

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dengue fever (DF) is a mosquito-borne disease caused by dengue virus (DENV), belonging to the genus Flavivirus. DF has become global public health concerns. The dengue infection has spread dramatically around the world in recent decades. The infection is seen as endemic in more than 100 countries and about 50% of the world’s population is at risk of DF (1). A recent study indicated an estimated 390 million dengue infections occur per year, of which 96 million appeared to have clinical manifestation (2). Among the countries with DF, Southeast Asia and the Western Pacific countries are known to be the most endemic regions (2).
Any autochthonous case of DF has not been confirmed yet in Korea, imported DF was first reported in 2001 and the cases have increased continuously thereafter (3). Most cases were caused by travelers returning from Southeast Asia, including Philippines, Indonesia, Malaysia and Thailand. As Korean travelers visiting Southeast Asia have increased during recent years, there was an increased trend in annual imported dengue cases.
DENV is known to be transmitted between people by the mosquitoes, particularly Aedes aegypti and Aedes albopictus. Aedes aegypti, known as the primary vector of dengue and zika viruses, is not detected but Aedes albopictus is commonly found in Korea. Aedes albopictus is known to be a secondary vector of DENV and play a limited role for transmission (4). However, over-dispersed abundance of Aedes albopictus may be a risk factor of DF outbreak in Korea.
Secondary infection with a different DENV serotype (DENV-1 to 5) from primary infection has been known as a major risk factor for the development of severe dengue, formerly known as dengue hemorrhagic fever (DHF)/dengue shock syndrome (DSS) (56). Secondary infection with different serotype may elicit antibody-dependent enhancement (ADE) response, which facilitates infection of Fc-receptor-bearing cells with DENV and amplified production of cytokines (78). These responses were reported to be linked to severe symptom and increased mortality (910). DHF or DSS have been not reported yet in Korea. However, increasing travel to dengue-endemic regions and accumulation of infected people with residual antibody may predispose Korean travelers to severe dengue by repetitive infection.
Previous studies in Europe, Australia, and Japan reported various dengue cases imported from endemic regions (111213). The study analyzed the relationship between the number of dengue cases imported into each region and the number of travelers arriving from dengue-affected areas, using national dengue importation data from web resources and surveillance reports. The study in Europe reported that travelers arriving from dengue-endemic regions affect dengue importation into Europe and the risk of dengue importation was greatest in August, September, and October (11). For Japan, most of dengue cases were imported from Southeast Asia and the trend in dengue infection among Japanese travelers was associated with seasonal fluctuation of DF incidence in Southeast Asia (12). The study in Australia also reported that imported DF was caused by infected travelers returning from Southeast Asia (13). These studies provided spatio-temporal elements affecting dengue importation into each country and suggested effective public health responses.
In this study, we analyzed epidemiological characteristics for imported dengue infection in Korea by using national surveillance data and reports. We suggest the potential risks of dengue transmission by continuous importation and the effective responses to minimize dengue infection.
MATERIALS AND METHODS
Data collection
This study analyzed national surveillance data on the annual number of reported dengue cases from 2006 to 2015. Data for the Philippines and Lao People’s Democratic Republic (Lao PDR) were collected from World Health Organization (WHO) Western Pacific Region (14). Data for Thailand are collected from Department of Disease Control, Ministry of Health, Thailand (15). For Malaysia and Singapore, data were obtained from WHO Western Pacific Region and Ministry of Health (14161718). Data for Taiwan were collected from Centers for Disease Control, Taiwan (19). For Japan, the number of reported dengue cases was collected from National Institute of Infectious Diseases, Japan (20).
Data of DENV serotypes for Malaysia, Thailand, Singapore and Vietnam were collected from previously published reports (17212223). Each study group used national epidemiological data and provided partial data on the serotype distribution for the period 2002–2014.
For Korea, data on imported dengue cases were provided by Korea Centers for Disease Control and Prevention (KCDC) (3). Monthly data from 2011 to 2015 were summed and used to analyze seasonal trend in the imported dengue cases. KCDC reported the number of male and female cases by age group. The aggregated data from 2011 to 2015 were used to determine risk groups by gender and age distributions. To analyze distribution of Korean travelers, Korean departure statistics from Korea Tourism Organization were used (2425).
Statistical analysis
To determine risk group by age and gender, the χ2 test were used to compare the observed proportion of males and females among reported dengue cases to the expected proportion based on data from Korean departure statistics.
The incidence of imported DF among Korean travelers returning from Southeast Asia was compared between high-incidence period (July–November) and low-incidence period (December–June). This comparison was calculated as a relative risk (RR) and associated 95% confidence intervals (CI). Statistical analysis was performed using GraphPad Prism (GraphPad Software, La Jolla, CA, USA). A P value of < 0.05 was deemed to be statistically significant.
GLOBAL PREVALENCE
DF has rapidly spread in all regions in recent decades. WHO reported the number of cases reported increased from 2.2 million in 2010 to 3.2 million in 2015 (1). Increased global traveling of people and international trade contributed to transmit DENV from endemic regions to other countries (26). Furthermore, global climate changes such as warming facilitated spread of dengue-infected mosquitoes and transmission of virus (27).
Recent study reported that 70% of DENV infections occurred in Asia (2). The number of DF cases in Asia has rapidly increased (Fig. 1). For Philippines, 200,415 dengue cases were reported in 2015. The Philippines showed increase in DF of about 65% compared to 2014. Furthermore, the number of cases reported in August 2016 is 15.8% higher than that reported during the same period in 2015 (14). A study reported clinically diagnosed dengue cases in the Philippines were associated with a direct cost of $345 million per year (28). The trend of dengue incidence in Malaysia has continued to increase since 2001 until 2015 (16). The dengue incidence rate (cases per 100,000 populations) was 72 in 2001 and progressively increased to 396 in 2015. For Thailand, 144,952 dengue cases and 141 deaths were reported in 2015 (15). The number of cases in 2015 was about 200% higher than in 2014. More than 136,000 cases of dengue were reported in August 2016 and is the highest number of cases in over 20 years (14). The incidence of DF in Taiwan has risen sharply in recent years. A significant rise in the number of dengue cases was reported especially in 2015 (19). Singapore has seen fewer dengue cases in 2015, compared to 2014. However, the cumulative number of cases in August 2016 (n = 10,095) was almost doubled as compared to that reported in the same period of 2015 (n = 5,447) (14). For Indonesia, the government reported 112,511 DF cases and 871 fatalities in 2013 (29). In 2015, the reported cases of dengue fever doubled those of 2014 in the Jambi, Indonesia (30). A recent study reported that the DHF incidence increased rapidly but the case fatality ratio of DHF decreased considerably in recent decades (31). However, it was difficult to perform comprehensive analysis for dengue epidemiology because precise surveillance data of DF cases were not available for Indonesia.
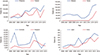 | Fig. 1Number of dengue cases reported in Asian countries, 2006–2015.
Increasing trends in annual dengue cases were shown in Asian countries (Philippines, Thailand, Malaysia, Cambodia, Taiwan, Singapore, Japan, and Korea). Note that each graph displays data with different scales on the number of reported cases. Data for dengue cases in each country were collected from World Health Organization (WHO) and national surveillance reports, as described in Materials and Methods (31416171819).
|
Notably, periodical epidemic cycles at 2–5 year intervals were identified in Thailand, Cambodia and Singapore. Previous studies also reported that Southeast Asian countries with high dengue incidence have the cycles of epidemics occurring every 3 to 5 years (2132). These epidemiologic dynamics were known to be associated with the changes in herd immunity and genetic diversity of DENV (3233). Japan showed increasing dengue cases over recent years. Most of dengue cases are detected among travelers returning from endemic regions. However, 162 autochthonous cases were reported in 2014 and there is an ongoing concern for potential dengue outbreaks in Japan (20).
Dengue outbreaks and transmission have been frequently reported in all regions of Africa (343536). Recent reports suggest that DF is endemic in 34 African countries (Table 1) (3435). Of these countries, 22 have reported outbreaks of local transmission of DENV. Twelve other countries in Africa reported DF cases only in travelers, returning from dengue-affected areas (34). Aedes aegypti, the primary vector for dengue, is known to be resident in all but five countries (Western Sahara, Morocco, Algeria, Tunisia, and Libya) (34). Although dengue outbreaks in Africa are not well characterized owing to the absence of reliable surveillance system and underrecognition of DF, the presence of disease and high prevalence of antibody to dengue virus suggest that dengue infection is endemic in all regions of Africa. All four DENV serotypes (DENV-1 to 4) have been detected in Africa and DENV-2 appeared to cause the most epidemics (34). Until recently, severe dengue had been reported infrequently in Africa (37). Previous studies showed decreased susceptibility to severe disease among the black population and suggested race may be host resistance factor to severe dengue (3839). These genetic factors may be associated with low incidence of DHF/DSS in Africa. Furthermore, because over 70% of febrile illnesses are treated as presumptive malaria in Africa, DF cases might be underreported or misdiagnosed as malaria (40).
Table 1
African countries reporting dengue transmission*

*Data for 34 African countries are collected from previously published study (34).
![]()
IMPORTED CASES IN KOREA
Any autochthonous dengue case has not been confirmed yet in Korea, but imported dengue cases have been increased since 2001. Imported DF cases have been caused by the travelers returning from various dengue-affected regions such as Southeast Asia, Africa, and Latin America (Table 2). The accumulated data from 2011 to 2015 show most of DF cases were imported from Southeast Asia (Fig. 2A) (3). The largest number of DF cases in Korea was imported from the Philippines (n = 339, 38.0%), and followed by Thailand (n = 122, 13.7%), Indonesia (n = 98, 11.0%), and Cambodia (n = 65, 7.3%). The number of imported cases per 1,000,000 travelers showed that the incidence of imported dengue was the highest in travelers visiting to Indonesia (69.8 cases per 1,000,000 travelers), not the Philippines (60.1 cases per 1,000,000 travelers) (Fig. 2B). Notably, although the number of visitors to the Philippines is similar to that of visitors to Thailand, more cases were imported from the Philippines. Furthermore, the incidences of dengue from Cambodia and Malaysia were similar to that from Thailand. Because the number of Korean travelers visiting to these countries has been increased in recent years, it is expected that the importation of DENV will increase continuously (Fig. 3) (24). Collectively, these data showed that Korean travelers to dengue-endemic countries of Southeast Asia have higher risk for dengue infection, and the risk of dengue importation may be closely associated with local dengue incidence of visited region. Therefore, we suggest travelers planning to Southeast Asia should be aware of regional dengue situation and take necessary precautions to avoid DENV infection.
Table 2
Imported dengue cases in Korea*

*Data for imported dengue cases were collected from Korea Centers for Disease Control and Prevention (KCDC) (3).
![]()
 | Fig. 2Number of imported dengue cases in Korea, 2011–2015.
(A) The number of dengue cases imported from Southeast Asian countries. (B) The number of imported cases per 1,000,000 travelers. Most of reported dengue cases in Korea were imported from Southeast Asian countries. Data for dengue cases from 2011 to 2015 were provided by Korea Centers for Disease Control and Prevention (KCDC) (324).
|
 | Fig. 3Number of Korean visitors to dengue-endemic countries in Southeast Asia, 2011–2015.
The number of Korean travelers visiting to Southeast Asia has been increased during 2011–2015. Data for Korean travelers were provided by Korea Tourism Organization (24).
|
DF is caused by five antigenically distinct serotypes of DENV (41). Primary infection may be asymptomatic or result in a mild febrile illness without lasting complications. However, secondary infection with a different dengue serotype may causes DHF or DSS, which is characterized by coagulopathy, organ impairment, plasma leaking, and severe bleeding that may progress to hypovolemic shock (2). Such severe dengue disease is mediated by ADE response, which facilitates infection of Fc-receptor-bearing cells with DENV-antibody immune complexes and virus replication (42). The rates of severe dengue in each of the Southeast Asian countries vary as they have different incidences of dengue (Fig. 4). For Thailand, approximately 50% of total dengue patients were registered to have severe dengue disease. Because passive surveillance system is main source of reported data, mild cases of DF may be not reported in Thailand. The countries with relatively low incidence of dengue, such as Taiwan and Singapore, showed severe dengue rates of less than 1%. In Korea, national surveillance system has not reported the incidence of severe dengue, but clinical case study reported a few cases of severe dengue (4344).
 | Fig. 4Reported dengue cases and the rate of severe dengue in Southeast Asian countries, 2001–2015.
The number of dengue cases and the rate of DHF/DSS (%) reported in Southeast Asian countries (Thailand, Malaysia, Taiwan, and Singapore). Note that each graph displays data with different scales on the number of reported cases. Data for Thailand (2006–2015), Malaysia (2001–2010), Taiwan (2006–2015) and Singapore (2010–2015) were collected from national surveillance reports and previously published studies (15171819).
DHF = dengue hemorrhagic fever, DSS = dengue shock syndrome.
|
Previous reports showed that dominant serotype of DENV in each country had changed continuously (Fig. 5) (17212345). For Thailand, DENV-1 and 4 were dominant in 2005, and DENV-1 had kept the highest proportion from 2006 to 2009. In 2010, DENV-2 was a dominant serotype (21). For Malaysia, DENV-1 was dominant in 2005, and DENV-2 became a dominant serotype in 2007 and 2009. In 2008 and 2010, DENV-1, 2, and 3 showed similar distribution. A dynamic change was also detected in monthly distribution of virus serotypes (17). Furthermore, regional data in Malaysia showed a heterogenous distribution of virus serotypes in different states (17). In endemic countries, dengue incidence has an interannual periodicity of epidemic cycles at 3–5 year intervals (32). The epidemic cycle was often linked to change in DENV serotypes or genotype (3233). These data indicate repeated travel to dengue-endemic region raises a possibility of infection with different serotype virus and risk for severe dengue. Especially people infected in the past should avoid unnecessary revisit to endemic countries to prevent secondary infection. In Korea, serotyping data of the patient have not been provided yet. To reduce severe dengue by secondary infection with different serotypes, determination of previously infected virus serotypes is helpful. The data for serotype distribution will be also useful for understanding epidemiological trends of imported dengue and preventing severe dengue.
 | Fig. 5Changes in serotype distribution of dengue virus reported in Southeast Asian countries, 2002–2012.
|
In Korea, the number of imported dengue cases showed seasonal patterns (Fig. 6) (3). The aggregated monthly data from 2011 to 2015 showed that importation of DF was most common during August through November (RR = 2.60; 95% CI, 2.26–2.99). The largest number of dengue cases was imported in August (163 of 893, 18.3%). In 2014 and 2015, there were two peaks in imported dengue cases in July–September and October–December. These periods are relevant to the rainy season with high incidence of dengue in most Southeast Asian countries. For Philippines, peak infection rates were shown during the rainy season, between May and November (14). In 2015, more cases were reported and highest incidence of dengue was shown during June through December. For Thailand, peak transmission occurs in the rainy season, between June and September, all across the country (21). In 2015, two infection peaks were shown between June and December. Cambodia also show highest infection rates during the rainy season from May to November, and infection risk may be increased in urban areas (14). For Indonesia, dengue infection is elevated during the rainy season from November to April but year-round transmission occurs (46). For Malaysia, the periods with high infection rates differ regionally (October–February in east peninsular Malaysia; July–August in west peninsular Malaysia) (1747). Collectively, dengue outbreak in Southeast Asian countries follows seasonal patterns. The seasonality of dengue affects not only internal outbreak but also importation of DF into non-endemic region. Because seasonal pattern of dengue incidence showed region-specific peaks, travelers visiting to dengue-endemic countries need to be aware of regional prevalence and seasonal dengue incidence. In addition, Korean travelers visiting to Southeast Asia should be aware of dengue infection not only in summer but also winter season.
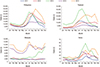 | Fig. 6Number of monthly dengue cases in Asian countries, 2011–2015.
The seasonal patterns of dengue cases were shown in Asian countries (Philippines, Thailand, Malaysia, and Korea). Note that each graph displays data with different scales on the number of reported cases. Data for dengue cases in each country were collected from World Health Organization (WHO) and national surveillance reports, as described in Materials and Methods (3141516).
|
In dengue-endemic regions, DF was known to occur predominantly in children (214849). Most cases of dengue in the Philippines were reported in children aged 5–14 years (Fig. 7) (48). Similar pattern was shown in Thailand. The highest rates of dengue in Thailand were reported in individuals aged 5–14 years, followed by those aged 15–24 years (21). Furthermore, previous study reported more cases of severe dengue by secondary infection were examined in individuals aged between 5 and 14 years compared with those aged 15 years or older (50). However, dengue patients aged 20–49 years accounted for 75.2% of total imported cases in Korea (P < 0.001). Similarly, dengue cases aged 20–39 years occupied about 60% of total imported cases in Japan (51). Such distribution is different from those in dengue-endemic countries. The pattern among Koreans may be associated with the highest rate of travel abroad in the 20–49 year old age group (60.7% of total overseas travelers) (25).
 | Fig. 7Number of reported dengue cases by age groups in Asian countries.
Age distribution of dengue cases in endemic countries (Philippines and Thailand) and non-endemic countries (Korea and Japan). Note that each graph displays data with different scales on the number of reported cases and age distribution. Data for Philippines (2009), Thailand (2010) and Japan (2006–2014) were collected from national surveillance reports and previously published studies (3214851).
|
The aggregated data from 2011 to 2015 showed that males were found predominantly among imported dengue cases in Korea (P < 0.001) (Fig. 8A) (3). Specially, infected males (n = 411) were 1.5 times more than females (n = 261) in the 20–49 year age group. Similarly, more dengue cases were reported for males than for women in Korea and Japan during 2006–2010 (51). A previous study also showed that there was a predominance of males with DENV infection in six Asian countries (Lao PDR, Philippines, Singapore, Sri Lanka, Cambodia, and Malaysia) (52). The report demonstrated an excess of males was detected among reported dengue patients over 15 years of age in dengue-endemic countries.
 | Fig. 8Number of imported dengue cases by age and gender groups in Korea. 2011–2015.
(A) The accumulated number of dengue cases from 2011 to 2015, stratified by age and gender. (B) Age and gender distribution of dengue cases per 1,000,000 travelers. Data for Korea (2011–2015) are provided by Korea Centers for Disease Control and Prevention (KCDC) (325).
*P < 0.001 analyzed by χ2 test, comparing the observed proportion of males and females among reported dengue cases to the expected proportion based on the number of travelers.
|
With consideration of the number of travelers by age and gender, age distribution of dengue cases per 1,000,000 travelers shows that the incidence of imported dengue was the highest in males aged 20–29 years (Fig. 8B). Notably, although dengue cases aged 30–49 years occupied higher proportion of total cases due to frequent travel, the incidence of dengue in group aged 30–49 years was shown to be similar to that in group aged 10–19 years. These data indicate all age groups except 20–29 year old males have a similar risk for dengue infection. Different age distribution of DENV infection between Southeast Asia and Korea may come from the different status of herd immunity. Koreans were not exposed to DENV and susceptible to DENV in any age group, while repeated infection in Southeast Asia may form the immunity to DENV through the juvenile period (2153).
The reasons for male predominance are not clear, but it is supposed that gender-related biological factors or behavior may affect the male predominance in dengue infection (49). Collectively, males aged 20–29 years, having frequent visit to endemic regions and outdoor activities, are considered the highest risk group for imported DF in Korea. Considering the age and gender distribution of travelers, all age groups need to be aware of dengue infection when traveling to endemic areas.
DISCUSSION
Cases of DF have increased in Southeast Asia over recent decades. Increased dengue viral infection in Southeast Asia also affects the incidence of dengue in non-endemic area. Recent studies reported climate change may facilitate dengue outbreaks in endemic areas (2754). Global warming enhanced spread of dengue vectors and transmission of virus (27). Numbers of months with average temperature higher than 18°C per year were found to be associated with increasing incidence of DF in Taiwan (54). In addition, urbanization affected the propagation of dengue fever throughout the world (5556). Rapid urbanization in Southeast Asia brings a higher population density and makes it easier for infected mosquito to transmit dengue virus (56). Increase in population density and movement by urbanization contribute to rapid spread of DF.
To reduce the burden of dengue, WHO global strategies for dengue prevention have focused on five technical elements: 1) early diagnosis and case management, 2) integrated surveillance and outbreak preparedness, 3) sustainable vector control, 4) future vaccine implementation, and 5) basic operational and implementation research (57). WHO suggests international collaboration for integrated vector management and development of effective control measures. Furthermore, WHO indicates early diagnosis of dengue cases is crucial for determining clinical outcome, and emphasizes early notification for initiating an early response against dengue outbreaks.
In Korea, DF has been included in a legally designated infectious disease since 2000. Surveillance and detection for dengue infection is performed by KCDC. Suspected cases in local hospitals are reported to KCDC, and then KCDC performs serological and molecular test to confirm dengue infection. Because DF is not endemic in Korea, the government does not perform active surveillance but focuses on early diagnosis, education and information for dengue prevention in recent years (3).
Among people infected with DENV, asymptomatic cases are more frequent than symptomatic cases. About 75% of all dengue infections are known to be clinically inapparent or mild symptomatic cases (2). A recent study reported asymptomatic people can be infectious to competent mosquitoes despite their lower level of viremia (5859). Moreover, it was reported that people with asymptomatic dengue infection can spread DENV to non-endemic area by nosocomial transmissions such as transfusion, organ transplantation, and needle stick injury (606162).
In Korea, national surveillance system did not include the prevalence of asymptomatic infection, and only symptomatic cases were recorded. Possibly, there might be much more cases with asymptomatic infection than reported cases. The asymptomatic people also have a risk of developing severe dengue, if any, by secondary infection. Moreover, the asymptomatic people with persistent viremia may contribute to dengue transmission to mosquitoes or contact people by atypical contamination. Therefore, travelers should consider asymptomatic dengue infection and subsequent risk. And monitoring and surveillance system for travelers returning from dengue-endemic countries are required to detect any asymptomatic infection and to control virus transmission.
Although there were no indigenous DF cases in Korea, imported cases occurred every year and 1,339 cases were reported between 2001 and 2015. Previous studies have estimated that severe dengue may develop in 1%–5% of total dengue-infected people and, if treated, a mortality rate is less than 1% (1263). The data indicate an accumulation of infected people in Korea may predispose to severe dengue infection and dengue-associated deaths. Moreover, because most of people with primary infection are asymptomatic, more people have the potential risk of developing severe dengue. For example, considering asymptomatic cases comprise 80% of the total cases, it is expected that an estimated 6,700 people may have been exposed with DENV. Furthermore, supposing approximately 2,000 people (30% of 6,700 people) have frequent revisit to endemic regions, an estimated 20–100 people (1%–5% of the 2,000 people) may develop severe dengue by repetitive infection and approximately 0.2–1 dengue-related death (1% of the 20–100 people) may occur in near future.
There are several limitations in current study. Because only low numbers of imported cases were reported in Korea, there was no detailed epidemiological information available for risk analysis. This lack of epidemiological knowledge makes it difficult to assess distinct risk by gender and age distribution. To further analyze the risk factors, more detailed information such as visit locations (urban or rural) and duration is required. Furthermore, it is difficult to detect repetitive infection and severe dengue cases because symptomatic information such as time of onset, disease severity and virus serotypes were not available. As there has been an increasing trend in imported dengue cases in Korea, it is required to analyze risk factors for severe dengue with more data in the future.
In conclusion, as dengue infection has rapidly spread around world, imported cases also have been increased continuously in Korea. Recent data in Korea demonstrated that most of dengue cases were imported from Southeast Asia and the seasonal trend is also similar to those of endemic countries. An increasing trend in dengue cases in Korea may contribute to introduction of severe dengue and autochthonous outbreak, as indicated by the recent dengue outbreak in Japan. Furthermore, unreported asymptomatic infection can increase a risk of severe dengue and virus transmission. To minimize a risk of dengue infection, travelers planning to endemic regions should consider current dengue situation and try to avoid mosquito biting or abstain from repetitive visit to endemic countries. In addition, considering global trend of mosquito-borne disease, more active surveillance is required to prevent the importation of DENV. Introduction of diagnostic and monitoring system for travelers returning from endemic area would be helpful to preventing indigenous dengue outbreak and transmission.
 XML Download
XML Download