in products A and B were 686 mIU/mL (95% CI, 562–838) and 506 mIU/mL (95% CI, 480–533), respectively. The GMT of anti-HBs antibody in product A was statistically higher than that in product B (P < 0.05) (Table 1).
Table 1
Concentrations of anti-HAV and anti-HBs antibodies in 19 lots of IVIG products from Korea, Japan, and the USA

HAV = hepatitis A virus, HBs = hepatitis B surface, GMT = geometric mean titer, CI = confidence interval.
![]()
Estimated trough titers of specific antibodies against HAV and HBV in the recipients’ serum
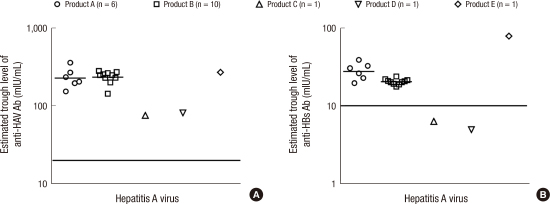
Estimated trough titers of anti-HAV antibody ranged from 76 mIU/mL (product C) to 357 mIU/mL (product A). All IVIG products exceeded the minimal protective level, 20 mIU/mL, assuming that IVIG was infused to patients with PAD at the dose of 400 mg/kg, which is the recommended dose.
Estimated trough titers of anti-HBs antibody in products A, B, and E exceeded the minimal protective level, 10 mIU/mL, assuming that IVIG was infused to patients with PAD at the dose of 400 mg/kg. However, estimated trough titers of anti-HBs antibody in products C (6 mIU/mL) and D (5 mIU/mL) did not reach the minimal protective level (Fig. 1).
 | Fig. 1Expected trough levels of anti-hepatitis A virus (HAV) antibody (A) and anti-hepatitis B surface (HBs) antibody (B) in various intravenous immunoglobulin G (IVIG) products, assuming an infusion dose of 400 mg/kg. Short bars indicate the geometric mean and long bars indicate the minimum protective concentrations of anti-HAV and anti-HBs antibodies (20 mIU/mL and 10 mIU/mL, respectively). Numbers in brackets indicate different lot numbers of the same product.
|
DISCUSSION
This is the first comprehensive study to evaluate and compare the concentrations of antibodies against HAV and HBV in commercial IVIG products from Korea and other countries. Most of the IVIG products in this study contained sufficient antibodies against HAV and HBV to protect PAD patients from HAV and HBV infections through IVIG replacement therapy.
Commercial IVIG products are produced from a pool of plasma samples collected from 10,000–40,000 donors and contain millions of different IgGs (24). The constituent pathogen-specific antibodies in IVIG may vary according to the cumulative exposure to the infections and vaccination status of the donor population. The IVIG products in this study were manufactured by Korean, Japanese, and USA companies using plasma collected from their respective local populations.
The incidence of HAV infection has declined in Korea, Japan, and the USA. Consequently, the seroprevalence of anti-HAV antibodies has recently been reported to be low among people under the age of 40 years in these countries (125262728293031). However, unlike the situation in Japan, the seroprevalence of anti-HAV antibodies has increased in children under the age of 10 years in Korea and the USA following the recommendation of vaccination against HAV for all children over the age of 12 months (12628). As we expected, titers of anti-HAV antibody in IVIG products prepared in Korea and the USA were higher than those in IVIG products from Japan. However, the estimated trough titers of anti-HAV exceeded the minimal protective level, 20 mIU/mL, in all IVIG products regardless of their country of origin. Thus, all IVIG products studied herein were found to have sufficient antibodies against HAV to protect patients with PAD from HAV infections at the current recommended dose.
However, the titers of anti-HAV antibody we measured in IVIG products were lower than those reported in previous studies, which were performed with IVIG products derived from the EU, USA, and Taiwan (2232). These findings support that interval monitoring of specific antibody levels in various IVIG products is required for the establishment of appropriate guidelines for treatment.
The concentrations of anti-HBs antibody in various IVIG products varied according to the countries of origin of the products. IVIG products from the USA showed the highest level of anti-HBs antibody, in agreement with the findings of previous studies (3233). The concentrations of anti-HBs antibody in products from Korea were lower than those reported by previous studies (3233). However, IVIG products from Korea and the USA contained a sufficient concentration of anti-HBs antibodies exceeding the minimal protective level, 10 mIU/mL, assuming that 400 mg/kg IVIG was infused to patients with PAD. In contrast, titers of anti-HBs antibody in the products derived from Japan were lower than those in the products from the USA and Korea, and the expected trough titers of anti-HBs antibody in the products from Japan did not reach the minimal protective value. These differences may be caused by many reasons, potentially including the different national immunization strategy used in Japan compared with that used in Korea and the USA. Whereas Korea and the USA have recommended routine vaccination against HBV for all infants since 1991, Japan started routine vaccination against HBV for all infants in 2014 (34). As a consequence, the seroprevalences of anti-HBs antibody in Korea and the USA were 63%–72.9% and 19.5%–60.5%, respectively, depending on the age group (2935363738). In contrast, the prevalence rate of anti-HBs antibody was only 5.1% in Japan (2935363738). Thus, IVIG products prepared from Japan showed relatively low concentrations of anti-HBs antibody.
The variation in the concentrations of specific antibodies against HAV and HBV in the IVIG products evaluated in this study may also reflect the natural occurrence of various infections, immunogenicity of vaccines, and other factors in each country where the products were manufactured. HAV infection is strongly related to socioeconomic indicators since it is transmitted primarily person-to-person contact via the fecal-oral route or ingestion of contaminated food or water. HBV infection is transmitted through contact with infected blood or semen and perinatal transmission from infected mothers to neonate. Since the incidence of these two infections tends to be dramatically lower in many developed countries including Korea when compared with less economically developed countries, the titers of antibodies against both HAV and HBV induced by vaccination will decline gradually after vaccination without the natural booster response. Therefore, continuous monitoring of the titers of specific antibodies in various immunoglobulin products should be performed to facilitate the judicious use of IVIG in PAD patients.
This study has some limitations. First, the number of included IVIG product lots from Japan and the USA was too small to draw any definitive conclusion. Second, antibody titers against HAV and HBV were examined in IVIG products and trough levels in the serum of patients with PAD receiving IVIG were estimated. It is commonly understood that the half-life of IVIG is about 23 days, but the actual average half-lives of commercial IVIG products vary from 20–41 days among the different products, and this variability causes differences among the products in the trough levels of plasma IgG following injection (39). However, to our knowledge, there have been no previous studies to evaluate the half-life or pharmacokinetics of specific antibodies against HAV and HBV. In addition, there have been no studies to report the protective levels of specific antibodies against HAV and HBV in patients with PAD. In this study, we considered the protective levels of antibodies to HAV and HBV to be the same as those reported for immunocompetent people. Thus, further studies are needed to examine a larger number of IVIG products prepared from various regions by different manufacturing processes (32) and test antibodies after treatment directly in the recipient patients’ serum. In addition, more studies are necessary to demonstrate the half-lives of available IVIG products and evaluate whether a correlation exists between the incidence of HAV and HBV infections in a given geographic region and the concentrations of antibodies against HAV and HBV in the IVIG products produced in that area. Finally, this study did not deal with intramuscular immunoglobulin (IMIG) or hepatitis B immunoglobulin (HBIG), which are frequently recommended as post-exposure prophylaxis. However, IVIG is preferred to IMIG or HBIG in subjects with a bleeding tendency or many types of immune deficiency (33). Further studies may be needed to analyze IMIG and HBIG products as well as the serum of patients treated with IMIG or HBIG.
In conclusion, most of the commercial IVIG products evaluated in this study contained a sufficient amount of antibodies against HAV and HBV to protect patients with PAD receiving IVIG treatment. These findings indicated that the concentration of antibodies in IVIG products can vary depending on the environment, socioeconomic status, and vaccination strategy in the country where the products are manufactured. Therefore, regular monitoring of the concentrations of antibodies against specific microorganisms in commercial IVIG products is needed to guide appropriate clinical implementations and treatment policy.
 XML Download
XML Download