

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Anatomical severity of coronary lesions is associated with adverse outcomes (123). The fractional flow reserve (FFR) has emerged as the reference tool for the assessment of functional severity of coronary lesions. It is significance in the treatment of coronary artery disease (CAD) has recently been underscored by the observation that coronary revascularization according to lesion functional significance is associated with improved long-term clinical outcomes (4567). However, there have been limited comparative data on clinical outcomes among deferred coronary lesions according to the functional severity. In addition, clinical factors that are associated with adverse clinical outcomes after deferred lesions using FFR have not been well elucidated. It may be important to identify the prognosis of deferred lesions considering that the use of FFR is increasing in daily clinical practice. This study therefore aimed to 1) evaluate the 3-year clinical outcomes of deferred lesions according to functional severity; and 2) define the factors which affect adverse outcomes in deferred lesions.
MATERIALS AND METHODS
Study design and population
Among 1,294 patients and 1,628 lesions in Korean FFR registry (ClinicalTrials.gov ID: NCT01409577) that was performed between July 7, 2003 and October 2011, 665 patients with 781 deferred coronary lesions without revascularization were included in this study. All enrolled coronary lesions were deferred after performing successful FFR measurement in at least one de novo lesion located at major epicardial vessels. In brief, Korean FFR registry was a multicenter registry designed to investigate FFR-guided percutaneous coronary intervention (PCI) outcomes. The patients who had at least one de novo lesion located in major epicardial coronary arteries in which FFR could be successfully measured were enrolled in Korean FFR registry. Patients with planned or previous coronary artery bypass surgery (CABG), cardiomyopathies, balloon angioplasty only, and congenital coronary anomaly were excluded. Previous results of Korean FFR registry demonstrated that drug-eluting stents implantation against FFR could not improve outcomes, and medical treatment for a functionally significant stenosis increased the risk of a delayed event (8). For the present study, participants were consecutively categorized on the basis of FFR in the following manner; ≥ 0.96 (group 1, reference group; n = 56), 0.86–0.95 (group 2, deferred group; n = 330), 0.81–0.85 (group 3, borderline deferred group; n = 170), and ≤ 0.80 (group 4, ischemic group; n = 99). The composite of groups 1–3 was defined as the non-ischemic group. If patient had multiple deferred lesions, patient was included in the group according to the worst FFR values of coronary lesion considering the objective of this study. The study protocol was approved by the ethics committee at each participating center.
Procedural details
Coronary angiography was performed using standard techniques. Antiplatelet and antithrombotic agents were prescribed according to current PCI guidelines (9). Angiographic images were acquired after intracoronary administration of 100 to 200 μg of nitroglycerin. FFR was measured using a 0.014-inch pressure guide wire (PressureWire, St. Jude Medical, St. Paul, MN, USA; ComboWire, Volcano Corporation, San Diego, CA, USA) as previously described and defined as the ratio between mean distal coronary pressure and mean aortic pressure, both measured simultaneously at maximal hyperemia (10). Hyperemia was induced with an intracoronary bolus administration (80 μg in left coronary artery, 40 μg in right coronary artery), intracoronary (240 μg/min) or intravenous continuous infusion (140 μg/kg/min) of adenosine (111213).
Quantitative coronary angiography
Quantitative coronary angiography (QCA) was performed by independent core laboratories at Seoul National University Cardiovascular Center and Ajou University Cardiovascular Center. QCA was performed by experienced observers, who were blinded to the FFR value and clinical data. Using the guiding catheter for calibration and an edge detection system (CAAS 5.7 QCA system, Pie Medical, Maastricht, the Netherlands), the reference diameters, minimal lumen diameter and lesion length were measured and the percent diameter stenosis was calculated. Lesion location was determined according to the American Heart Association classification (14).
Clinical outcomes
Follow-up data were obtained from a web-based reporting system. Additional information was obtained from hospital records and telephone contact, if needed. An independent study monitor verified all information on electronic case report forms. Primary endpoint was major adverse cardiac events (MACE) which was defined as the composite of all-cause death, myocardial infarction (MI), and target vessel revascularization (TVR). All death was considered cardiac unless there was a clear non-cardiac cause. Revascularization was defined as ischemia-driven if there was stenosis of at least 50% of the diameter and documented ischemia by a positive functional study, ischemic changes on an electrocardiogram, ischemic symptoms or FFR, or if there was stenosis of at least 70% as assessed by QCA in the absence of documented ischemia. MI was defined as an elevated cardiac enzyme with ischemic symptoms or new pathologic Q waves on electrocardiogram (15). Peri-procedural MI was not included. All clinical events were adjudicated by a clinical events committee in a blind fashion using original source documents and angiographic images.
Statistical analysis
Continuous variables are expressed as mean ± standard deviation (SD) and were compared using 1-way analysis of variance (ANOVA). Categorical data are presented as frequency (%) and were compared using the Pearson χ2 test or the Fisher exact test, as appropriate. The times to event data are presented as Kaplan-Meier estimates and the comparisons between groups were performed using log-rank test. To find the determinants for the primary endpoint, univariate and multivariate Cox regression analyses were performed in this study. Variables with P < 0.05 in the univariate analysis were entered into multivariate analysis. Statistical analyses were performed using SPSS version 18.0 for Windows (SPSS Inc., Chicago, IL, USA) and SAS 9.2 version (SAS Institute, Cary, NC, USA), and a P value of < 0.05 was considered statistically significant. All P values and confidence intervals are 2-sided.
RESULTS
Patient and angiographic characteristics
Baseline characteristics of the 655 participants are presented in Table 1. There were no significant differences in clinical characteristics such as age, left ventricular ejection fraction (LVEF), and the incidence of diabetes mellitus (DM), smoking, dyslipidemia, acute coronary syndrome (ACS), and previous history of MI or PCI among all groups. However, the incidence of multivessel disease was significantly different in each FFR group. Angiographic characteristics of 781 coronary lesions according to FFR are presented in Table 2. The deferred vessel was significantly different in each FFR group, with left anterior descending coronary artery (LAD) lesion being more frequent in the lower FFR group. QCA results of the deferred coronary lesions such as reference vessel diameter, minimal luminal diameter (MLD), % diameter stenosis (DS), and lesion length were also significantly different among these groups.
Table 1
Patient characteristics according to FFR group
Values are presented as mean ± standard deviation (SD) or number (%).
FFR = fractional flow reserve, ACS = acute coronary syndrome, MI = myocardial infarction, PCI = percutaneous coronary intervention, VD = vessel disease, LVEF = left ventricle ejection fraction, CCB = calcium Channel blocker, ACE = angiotensin converting enzyme.
![]()
Table 2
Angiographic characteristics according to FFR group

Values are presented as mean ± standard deviation (SD) or number (%).
FFR = fractional flow reserve, LAD = left anterior descending coronary artery, QCA = quantitative coronary angiography, MLD = minimal luminal diameter, DS = diameter stenosis.
![]()
Clinical outcomes according to FFR groups
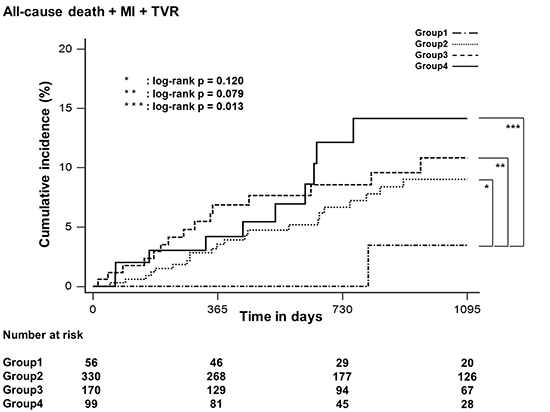
During 3-year follow-up, the overall rate of MACE was 8.2%. The rate of MACE in groups 1–4 was 1.8%, 7.6%, 8.8%, and 13.1%, respectively. The rate of individual MACE according to FFR groups was presented in Supplementary Table 1. In Kaplan-Meier survival analysis, the cumulative rate of MACE was not different in group 2 (log-rank P = 0.120) and group 3 (log-rank P = 0.079) compared with group 1. However, group 4 had significantly higher cumulative rate of MACE compared with group 1 (log-rank P = 0.013) (Fig. 1A). Compared with group 1, the risk of MACE was numerically higher without statistical significance in both group 2 (hazard ratio [HR], 4.46; 95% confidence interval [CI], 0.60–32.90; P = 0.143) and group 3 (HR, 5.13; 95% CI, 0.68–38.89; P = 0.113). However, the risk of MACE in group 4 was significantly higher than that in group 1 (HR, 8.18; 95% CI, 1.07–62.53; P = 0.043) (Supplementary Table 2). The cumulative rate of MACE was significantly higher in group 4 than in non-ischemic group (log-rank P = 0.040) (Fig. 1B). In landmark analysis, there was no difference in the cumulative rate of MACE during 1-year follow-up (log-rank P = 0.248). However, the cumulative rate of MACE was significantly different in each FFR group after 1 year, with group 4 having the highest cumulative incidence of MACE between 1- and 3-year follow-up (log-rank P = 0.020) (Fig. 2).
 | Fig. 1Time-to-event curve for 3-year MACE. Comparison of the event of MACE based on (A) normal FFR and (B) FFR < 0.80.
MACE = major adverse cardiac events, FFR = fractional flow reserve, MI = myocardial infarction, TVR = target vessel revascularization.
*log-rank P = 0.120; †log-rank P = 0.079; ‡log-rank P = 0.013; §log-rank P = 0.040.
|

Independent determinants for the primary endpoint in all participants
Univariate and multivariate Cox hazard regression analyses were performed to identify independent determinants for MACE among all participants. In the univariate Cox hazard regression analysis, diabetes mellitus (HR, 1.95; 95% CI, 1.14–3.34; P = 0.016), previous MI (HR, 2.35; 95% CI, 1.11–4.99; P = 0.026), previous PCI (HR, 2.13; 95% CI, 1.22–3.72; P = 0.008), ACS (HR, 2.04; 95% CI, 1.16–3.60; P = 0.014), LVEF (HR, 0.96; 95% CI, 0.93–0.99; P = 0.008), multivessel disease (HR, 2.31; 95% CI, 1.28–4.15; P = 0.005), LAD (HR, 0.51; 95% CI, 0.30–0.88; P = 0.015), %DS (HR, 1.03; 95% CI, 1.00–1.05; P = 0.020), and FFR (HR, 0.95; 95% CI, 0.92–0.98; P = 0.001) were significantly associated with MACE. Multivariate Cox hazard regression analysis revealed that only FFR (HR, 0.95; 95% CI, 0.92–0.99; P = 0.005) was independently associated with the risk of MACE (Table 3).
Table 3
Cox regression analyses to determine independent predictors for 3-year MACE
MACE, major adverse cardiac events, FFR = fractional flow reserve, HR = hazard ratio, CI = confidence interval, MI = myocardial infarction, PCI = percutaneous coronary intervention, ACS = acute coronary syndrome, LVEF = left ventricle ejection fraction, VD = vessel disease, LAD = left anterior descending coronary artery, DS = diameter stenosis, MLD = minimal luminal diameter.
![]()
Independent determinants for the primary endpoint among participants with FFR > 0.8
In univariate Cox hazard regression analysis, previous MI (HR, 2.56; 95% CI, 1.08–6.08; P = 0.034), previous PCI (HR, 2.64; 95% CI, 1.41–4.94; P = 0.002), ACS (HR, 2.46; 95% CI, 1.31–4.61; P = 0.005), LVEF (HR, 0.96; 95% CI, 0.93–0.99; P = 0.006), multivessel disease (HR, 2.25; 95% CI, 1.16–4.34; P = 0.016), and LAD (HR, 0.45; 95% CI, 0.24–0.84; P = 0.012) were significantly associated with MACE. However, FFR was not significantly associated with MACE (HR, 0.96; 95% CI, 0.90–1.02; P = 0.188). Multivariate Cox hazard regression analysis revealed that previous PCI (HR, 2.37; 95% CI, 1.13–5.01; P = 0.023) and ACS (HR, 2.35; 95% CI, 1.18–4.65; P = 0.015) were independently associated with increased risk of MACE (Table 3).
DISCUSSION
The major findings in the present study are that 1) the prognosis of deferred lesions without ischemia was favorable, consistent with previous investigations; 2) subjects with borderline FFR of 0.81–0.85 have similar incidence of MACE compared with those with usual deferred lesions as FFR 0.85–0.96, and deferring PCI therefore might be reasonable; 3) despite significant differences in angiographic parameters in each FFR group, these parameters could not predict MACE, and only FFR was independently associated with MACE among all subjects with deferred lesions; and 4) both angiographic parameters and FFR were not independent predictors for MACE among subjects with non-ischemic deferred lesions, and only clinical presentation and history of revascularization were strongly associated with the risk of MACE in these subjects.
Parameters assessing anatomical lesion severity such as DS, lesion length, plaque eccentricity, angle, and calcification may be related to both procedural complexity and prognosis of the indicated lesion. However, it is manifest that coronary lesion prognosis differs according to the presence of ischemia (16). Therefore, the need to overcome the limitations of angiography in assessment of lesion severity led to evaluation of functional significance of coronary stenosis, for which FFR has been regarded as a reference invasive physiologic tool (10). Recently, several studies consistently have reported the favorable results of PCI using FFR in clinical practice. In the Deferral Versus Performance of PTCA in Patients Without Documented Ischemia (DEFER) study, clinical outcomes after deferral of PCI of an intermediate coronary stenosis based on FFR ≥ 0.75 were excellent during 5-year follow-up (4). Tonino et al. (5) also reported that the routine measurement of FFR significantly reduced the rate of a composite clinical outcome of death, non-fatal MI, and revascularization in patients with multivessel coronary disease who were treated with DES in the Fractional Flow Reserve versus Angiography for Multivessel Evaluation (FAME) 1 study. Furthermore, FFR-guided PCI accompanied by optimal medical therapy decreased the need for urgent revascularization compared to optimal medical therapy alone in stable patients with functionally significant coronary lesion according to the FAME 2 study (7). Considering the results of these studies, the treatment of coronary lesions using FFR assessment may guarantee better clinical outcomes. However, there is a paucity of data on the prognosis of deferred lesions according to functional severity. In addition, data on the independent determinants of adverse clinical outcomes in patients with deferred lesions have been limited. In the present study, the long-term prognosis of subjects with ischemic coronary lesions was significantly worse than that of patients with non-ischemic coronary lesions after deferring PCI. Furthermore, considering that the rate of 3-year MACE was not significantly different relative to usual deferred lesions as FFR 0.86–0.95, deferring PCI with medical therapy may be safe in subjects with borderline FFR (0.81–0.85) value, which is an important finding.
According to the Providing Regional Observations to Study Predictors of Events in the Coronary Tree (PROSPECT) study, non-culprit lesions that were anatomically more significant were responsible for adverse clinical outcomes in patients with ACS (2). In the latter study, anatomically severe and functionally significant non-culprit lesions might be an important cause of adverse clinical outcome, however, the functional severity of those lesions was no evaluated. Interestingly, none of the angiographic parameters predicted MACE and only FFR was independently associated with MACE among all subjects with ischemic and non-ischemic deferred lesions in the present study. In contrast, FFR did not independently predict 3-year MACE among subjects with only non-ischemic deferred lesions. Clinical presentation as ACS and history of revascularization were more important clinical factors which were strongly associated with 3-year MACE among these subjects.
The rate of adverse clinical outcomes was not significantly different according to functional severity among subjects with non-ischemic deferred lesions despite significant different anatomical severity. There can be several explanations: 1) FFR grade may not be exactly the same as coronary plaque burden and could be affected by not only plaque burden but also various factors such as angle, vessel remodeling, and underlying macro- and microvascular structure, among others; 2) anatomical or physiologic severity itself may not be an unique player for future event occurrence in functionally insignificant coronary lesions; and 3) optimal medical therapy may play an important role in preventing plaque rupture in various amount of plaque volume. Based on the previous results that the benefits of stenting in functionally insignificant coronary lesions are not greater than those of optimal medical therapy, an alternative to the “no plaque, no event” concept is the hypothesis of “no ischemia, no benefit of stent” (45). If the purpose of coronary revascularization is an improvement in coronary flow, stenting in coronary lesion without flow limitation may not improve outcomes. Although vulnerable plaque is a substantial issue in the treatment of CAD, there remain no data supporting the efficacy of stenting in vulnerable plaque without flow limitation.
Although reference group of FFR ≥ 0.96 was considered to represent normal coronary artery, all deferred lesions enrolled in this study had at least mild angiographic stenosis, which is explicitly different from normal coronary artery. Also, it may be difficult to directly apply the previous prerequisite of “no plaque, no event” in the present study. Statistically insignificant but numerically higher event rate in deferred groups 2 and 3 compared to reference group 1 could be understood on the extension of specific patient population in current study. The results of current landmark analysis, namely that the rate of MACE was not obviously different according to FFR grade after deferring PCI within 1-year follow-up despite the significant difference observed between 1 and 3 years of follow-up, raised the important issues that 1) borderline deferred lesions can be progressively stabilized, consistent with previous studies emphasizing the importance of optimal medical therapy in patients with stable CAD (17); 2) however, the deferral of revascularization in ischemic coronary lesions should be avoided even with optimal medical therapy in order to achieve favorable clinical outcomes based on the results of recent meta-analysis (18).
Several studies have reported the clinical outcomes of deferred lesions focused on the FFR of 0.75–0.80 that has been considered as gray-zone for the deferral of coronary revascularization in clinical practice (1920). However, these studies were limited by their small number of participants which might contribute to somewhat different results. Although several studies with larger sample size evaluated the clinical outcomes of deferred lesions (2122), these studies mainly focused on the risk of revascularization in deferred lesions according to functional severity. The present study identified the safety of deferring revascularization in patients with coronary lesions with borderline FFR values. Additionally, this study identified different independent predictors for MACE in deferred lesions according to ischemia status. Considering the largest number of our participants compared with those of previous studies which evaluated the similar issue, this study might be able to provide a confirmative evidence for the safety of deferred lesions with borderline-zone of FFR.
The present study has some limitations. First, sample size of this registry and limited numbers of major adverse events may be insufficient to reveal clinical outcome of each group of lesion severity. Second, our registry data cannot be free from selection bias. However, all patients were enrolled consecutively during study period from each center. Third, adenosine infusion method for achieving maximal coronary hyperemia was not coherent in the present study. However, previous study confirmed that both intracoronary and intravenous adenosine induced maximal hyperemia might be suitable to assess FFR (11). Fourth, this study did not evaluate the vulnerability of coronary plaques. Concomitant invasive coronary imaging study would have provided more information on the clinical value of vulnerable plaque in coronary lesions without functional significance. Finally, the relatively low use of statin and the paucity of data on anti-anginal medication might be limitation in the present study. Despite the limitations of the present study, it is unique in that we identified the independent determinants for adverse clinical outcomes in patients with deferred coronary lesions according to ischemia and functional severity. Further prospective studies with larger sample sizes and longer follow-up are required to address these issues.
In conclusion, clinical outcomes of subjects with non-ischemic deferred lesions by FFR were acceptable, and the prognosis of these lesions was not significantly different according to the functional severity. No angiographic parameters predicted the development of MACE but only FFR independently associated with MACE among all patients with deferred lesions. However, previous history of PCI and presentation as ACS, but not FFR, were more important clinical factors which were independently associated with the increased risk of MACE in subjects with non-ischemic deferred lesions.
 XML Download
XML Download