

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Varicella is an acute contagious disease caused by the varicella-zoster virus (VZV). A live attenuated varicella vaccine was first developed in 1974 and is now used widely in many countries including the United States, Germany, China, Taiwan, and Republic of Korea (12345). In a recent meta-analysis of global varicella vaccine effectiveness, varicella vaccine was reported to be effective in preventing varicella (6). In specific, the United States where a universal two-dose varicella vaccination program was adopted since 2006 experienced declines in the incidence of the disease, the hospitalization of infected patients, and disease outbreaks (7).
In Korea, the varicella vaccination has been recommended for children in high-risk groups since 1988. Following the introduction of universal varicella vaccination by the National Immunization Program (NIP) in 2005, one-dose varicella vaccine has been recommended for all children aged 12–15 months. Four live attenuated varicella vaccines are available; three are based on the Oka strain, and one is based on the MAV strain. However, the incidence of varicella has yet to decline and, in fact, has been continuously rising, from 22.5 per 100,000 persons in 2006 to 73.2 in 2013 (8).
The objective of this study was to evaluate the effectiveness of one-dose varicella vaccination program in Korea by performing a matched case-control on children in Seoul.
MATERIALS AND METHODS
We performed a matched case-control study on children who were younger than 12 years of age in Seoul, Korea. Relevant data were collected from the National Notifiable Disease Surveillance System (NNDSS). The NNDSS, which was established in 2001, consists of case-based national infectious disease data collected via a surveillance system; nationally notifiable diseases such as varicella must be reported by all local public health centers in the country. The varicella case data in the NNDSS include demographic and clinical details such as patient name, date of birth, gender, address, date of disease onset, laboratory confirmation, and vaccination status.
All cases were children with varicella identified in Seoul between January 2013 and December 2013. Cases were composed of confirmed and possible cases and we only use the former to avoid misclassification bias. We excluded cases born prior to universal varicella vaccination adopted in 2004 or after 2012, because varicella vaccination is recommended for children aged 12–15 months. In order to estimate the exact effectiveness of varicella vaccine, we also excluded subjects who developed varicella within 42 days after vaccination (the so-called “wild-type” varicella) and who were vaccinated twice.
We aimed at selecting controls to represent the source population from which varicella cases arose. From the same NNDSS data, mumps and scarlet fever were considered appropriate as controls for the following reasons; 1) mumps and scarlet fever are infectious diseases independent of varicella, 2) age distribution in incidence of mumps or scarlet fever is similar to that of varicella.
In recruiting age-matched controls who had suffered from mumps or scarlet fever but had no history of varicella were identified in Seoul between January 2013 and December 2013 in the same NNDSS population where cases were reported. We matched each control by date of birth to a 1-month interval centered on the birth date of each case; a single control was randomly chosen if more than one candidate seemed appropriate. Ultimately, we created a list of 1:1 individually matched controls.
The effectiveness of a vaccine was estimated as follows; we calculated vaccine effectiveness by substituting the matched overall risk (OR) for the relative risk (RR) (1 – RR); this approximates the RR in a case-control study (9).
Statistical analysis
The χ2 test was used to compare the groups in terms of categorical variables, and the paired t-test was used to compare them with regard to continuous variables. To estimate the effectiveness of one-dose vaccination, we performed conditional logistic regression analysis on the 1:1 matched pairs after adjusting for the effects of possible confounders such as sex and age at vaccination; we then calculated matched odds ratios with 95% confidence intervals (CIs). When calculating the effect of time since vaccination, we used conditional logistic models with dummy-coded variables (10). A two-sided P value < 0.05 was considered statistically significant. All data were analyzed with the aid of SAS software, version 9.3 (SAS Institute, Inc., Cary, NC, USA).
RESULTS
Subjects
In 2013, a total of 3,622 cases were reported. Of the 3,622, we excluded 2,807 possible varicella cases. Of the remaining 815 cases, we also excluded 278 cases; 230 had been born before June 2004, 27 had been infected within 12 months of birth, 5 had wild-type varicella, 16 had received two doses of vaccine (Fig. 1). Finally, we included 537 varicella cases in the study.
Characteristics of cases and controls
The 537 cases and their individually matched controls were similar in terms of both age and gender. The proportions of vaccinated cases and controls were similar, at 407 (75.8%) and 419 (78.0%), respectively (Table 1).
Table 1
Characteristics of children with varicella and matched controls

Number of who received varicella vaccine at age younger than 12 months was 5 in controls.
MMR = measles-mumps-rubella.
![]()
Of those who were vaccinated, 379/407 (93.1%) cases and 366/419 (87.4%) controls were vaccinated before 15 months of age, as recommended by the national vaccination policy. The proportion of cases vaccinated was significantly higher than the proportion of controls vaccinated (P < 0.002).
More than half of all vaccinated cases (241/407; 59.2%) and 227/419 (54.2%) of the controls received vaccine A; the proportions of the other vaccines used were as follows: Unknown (20.4% of cases and 19.1% of controls) > vaccine B (13.0% and 10.0%, respectively) > vaccine C (5.9% and 11.7%, respectively) > vaccine D (1.5% and 5%, respectively). However, the proportions of the vaccines used were significantly different between the groups (P = 0.001). Thus, both age at vaccination and type of vaccination were entered into the conditional logistic model.
Effectiveness of varicella vaccination
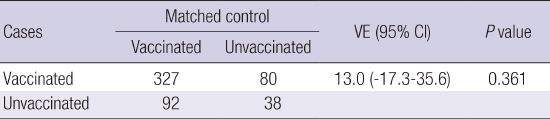
According to the conditional logistic regression analysis of the data for matched pairs, the overall effectiveness of one-dose varicella vaccination was 13% (95% CI, −17.3–35.6). The unadjusted estimate of vaccine effectiveness was 11.8% (95% CI, −17.1–33.6, P = 0.385) (Table 2).
Table 2
Overall effectiveness of varicella vaccine
| Cases | Matched control | VE (95% CI) | P value | |
|---|---|---|---|---|
| Vaccinated | Unvaccinated | |||
| Vaccinated | 327 | 80 | 13.0 (−17.3–35.6) | 0.361 |
| Unvaccinated | 92 | 38 | ||
When unadjusted for matched pairs, vaccine’s effectiveness (= 1 − OR) was 11.8% (−17.1%–33.6%, P = 0.385).
VE = vaccine effectiveness (= 1 − matched OR), CI = confidence interval, OR = overall risk.
![]()
Conditional logistic regression analysis of vaccine effectiveness by each of the four vaccine manufacturers showed that the effectiveness of different vaccines varied (Table 3). Only vaccine C exhibited statistically significant effectiveness (88.9%; 95% CI, 52.1–97.4). The vaccine effectiveness were −5% (95% CI, −61.9–31.9) for vaccine A, −100% (95% CI, −700–50.1) for vaccine B, 71.4% (95% CI, −37.5–94.1) for vaccine D, and −16.7% (95% CI, −101–32.4) for the vaccine of an unknown manufacturer.
Table 3
Effectiveness of varicella vaccine by manufacturers
![]()
Overall, the effectiveness of a one-dose varicella vaccination was 75.8% (95% CI, 22.8–92.4) in the first year after vaccination. Thereafter, effectiveness decreased, falling to zero (or below) in the fourth and the sixth years. When adjusted for sex, age at vaccination and measles-mumps-rubella (MMR) vaccination within 28 days of birth, the effectiveness of varicella vaccine was not significant even in the first year after vaccination (Table 4).
Table 4
Overall effectiveness of varicella vaccination by time since vaccination

VE = vaccine effectiveness, CI = confidence interval, MMR = measles-mumps-rubella.
*Results are adjusted for sex, MMR vaccination within 28 days, age at vaccination.
![]()
DISCUSSION
The results of this study show that the overall effectiveness of one-dose varicella vaccination in preventing confirmed cases of varicella was low and insignificant (13%; 95% CI, −17.3–35.6). Specifically, the vaccine effectiveness of vaccine A, which was used in more than half of all vaccinations, was −5% (95% CI, −61.9–31.9), whereas vaccine C was highly effective (88.9%; 95% CI, −52.1–97.4). Vaccination was effective for only 1 year (the estimate of 75.8% fell to 67.1% after adjustment for confounders).
These results are consistent with those of a recent clinical case-control study assessing the effectiveness of an MAV strain-based varicella vaccine in Korea (11). The estimated effectiveness was statistically insignificant (54%; 95% CI, −0.10–2.05) and the vaccine may not have alleviated clinical symptoms. In contrast, studies in other countries have shown that single-dose varicella vaccination was highly effective in terms of both reducing the prevalence of varicella and alleviating the symptom severity (31213141516). Oka strain-based varicella vaccines have been 87% effective in the United States (13, 17), 86% effective in Germany (12), and 84% effective in China (3). In other studies, varicella vaccination remained quite effective over time, although some waning was evident after the first year (13). However, vaccine effectiveness then rebounded and persistent immunity was evident in some studies.
In Korea, more than half of all vaccinees were immunized with vaccine A, derived from an MAV/06 strain of varicella isolated from a 33-month-old Korean boy in 1989 (1819). An immunogenicity study and a prelicensing safety study (192021) showed that the strain was highly immunogenic and safe, with a post-vaccination geometric mean titer (GMT) of 173.7 and seroconversion rate of 100%. However, two clinical trials (2223) and a recent clinical case-control study (11) showed that the vaccine did not ameliorate disease severity and was poorly immunogenic. A recent immunogenicity study on MAV and Oka (Vari-L) vaccine showed that the MAV vaccine generated higher seropositivity rates and antibody titers than the Oka vaccine and provided immunity against VZV, despite waning of immunity observed (24). Not all Oka vaccine in this study, however, were effective against VZV, so it cannot directly be interpreted that MAV vaccine is effective.
The age at vaccination may also affect effectiveness, and our cases and controls differed significantly in this regard. In the United States, children vaccinated at younger than 15 months were at increased risk of breakthrough infection of varicella (13). The proportion of children vaccinated at ages younger than 15 months was higher in the case group. Nevertheless, when we entered age at vaccination in our conditional model, using a dummy variable for time, age was not significant.
This study had several limitations. Selection bias may have been operating when we created our list of controls. The proportions of cases and controls who received MMR vaccinations differed, as it was lower in cases (81.9%) than in controls (97.6%). However, as Korea operates a universal health insurance system and as MMR vaccination is included in that system, the difference between cases and controls is unlikely to have introduced any substantial bias. Second, the severity of disease was not recorded. To assess vaccine effectiveness, it is appropriate to ask if the vaccine alleviates severity of symptoms aspects of disease, such as fever, rash, and number of lesions. Again, we lacked such data. However, this is the first community-based matched case-control study on cases confirmed both epidemiologically and in the laboratory who underwent one-dose varicella vaccination in Korea.
In conclusion, the one-dose varicella vaccination program did not clearly protect against varicella. Therefore, it is necessary to further investigate why we had reduced effectiveness of varicella vaccine in Korea
 XML Download
XML Download