

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Preterm birth is defined as a birth occurring at less than 37 weeks of completed gestation. Preterm infants are vulnerable to serious medical complications and/or mortalities during the neonatal period as well as morbidities later in life (123). Preterm birth has many potential adverse effects on health, such as sensory deficits, lower weight and height in later life, impaired cognitive function, and cerebral palsy (456789). The morbidity of preterm birth can persist in later life, resulting in tremendous economic burden as well as physical and psychological problems (1011).
Although the adverse health effects of preterm birth are highly recognizable as medical conditions, the causes for preterm birth remain largely unknown. A complex mix of maternal characteristics such as genetics, age, infections, chronic conditions, and socioeconomic and lifestyle factors are suspected to be important risk factors (121314). Several possible etiological routes have the potential to result in spontaneous preterm birth (15). Hewitt (16) reported a seasonal pattern of still births in 1962; subsequently, many researchers have been interested in the environmental and meteorological factors affecting adverse birth outcomes and preterm births.
Although seasonal patterns of birth have been documented in human populations for almost two centuries, studies have drawn alternative conclusions regarding seasonal peaks of preterm births (171819). Cultural, biological, and environmental factors are hypothesized to contribute to these seasonal patterns, which differ across location and time. The investigation of seasonal patterns in preterm births may aid the search for the causes of this important condition. No studies have investigated the seasonal patterns of preterm births in Korea. Thus, this retrospective study aimed to investigate the seasonal patterns of preterm births in Korea.
MATERIALS AND METHODS
All data were taken from Korea’s Vital Birth Statistics for the period of 2000–2012. In Korea, birth certificate records are based on records compiled by doctors or nurses at delivery and registered with regional public health centers. The study data included birth weight, neonatal sex, parity, multiple pregnancy, gestational age at delivery, parental age, and parental educational level.
Gestational age at delivery is usually calculated based on the last menstrual period and confirmed by ultrasonic examination during the first trimester. Preterm birth was defined as that occurring at 37 weeks of gestation.
Delivery dates were grouped by the month of the year or by season (winter [December, January, February], spring [March, April, May], summer [June, July, August], and autumn [September, October, November]). The seasonal patterns of the rates of preterm births were assessed.
Data are expressed as mean ± standard deviation (SD) for continuous variables and as percentages for categorical variables. Characteristics among groups were compared using the t-test for differences in continuous variables, and the χ2 test was used for categorical variables. Multivariate logistic regression analysis was used to estimate the adjusted odds ratio (OR) and 95% confidence interval (CI) for the risk of preterm birth. All tests were two-sided, and a P value < 0.05 was considered statistically significant. Statistical analysis was performed using the SPSS package V.17 edition.
RESULTS
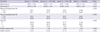
The basic characteristics of the study participants by season at delivery are summarized in Table 1. The table includes maternal age, paternal age, maternal educational level, paternal educational level, parity, multiple pregnancy, and neonatal gender. These variables were statistically significant (P < 0.001), indicating that basic characteristics at delivery could be considered different among each season.
Table 1
Basic characteristics of participants by season at delivery for 2000–2012
The rate of preterm birth showed two peaks a year, once in summer and again in winter (Fig. 1). To determine the seasonal effects on preterm births, the basic characteristics of the participants needed to be controlled, as these can influence the results as confounding variables. Therefore, we used multiple logistic regression analysis. In conclusion, the rates of preterm births at 37 weeks were the highest twice a year (once in winter and again in summer). The rates of preterm births increased by 13.9% in summer and 7.5% in winter, respectively, as compared to those in spring (OR, 1.139; 95% CI, 1.127–1.1152, and OR, 1.075; 95% CI, 1.064–1.087, respectively) after controlling for age, the educational level of parents, maternal parity, and neonatal gender (Table 2). Compared to spring, the rates of preterm births increased by about 10% in the summer and winter.

Table 2
Multiple logistic regression analysis for preterm births (< 37 weeks) by seasons at delivery
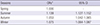
| Seasons | ORs* | 95% CI |
|---|---|---|
| Spring | 1.000 | - |
| Summer | 1.139 | 1.127–1.152 |
| Autumn | 1.053 | 1.042–1.065 |
| Winter | 1.075 | 1.064–1.087 |
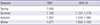
Interestingly, the patterns for spontaneous preterm births occurring at < 34 weeks were similar. The rates of early preterm births increased by 14.5% in summer and 7.7% in winter than that in spring (OR, 1.145; 95% CI, 1.121–1.170, and OR, 1.077; 95% CI, 1.055–1.100) after adjustment for age, the educational level of parents, maternal parity, and neonatal gender (Table 3). The early preterm birth rate showed a greater increase in the odds ratio than preterm births, however the difference between two groups was minor.
DISCUSSION
In this first study of seasonal variation of preterm births in Korea, we observed that the prevalence of preterm births showed a bimodal seasonal pattern that was the highest in the summer and winter. When the contributing factors were equally adjusted, the rates of preterm births increased by approximately 10% in summer and winter as compared to the rate in spring.
Our result is in agreement with previous studies that demonstrated a bimodal seasonal pattern with summer and winter peaks. Keller and Nugent (20) studied 402,540 singleton births from 1967 to 1973 in Minnesota and reported peaks for preterm births in summer and winter. Similar peaks in summer and winter were found in a study of 7,675,006 singleton infants from 1979 to 1983 in Japan (19). On the other hand, studies on seasonality concerning preterm births exist whose results are inconsistent with ours. There are reports of an autumn peak for preterm births in Missouri, USA (17), and a winter peak in London (21). Moreover, a bimodal seasonal pattern in spring and summer was found in Greece (22). Our results are more consistent with those of the study in Japan (19), potentially due to the geographical adjacency and similarities.
The seasonal patterns of preterm births have been studied by many reports, which may suggest a correlation between birth outcomes and seasonal variations, including hot and cold temperatures. Nevertheless, only a few studies have proved the correlation between preterm birth occurrence and exposure to different temperatures. Since we noted higher rates of preterm births in summer and winter, we suggest that ambient temperature could be an important factor leading to higher preterm birth rates. Similarly, other reports have described the maximum ambient temperature to be correlated with preterm births (P < 0.001) (2223). Preterm births increased by 8.6% (95% CI, 6.0–11.3) for every increase of 5.6% in the ambient temperature in California (24). Several biological mechanisms have been reported to support such an effect of warm temperature. One of the possible biological mechanisms by which warm-season temperatures affect preterm births is that heat induces the production of proinflammatory cytokines, such as interleukins and tumor necrosis factor (TNF), causing inflammatory processes at the maternal-fetal interface (25). Furthermore, heat stress increases the production of oxytocin and prostaglandin, which are associated with uterine contraction, inducing early labor (2627). Alternatively, heat stress causes dehydration, resulting in decreases in maternal fluid levels, subsequently reducing the fetal blood volume and leading to the production of the pituitary hormones that provoke labor (14).
Although our results showed higher rates of preterm births in winter than in spring, the mechanism underlying effect of cold temperatures remains unclear. Our result showing that preterm births are frequent in winter is consistent with the study of seasonal peaks on preterm births in Japan, suggesting that the seasonal peaks are dependent on the geographical location, with the winter peak being dominant in northern areas and the summer peak showing dominance in southern areas (19). It has been suggested that cold temperatures could affect pregnancy outcomes and that low ambient temperature could affect fetal birth weight (28); exposure to low winter temperatures during mid-gestation results in low birth weight; consequently, infants born during late spring and summer are lighter than those born in winter. In addition, the cold may influence pregnancy outcomes by decreased human activities, increased exposure to infectious agents, or increased prevalence of specific diseases, such as pregnancy-induced hypertension (12).
Previous studies have focused on each different exposure time during pregnancy, while we focused on the season of births for preterm infants. Murray et al. (28) and Elter et al. (29) concluded that low ambient temperatures in the mid-trimester can be associated with pregnancy outcomes. Alternatively, the season of conception may be an important factor causing spontaneous preterm births (18), suggesting that the beginning of pregnancy is an important etiologic factor related to spontaneous preterm birth. This previous study calculated the estimated date of conception and noted that preterm births often occurred among patients who had begun pregnancy in winter and spring.
Air pollutants, which show increased levels during summer, have been studied as an important factor influencing preterm labor. To be specific, Korea has significant air pollution levels in the transition period between spring and summer. While analyzing the effects of ambient air pollution on preterm births, daily preterm birth rates were shown to be related to average PM2.5 sulfate and PM2.5 water-soluble metal concentrations in the preceding week and to average NO2 concentrations in the preceding 6 weeks (30).
Although the mechanisms of the causality between air pollutants and preterm delivery remain unclear (31), two pathways are considered to be involved—endothelial dysfunction and oxidative stress with consequent placental inflammation (28). Fetal susceptibility to hypoxic injury is due to a leftward shift of the dissociation curve of fetal hemoglobin. Lower baselines for the partial pressure of oxygen and carboxy-hemoglobin levels at equilibrium, which are 10%–15% higher than maternal levels, are also significant factors that render the fetus more vulnerable to oxidative stress. Hypoxic injury is caused by CO, which impairs oxygen transport to the cell and involves leukocytes, platelets, and the endothelium, resulting in a cascade of effects (30). Alternatively, cytokines including interleukin-1, TNF, and interleukin-6, are possibly produced by macrophages following antenatal infection, which then promote preterm labor.
Our study had certain limitations. First, we did not include diverse characteristics of pregnancy, such as preterm and abortion birth history. Second, we could not evaluate the exact reasons for the preterm births. A further limitation was our use of Vital Birth Statistics, which only records data for living children after birth, which meant that stillbirths were excluded from our data. This creates a significant population bias. The definition of preterm birth is independent of the living status of the infants and purely dependent on the gestational period. A population bias would significantly affect our data, thus requiring further investigations that also consider the prenatal death rate.
In conclusion, a seasonal pattern of preterm births was observed in Korea, with peak prevalence in summer and winter. The seasonal pattern described above may provide new insights for the pathophysiological characteristics of preterm births and assist with the formulation of necessary preventable measures and educational support to parents for minimizing the complications of preterm births.
 XML Download
XML Download