

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common preventable complication experienced by critically ill patients hospitalized in intensive care units (ICUs). The increased risk of VTE is due to immobilization related to severe illness, sedating medications, and invasive procedures (1). The estimated incidence of DVT in critically ill patients varies from 13% to 31%, depending on study design. DVT is responsible for most cases of PE, a potentially life-threatening condition that has a reported 30% mortality rate in the ICU (23).
Currently, prevention techniques for VTE in critically ill patients include pharmacological thromboprophylaxis and mechanical thromboprophylaxis. Pharmacological thromboprophylaxis, which is often used in medical critically ill patients, includes unfractionated heparin (UFH) and low-molecular-weight heparin (LMWH). The 9th American College of Chest Physicians (ACCP) Antithrombotic Therapy and Prevention of Thrombosis Guidelines suggest the use of UFH or LMWH based on low-quality evidence (Grade 2C) (4). In a recent meta-analysis, Alhazzani et al. (5) reported that thromboprophylaxis with any type of heparin reduced the rates of DVT to half (pooled risk ratio, 0.51; 95% CI, 0.41–0.63). The efficacy of mechanical prophylaxis in critically ill patients, compared to pharmacological prophylaxis, is based on even weaker evidence. The ACCP guidelines suggest the use of mechanical prophylaxis in critically ill patients who are bleeding or at high risk for major bleeding (Grade 2C) based on a systematic review of two randomized clinical trials (RCTs) that included patients who underwent major orthopedic surgery (4678). In a recent retrospective audit of 28 North American ICUs, guideline concordance with use of pharmacological thromboprophylaxis was 95.5%. However, when considering the absolute proportion of each prophylactic intervention, approximately one-fourth (9.5% mechanical prophylaxis alone, 15.3% no prophylaxis) of the patients did not receive pharmacological prophylaxis. The lack of pharmacological prophylaxis was mainly attributed to clinical bleeding or risk of bleeding, which together accounted for approximately 71% of the reasons for not using an anticoagulant (9). Up to 80% of critically ill patients experience at least one or more episodes of bleeding, so the actual utilization rate of mechanical prophylaxis is expected to be quite high, despite the lack of evidence for efficacy and safety in this special population.
Until now, no meta-analysis has compared the efficacy and safety of various approaches to thromboprophylaxis, including both pharmacological and mechanical interventions, in critically ill patients. Recently, two RCTs have reported results of trials evaluating the role of mechanical prophylaxis in the critically ill (1011).
Therefore, we performed a comprehensive Bayesian network meta-analysis to compare the efficacies and safety profiles of UFH, LMWH, mechanical prophylaxis, and no prophylaxis. We aimed to compare the efficacies of current thromboprophylaxis interventions and their effects on major bleeding, with particular attention paid to comparisons between intermittent pneumatic compression (IPC) and various types of heparin and between IPC and the control group.
MATERIALS AND METHODS
Data sources and searches
We searched PubMed, EMBASE, the Cochrane Central Register of Controlled Trials, and the United States National Institutes of Health Registry of Clinical Trials (www.clinicaltrials.gov) for pertinent published and unpublished studies. Our detailed search strategy is presented in the Online-Only Supplements. Additional data sources included conference proceedings from the American Thoracic Society (1994–2014), the Society of Critical Care Medicine (1994–2013), the European Society of Intensive Care Medicine (1994–2014), the American College of Chest Physicians (1994–2014), and the International Symposium on Intensive Care and Emergency Medicine (1997–2014). The electronic search strategy was complemented by a manual review of the reference list of each included article. Reference lists of recent reviews, editorials, and meta-analyses were also examined. No restrictions were imposed on language, study period, or sample size (12).
Study selection
We included RCTs that assessed the efficacy and safety of thromboprophylaxis for VTE, including DVT or PE, whose study population consisted of medical or surgical critically ill patients, including patients with major trauma. We defined critically ill patients as those who received care in an ICU setting. Pharmacological thromboprophylaxis included any form of heparin (UFH or LMWH) and mechanical prophylaxis included IPC or sequential compression devices. To be included in our analysis, clinical outcomes of efficacy (the incidence of DVT) and safety (the incidence of major bleeding) at the most recent available follow-up were clearly reported. We excluded RCTs that included pediatric patients and randomized crossover trials that assigned patients to multiple treatment arms simultaneously.
Data extraction and quality assessment
For our analysis, we examined summary data reported in the published articles. A standardized form was used to extract the following information for each study: trial characteristics; study design, including generation of randomization sequence, allocation concealment, crossover between assigned groups, number of post-randomization withdrawals, and loss to follow-up; number of study patients; age of patients; cause of ICU admission and underlying co-morbidities; inclusion and exclusion criteria for the trial; detailed protocols of each intervention, such as the dose, duration, and route of administration of pharmacological thromboprophylaxis or application duration of mechanical thromboprophylaxis; diagnostic modality and time point for evaluation of VTE; length of follow-up; and clinical outcomes regarding efficacy (the incidence of DVT) or safety (the incidence of major bleeding) reported on an intention-to-treat basis. The quality of eligible RCTs was assessed using the Cochrane Collaboration’s tool for assessing the risk of bias for RCTs (Supplementary Table 1) (13). We also reported the Jadad score for quantitative comparison among the included trials (14). Two investigators independently screened the titles and abstracts, identified duplicates, reviewed full articles, and determined eligibility for this analysis. Disagreements were resolved by a thorough discussion. The last search was performed in June 2014.
Outcomes and definitions
The primary outcome measure was overall incidence of DVT at the longest available follow-up. The secondary outcome measure was the incidence of major bleeding, as defined by the original trials. We defined four treatment groups: UFH, LMWH, IPC, and control. The control group included patients who received no thromboprophylaxis or who were treated only with gradual compression stockings. All patients and outcomes were analyzed according to the group in which they were assigned in the original study.
Data synthesis and analysis
A Bayesian random effects model for multiple treatment comparisons was constructed to compare the primary outcome (the incidence of thromboembolism) among the four groups (LMWH, UFH, IPC, and control). We used a Bayesian extension of the hierarchical random effects model proposed by Lumley for networks of multi-arm trials (15). Odds ratios (ORs) with 95% credible intervals (CrIs) are presented as summary statistics. Non-informative prior distributions were selected to allow the data to dominate the final results. We performed Markov chain Monte Carlo samplers in WinBUGS v.1.4.3 (MRC Biostatistics Unit, Cambridge, UK), and we ran four chains with different starting values. A burn-in phase of 10,000 iterations was followed by 50,000 updates; the number of burn-in iterations was chosen according to the Brooks-Gelman-Rubin method for convergence checks (16). Pair-wise ORs were estimated from the median of the posterior distribution, with CrIs obtained from the 2.5th and 97.5th percentiles. Results were considered significant if the CrIs of the ORs did not include 1. Pair-wise inconsistency and inconsistency between direct and indirect effect estimates were assessed with the node-splitting method, followed by an evaluation of inconsistency among P values. Heterogeneity across trials was evaluated by I2 statistics, which is consistent with a frequentist meta-analysis. In a pooled analysis of the secondary outcome (the risk of major bleeding), we stratified all of the included trials according to the baseline risk of bleeding. Since the trials showed heterogeneous risks for major bleeding, we separately evaluated the pooled risk of bleeding for each treatment group in trials that enrolled medical critically ill patients and trials that enrolled patients with major trauma or a high-risk of bleeding, such as patients with overt coagulopathy or active bleeding. Statistical analysis was performed with WinBUGS v.1.4.3 and R programming language, version 3.0.2 (R Foundation for Statistical Computing, Vienna, Austria). The к statistic was used to assess agreement between investigators for study selection. The present study was performed in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and the review protocol has not been registered (Supplementary Table 2) (17).
RESULTS
Search results
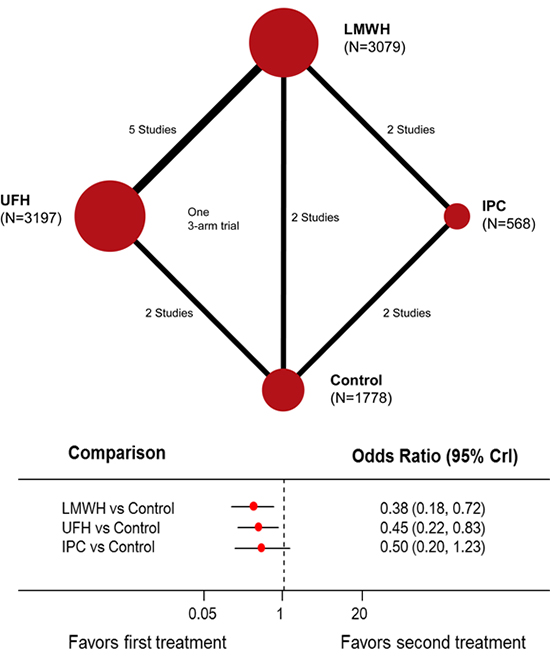
We identified 254 citations, retrieved 19 studies for detailed evaluation, and obtained 12 RCTs that met our inclusion criteria (Fig. 1A) (101118192021222324252627). The characteristics and reasons for exclusion of the seven eliminated studies are summarized in the supplementary materials. The inter-observer agreement for study selection was high (к = 0.91). The 12 RCTs included a total of 8,622 critically ill patients. The interventions for thromboprophylaxis were UFH in 3,197 patients (37.1%), LMWH in 3,079 patients (35.7%), and IPC in 568 patients (6.6%). The control group included 1,778 patients (20.6%) who did not receive any of these interventions for thromboprophylaxis. One trial was a 3-arm trial comparing UFH, LMWH, and control groups (Fig. 1B) (26).
Fig. 1
Flow diagram of trial selection and network plot of the meta-analysis. (A) The flow diagram follows the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). (B) Network plot of meta-analysis model: each treatment is represented by a node; the size of the node is proportional to the sample size randomized to each group and the thickness of the line connecting the nodes is proportional to the total randomized sample size in each pair-wise comparison.
LMWH = low-molecular-weight heparin, IPC = intermittent pneumatic compression, UFH = unfractionated heparin.

Trial characteristics
The main characteristics of the individual studies are summarized in Table 1. Six of the 12 trials included patients in the medical ICU (1021232526) and three trials involved trauma patients admitted to the ICU (182427). One trial included surgical critically ill patients (22) and two trials included both medical and surgical critically ill patients (1119). One trial did not specify the type of ICU (20). Fraisse et al. (23) reported a trial conducted in patients with acute exacerbations of COPD and Shorr and Williams (26) presented a post-hoc analysis regarding the efficacy of thromboprophylaxis from a trial conducted with sepsis patients. In all included trials, patients in the UFH groups were treated with 5000 U of UFH subcutaneously twice daily. In the LMWH groups, three different preparations, fraxiparin, enoxaparin, and dalteparin, were administered. The dosages and schedules of LMWH preparations varied among the trials (Table 1). In all but one study, the occurrence of DVT was measured with Doppler ultrasonography (USG); the remaining trial employed daily leg scanning using 125I-labeled fibrinogen (20). Supplementary Fig. 1 shows the risk of bias graph and illustrates the proportion of studies with each of the judgments for each entry in the Cochrane Collaboration’s tool. A full description of the summary of risk of bias judgments of each study is available in Supplementary Fig. 2 and Supplementary Table 1. Four trials with an IPC arm showed a high-risk of bias for the blinding procedure (10112427). However, blinding of patients and caregivers was inherently impossible in these trials and bias from the lack of double-blinding would likely not change the results of the current meta-analysis, since the diagnostic modalities and methods for DVT were objective methods and would not be influenced by the lack of blinding.
Table 1
Characteristics of included trials

| Trial (Ref) | Involved population | Inclusion criteria | Exclusion criteria | Intervention (No. of patients) | Control (No. of patients) | Other measures of prophylaxis | Intervention period | Follow-up period | Outcome assessment | Definition of major bleeding |
|---|---|---|---|---|---|---|---|---|---|---|
| Cade et al. (20) | Single center (Australia) | Patients admitted to general ICU | Age < 40 yr; impaired hemostasis; unable to undergo leg scanning | UFH 5000 U SC bid (60) | Placebo: isotonic saline SC bid (59) | N.R. | From < 24 hr to 10 days or fully ambulant or VTE occurrence | 4 to 10 days | Daily leg scanning using 125I-labeled fibrinogen | N.R. |
| Geerts et al. (18) | Single center (Canada) | Adult; severe injury, ISS ≥ 9 | ISS < 9; frank intracranial bleeding; bleeding that remained uncontrolled for 36 hr; systemic coagulopathy; anticoagulation indicated | LMWH: Enoxaparin 30 mg bid (136) | UFH 5000 U SC bid (129) | Not allowed | From < 36 hr to 14 days | 14 days | Venography between days 10 and 14; daily clinical assessment; venography conducted if suspicious Doppler USG findings | Hb decrease ≥ 2.0 g/dL; transfusion of ≥ 2 packs RBC; intracranial or retroperitoneal bleeding; need for surgical intervention |
| Kapoor et al. (25) | Single center (US) | Patients admitted to MICU | Patients requiring full dose anticoagulation; bleeding disorder | UFH 5000 U SC bid (401) | Placebo (390) | N.R. | During ICU stay | Until discharge | Venous duplex study every 72 hr; ± V/Q scan | N.R. |
| Fraisse et al. (23) | 34 MICUs (France) | AE-OPD requiring MV; age 40–80 yr; weight 45–110 kg | Confirmed DVT; bleeding lesion; hepatic or renal failure; uncontrolled HTN; coagulation disorder; history of heparin-related side effects | LMWH: Fraxiparin 3800 AXa IU for 45 to 70 kg SC qd; 5700 AXa IU for 71 to 110 kg, SC qd (84) | Placebo: isotonic saline SC qd (85) | N.R. | Until MV weaning; maximum 20–22 days | 20 to 22 days | Daily PE; Doppler USG once weekly; venography at end of study; ± pulmonary angiography | Hb drop > 2.0g/dL; transfusion of ≥ 2 packs RBC; intracranial or retroperitoneal bleeding; treatment halted |
| Goldhaber et al. (21) | 28 institutions (US) | MICU patients | N.R. | LMWH: Enoxaparin 30 mg SC bid (156) | UFH 5000 U SC bid (154) | GCS | N.R. | 14 days | Doppler USG on days 3, 7, 10, 14 | N.R. |
| Shorr et al. (26) | Multinational, multicenter | Age > 18 yr; severe sepsis; multiple organ failure; APACHE II score > 25 | Concurrent need for other anticoagulant medication; renal failure; not expected to survive 28 days; lack of commitment for aggressive management |
(1) LMWH: Enoxaparin 40 mg SC qd (478) (2) UFH 5000 U SC bid (498) |
Placebo: isotonic saline SC bid (959) | Mechanical methods (not specified) | Initial 4 days | 28 days | Doppler USG on days 4, 6, 28 | N.R. |
| De et al. (22) | Single center (India) | Critically ill patients (required ICU care > 1 day); age > 40 yr; scheduled for major elective surgery (required GA and > 6 days of hospitalization) | Bleeding diathesis; hepatic or renal failure; HIT; hemorrhagic stroke; GI bleeding; pregnancy or lactation | LMWH: Enoxaparin 40 mg SC qd (81) | UFH 5000 U SC bid + placebo (isotonic saline) (75) | Not allowed | From 1–12 hr before surgery to minimum of 6 days postoperatively; discontinued when fully mobile | 6 mon | Doppler USG between days 5 and 7; outpatient follow-up at 4 wk and 6 mon | GI bleeding diagnosed on stool test or upper GI endoscopy; any bleeding episode requiring reoperation |
| PROTECT (19) | Multinational, multicenter | Age > 18 yr; weight > 45 kg; expected to remain in ICU > 3 days | Major trauma; neurosurgery or orthopedic surgery; need for therapeutic anticoagulation; heparin administration in the ICU for at least 3 days; pregnancy; life-support limitation | LMWH: Dalteparin 5000 U SC qd + placebo SC qd (1873) | UFH 5000 U SC bid (1873) | Per protocol; alternative anticoagulant agent or mechanical prophylaxis (GCS or IPC) was applied | During ICU stay | 100 days | Doppler USG within 2 days after admission and twice weekly | Hb decrease ≥ 2.0 g/dL; transfusion of ≥ 2 packs RBC; intracranial or retroperitoneal bleeding; need for surgical intervention |
| Ginzburg et al. (24) | Single center (US) | Adult; severe injury, ISS > 9; one arm and one leg available for IPC | Need for systemic anticoagulation; unlikely to survive or remain in hospital > 7 days; renal failure; pregnancy; BMI > 25 kg/m2 | LMWH: Enoxaparin 30 mg SC bid (218) | IPC* (224) | Not allowed | From < 24 hr after trauma until independent walking or discharge | 30 days | Doppler USG within 24 hr and weekly thereafter or as indicated when DVT was suspected | Hb decrease ≥ 2.0 g/dL; transfusion of ≥ 2 packs RBC; intracranial or retroperitoneal bleeding; need for surgical intervention |
| Kurtoglu et al. (27) | Single center (Turkey) | Patients with severe head/spinal trauma in ICU | Age < 14 yr; hepatic or renal failure; spinal cord injury; history of DVT; high bleeding risk; regular use of anticoagulant | LMWH: Enoxaparin 40 mg SC qd (60) | IPC† (60) | All patients were placed on IPC on admission to ICU | From < 24 hr after admission for 7–10 days | Until 1 week post discharge | Doppler USG on admission to ICU, weekly, and one week after discharge | Macroscopic hematuria without renal injury; overt bleeding; and Hb decrease ≥ 2.0 g/dL |
| Zhang et al. (10) | Single center (China) | Patients admitted to ICU | Regular use of anticoagulant | IPC‡ (79) | No thrombo-prophylaxis (83) | Not allowed | 28 days after ICU admission | 28 days | Doppler USG on days 1, 3, and 7, then once a week | N.R. |
| Vignon et al. (11) | Multicenter (France) | Age > 18 yr; high risk of bleeding on ICU admission: (1) symptomatic bleeding; (2) organic lesion likely to bleed; (3) PLT < 50000, aPTT ratio > 2, PT% < 40% | History of DVT; ICU stay of > 36 hr or likely to be < 72 hr; life-support limitation; mechanical heart valve; contraindications to mechanical prophylaxis (i.e., severe limb arteriopathy) | IPC§ and GCS (205) | GCS (202) | Not allowed | 6 days after ICU admission | Follow up on days 30 and 90 | Compression ultrasonography on day 6 | N.R. |
AE-COPD = acute exacerbated chronic obstructive pulmonary disease, BMI = body mass index, bid = twice daily, DVT = deep vein thrombosis, GA = general anesthesia, GCS = graduated compression stocking, GI = gastrointestinal, Hb = hemoglobin, HIT = heparin-induced thrombocytopenia, HTN = hypertension, ICU = intensive care unit, IPC = intermittent pneumatic compression, ISS = injury severity score, LMWH = low molecular weight heparin, MICU = medical ICU, MV = mechanical ventilation, N.R. = Not reported, PE = physical examination, qd = once daily, RBC = red blood cells, SC = subcutaneous injection, UFH = unfractionated heparin, USG = ultrasonography, VTE = venous thromboembolism.
*Flowtron, Huntleigh Healthcare; †Flowtron Excell, Huntleigh Healthcare or AV Impulse System Duo, Novamedix; ‡Lympha-Tron type air pressure wave therapeutic apparatus, Daesung Maref; §SCD EXPRESS compression system with adapted tubing sets and thigh sleeves, Covidien.
Comparison of overall risk of DVT
In all, the 12 trials included 8,622 patients with identified DVT (Table 2) (101118192021222324252627). In a pooled analysis of overall incidence of DVT, the use of LMWH or UFH was associated with a significantly lower risk of DVT than the control group (LMWH: OR, 0.38; 95% CrI, 0.18–0.72; UFH: OR, 0.45; 95% CrI, 0.22–0.83). The efficacy of LMWH in reducing the risk of DVT was similar to the efficacy of UFH (OR, 0.86; 95% CrI, 0.47–1.48). IPC showed a trend toward lowering the DVT risk compared to the control group, but this difference was not significant (OR, 0.50; 95% CrI, 0.20–1.23) (Supplementary Table 3). Although LMWH and UFH showed lower risks of DVT than IPC, the differences were not statistically significant (LMWH: OR, 0.76; 95% CrI, 0.28–1.92; UFH: OR, 0.89; 95% CrI, 0.31–2.41; Fig. 2A). The significant benefit of LMWH or UFH compared to the control group was consistently observed in both direct and indirect estimates of the comparisons, with acceptable ranges of statistical heterogeneity. In a ranking probability analysis, LMWH showed the highest probability of reducing the risk of DVT (48.6%; Fig. 2B and 3).
Table 2
Incidence of DVT and major bleeding in each trial

| References | DVT | Major bleeding | ||||||
|---|---|---|---|---|---|---|---|---|
| LMWH | UFH | IPC | Control | LMWH | UFH | IPC | Control | |
| Standard risk of bleeding (medical critically ill) | ||||||||
| Kapoor et al. (25) | - | 44/401 | - | 122/309 | - | - | - | - |
| Fraisse et al. (23) | 13/84 | - | - | 24/85 | 6/84 | - | - | 3/85 |
| Goldhaber et al. (21) | 25/156 | 20/154 | - | - | 3/156 | 3/154 | - | - |
| Shorr et al. (26) | 23/478 | 26/498 | - | 56/959 | - | - | - | - |
| De et al. (22) | 1/81 | 2/75 | - | - | 1/81 | 2/75 | - | - |
| PROTECT | 138/1873 | 161/1873 | - | - | 103/1873 | 105/1873 | - | - |
| Zhang et al. (10) | - | - | 3/79 | 16/83 | - | - | - | - |
| High risk of bleeding (trauma patients or surgical critically ill) | ||||||||
| Geerts et al. (18) | 40/129 | 60/136 | - | - | 5/129 | 1/136 | - | - |
| Ginzburg et al. (24) | 1/218 | - | 6/224 | - | 4/218 | - | 4/224 | - |
| Kurtoglu et al. (27) | 3/60 | - | 4/60 | - | 2/60 | - | 1/60 | - |
| CIREA1 | - | - | 10/205 | 16/202 | - | - | 17/205 | 20/202 |
| Bleeding risk not stated | ||||||||
| Cade et al. (20) | - | 8/60 | - | 17/59 | - | - | - | - |
Fig. 2
Comparative efficacy of thromboprophylaxis interventions in the prevention of deep vein thrombosis (DVT). (A) Estimated odds ratios (ORs) and 95% credible intervals (CrIs) for DVT from network meta-analysis for different thromboprophylaxis interventions, according to a Bayesian network meta-analysis with random effects model. The circles and horizontal lines indicate pair-wise OR and 95% CrI, respectively. (B) Rank probability of each treatment arm for the risk of DVT. The number on the horizontal axis is the possible rank of each treatment, from best to worst according to the outcome. The size of each bar corresponds to the probability of each treatment being at a specific rank.
LMWH = low-molecular-weight heparin, IPC = intermittent pneumatic compression, UFH = unfractionated heparin.


Comparison of overall risk of major bleeding
The incidence of major bleeding was reported in eight of the 12 trials (Table 2) (1118192122232427). A network meta-analysis of the eight trials showed an insignificant trend of increased major bleeding in LMWH and UFH groups compared to the IPC and control group (Fig. 4A and Supplementary Table 3). However, the eight trials included four RCTs in the medical ICU and three RCTs with trauma patients and one RCT which included patients with high risk of bleeding. Since the two groups of trials showed different risks of major bleeding, we separately analyzed the risk of major bleeding in medical and surgical critically ill patients, according to the baseline risk of major bleeding. In medical critically ill patients with a standard bleeding risk, UFH and LMWH conferred insignificant trend of increased major bleeding compared with the control group (Fig. 4B). In surgical critically ill patients with a high risk of bleeding, UFH showed a tendency toward a decreased incidence of major bleeding compared with LMWH, IPC, and control groups. However, statistical significance was not observed (Fig. 4C).
Fig. 4
Comparative safety of thromboprophylaxis interventions for the risk of major bleeding. (A) Estimated odds ratios (ORs) and 95% credible intervals (CrIs) for major bleeding from eight trials reporting the incidence of major bleeding. (B) Estimated OR and 95% CrI for major bleeding from four trials that included medical critically ill patients with a standard risk of bleeding. (C) Estimated OR and 95% CrI for major bleeding from four trials that included surgical or trauma critically ill patients with a high risk of bleeding. The circles and horizontal lines indicate Bayesian ORs and 95% CrIs, respectively.

DISCUSSION
In this network meta-analysis, we aimed to compare the efficacy and safety of current techniques for thromboprophylaxis in critically ill patients. We observed a significant reduction of DVT risk with pharmacologic prophylaxis, including UFH and LMWH, compared to the control group. The efficacies of thromboprophylaxis of UFH and LWMH were similar. The risk of DVT in patients who had mechanical thromboprophylaxis was marginally lower, but the trend was statistically insignificant. The risk of major bleeding was not significantly different among the UFH, LMWH, IPC and control groups in critically ill patients regardless of their risk of bleeding.
To our knowledge, this is the first network meta-analysis of contemporary thromboprophylaxis interventions in critically ill patients and we performed multiple treatment comparisons that were previously unavailable. Two previous meta-analyses separately compared the efficacy of heparin to placebo (5) and mechanical thromboprophylaxis to LMWH (28). Alhazzani et al. (5) reported that the use of any heparin preparation was associated with a 50% reduction in the risk of DVT (pooled risk ratio 0.51; 95% CrI, 0.41–0.63; P < 0.001; I2 = 77%) compared to placebo. The difference in DVT risks between UFH and LMWH was not significant. In the current meta-analysis, we evaluated 12 RCTs, 10 of which included any heparin. Like the previous analysis, we observed a significant reduction in the risk of DVT with heparin compared with the control group (LMWH: OR, 0.38; UFH: OR, 0.45). Since the last evidence synthesis, no additional trial directly comparing the efficacy of heparin to the control group was reported, so the greater estimated risk reduction reported in our results is likely attributable to the indirect comparison of LMWH to the control group via IPC. We observed comparable efficacies of UFH and LMWH, which was also in agreement with the previous analysis.
Contrary to pharmacologic thromboprophylaxis, little evidence is available to guide clinicians in the efficacy of mechanical thromboprophylaxis. Current ACCP guidelines are based on two RCTs that compared the effect of IPC plus anticoagulation vs. anticoagulation alone in patients undergoing major orthopedic surgery, not in critically ill patients (4678). Despite the extensive use of mechanical prophylaxis in critically ill patients, evidence is limited to only one meta-analysis that included only two RCTs comparing IPC and LMWH (28).
In our current analysis, the efficacy of IPC in preventing DVT was evaluated more precisely than in the previous meta-analysis. We included two recent trials (1011) that directly compared the efficacy of IPC to a control group and also indirectly compared IPC to a control group via LMWH arms. Additional inclusion of recent trials and indirect comparison via network model in our analysis expanded the evidence for evaluating the efficacy of IPC as thromboprophylaxis. We observed a trend of reduced DVT risk with IPC compared to the control group, but the reduction was not statistically significant. The use of IPC is relatively widespread and unrestricted in routine practice, but our results question the evidence of thromboprophylactic efficacy of IPC. Moreover, recent report of a prospective cohort shows that nonleg venous thromboses are found in 2.2% of medical-surgical critically ill patients, primarily in deep veins and proximal veins (29). It could be explainable that the relatively inferior efficacy of IPC to systemic pharmacological thromboprophylaxis might be attributable to the increased incidence of nonleg venous thrombosis.
The risk of major bleeding is an important outcome of thromboprophylaxis in critically ill patients, since major bleeding events can be potentially life-threatening. Additionally, both bleeding itself and subsequent discontinuation of thromboprophylaxis adversely affect clinical outcomes in the ICU. The risk of bleeding is one of the main determinants of thromboprophylaxis strategy, so we separately analyzed this outcome in medical and surgical critically ill patients. In patients with a standard risk of bleeding (medical critically ill patients), the LMWH, UFH, and control groups did not show differences in the risk of major bleeding. In patients with a higher risk of major bleeding (surgical critically ill patients, including trauma patients), UFH was insignificantly associated with less major bleeding than the LMWH, IPC, or control groups. However, this result is primarily driven by the results of one RCT that compared LMWH and UFH in patients with major trauma. After reviewing all six major bleeding episodes (1 with heparin vs. 5 with LMWH), the percentage of patients who required a transfusion, and the amount of transfusion needed, the authors of the trial concluded that the difference in major bleeding risk between UFH and LMWH was not significant.
In the current guidelines, as well as in routine daily practice, the choice of thromboprophylaxis largely depends on a patient’s risk of bleeding. Therefore, the current analysis should be applied to patients according to individual bleeding risk. In critically ill patients with a standard risk of bleeding, pharmacologic thromboprophylaxis with any form of anticoagulant is likely the intervention of choice.
On the basis of our results, we are concerned that mechanical thromboprophylaxis is over-used in critically ill patients with a high risk of bleeding. As shown in the current meta-analysis, the evidence supporting the efficacy of IPC in DVT prophylaxis is not as robust as the evidence supporting pharmacological thromboprophylaxis. Moreover, patients with trauma and major surgical procedures did not show significantly increased risks of major bleeding with pharmacological thromboprophylaxis. Further, mechanical thromboprophylaxis can cause the spread of nosocomial infections, induce mechanical problems of the lower extremity, and dislodge pre-formed DVT that can result in fatal PE (303132). Such potential safety issues are more pronounced in critically ill patients. In addition, the routine use of IPC places a higher economic burden on the healthcare system, especially in developing countries with limited resources for critical care medicine. Therefore, in patients without evidence of active bleeding or risk of life-threatening bleeding, pharmacological thromboprophylaxis could be a more effective, equally safe, and less expensive measure for the prevention of VTE. Patients currently categorized as having a high risk of bleeding may be better sub-categorized according to their actual bleeding risk. The actual risk of major bleeding in various patient groups, such as critically ill patients with bleeding risk due to trauma, post-surgical patients, not including intracranial or intraocular surgery, and patients with a recent history of major bleeding in an internal organ, should be further tested in future trials. In addition, given the limited evidence regarding the efficacy of mechanical thromboprophylaxis, more studies evaluating the role of mechanical prophylaxis are required in critically ill patients, especially those who cannot tolerate systemic anticoagulation.
Our analysis has some important limitations. First, this meta-analysis included clinically and methodologically diverse studies. Although we included only RCTs in the final analysis and achieved insignificant statistical heterogeneity, the study designs and populations differed. In addition, this was a study-level meta-analysis, so data from individual patients were not included and, therefore, we could not adjust for patient-level confounders. Second, different diagnostic methods were used for the evaluation of DVT. Although most of the studies reported results of Doppler ultrasonography, one trial used 125I-labeled fibrinogen leg scans and another trial performed venography at the end of the study. Third, the follow-up durations were diverse among the trials, ranging from 14 days to 6 months. Fourth, the definition of major bleeding varied slightly among the included trials. Finally, we focused on DVT as the primary outcome. Reduced risk of DVT cannot directly correlate with reduced risk of PE. However, PE was not diagnosed by universal screening of patients and all trials that reported the incidence of PE performed confirmative diagnostic tests only in patients who were clinically suspected of having a PE. Therefore, the pooled analysis with PE is prone to bias.
In critically ill patients, the efficacy of mechanical thromboprophylaxis in reducing the risk of DVT is not as robust as those of pharmacological thromboprophylaxis. The risk of bleeding does not appear to be significantly influenced by the use of heparin, even in patients with a high risk of bleeding. The choice of best thromboprophylaxis technique still needs further investigations.
 XML Download
XML Download