

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The prevalence of human immunodeficiency virus (HIV) infection is relatively low in Korea (1). However, in contrast to the global trend, the number of newly diagnosed HIV cases continues to increase. Nationwide data show that the number of newly diagnosed HIV cases rose from 837 in 2010 to 1,114 in 2013 (2). In addition, the mean CD4 cell counts at the time of HIV diagnosis have decreased steadily in Korea (3); in other words, the proportion of late-presenting HIV patients is increasing (4). Late presentation is hazardous to both public health and the individuals concerned. Those who present late are more likely to have illnesses characteristic of AIDS and to exhibit poor responses to antiretroviral therapy (56). From a public health perspective, late presentation of HIV increases the risk of onward HIV transmission (7). Therefore, many authors have sought to identify the risk factors for such late presentation.
MATERIALS AND METHODS
Data sources
Data were derived from city-wide cross-sectional surveys conducted by the Seoul Metropolitan Government in March of 2013 and 2014. HIV-infected adults living in Seoul and enrolled in the National HIV/AIDS Surveillance System participated.
In 2013, 3,144 survival HIV-infected people were living in Seoul. Subjects were randomly selected in those with odd registration number allocated by the Korea Centers for Disease Control and Prevention in 2013; those with even numbers in 2014. In 2013 and 2014, around 25% of subjects by year were selected respectively. Subjects who were native Koreans, ≥ 19 years, HIV-positive, and capable of providing informed consent were selected for this study. As a result, 12%-13% of HIV-infected adults living in Seoul were surveyed in each of the 25 public health center (PHC) district of Seoul in each year.
The officials in charge of the HIV/AIDS programs in each district PHC conducted face-to-face interviews with, and administered questionnaires to, all subjects who agreed to participate. Sex, year of birth, educational level, calendar interval during which HIV was diagnosed, HIV exposure route, reason for HIV testing, and CD4 cell count at the time of HIV diagnosis were recorded.
Study design
Socio-demographic characteristics including sex, age at the time of HIV diagnosis, and educational level were recorded. Age at the time of HIV diagnosis was divided into three classes: 19-34, 35-49, and ≥50 years (91011). Educational level was divided into two classes: high school diploma or less and college or more. Epidemiological characteristics included the HIV exposure route, the calendar interval during which HIV was diagnosed, the reason for HIV testing, and the CD4 cell count at the time of HIV diagnosis. The HIV exposure routes considered were heterosexual, homosexual, and bisexual. Four reasons for HIV testing were considered (4); these were knowledge of HIV status, a request for a health check-up, risky behavior, and development of clinical manifestations. 'Knowledge of status' included the results of voluntary testing in PHCs or hospitals; 'health check-ups' included general health check-ups, appointments seeking medical certificates, operations, or blood donations; 'risky behavior' included being in a sexually transmitted infection (STI) risk group or engaging with HIV-infected partners; 'clinical manifestations' included HIV testing triggered by the development of clinical symptoms. The calendar intervals during which HIV was diagnosed were 1990-1999, 2000-2006, and 2007-2013, based on Korean HIV prevention policies. Around 2000, mandatory HIV testing was abolished and voluntary HIV testing encouraged in Korea; counseling of HIV patients and family members by specialized nurses working in government-designated hospitals commenced in 2007. A subject was considered to be a 'presenter with advanced HIV disease' if the initial CD4 cell count was <200/µL (1213).
Statistical analyses
Continuous variables are expressed as medians with inter-quartile ranges. The chi-square test was used to explore the significance of differences in subject characteristics and CD4 cell counts at the time of HIV diagnosis. Trends over time in the presentation of advanced HIV disease, according to the time interval during which the HIV diagnosis was made, were analyzed using the Cochran-Armitage trend test to explore the significance of the observed increases. Multivariate logistic regression was used to identify factors influencing presentation of advanced HIV disease. The results of such analyses are presented as adjusted odds ratios (aORs) with 95% confidence intervals (CIs) and P values. Model fit was assessed using the Hosmer-Lemeshow goodness-of-fit test. A two-tailed P<0.05 was considered statistically significant. All statistical analyses were performed using SAS 9.3 software (SAS Institute, Cary, NC, USA).
RESULTS
Participants
A total of 812 subjects (25.9%) were selected in 3,144 HIV-infected people. In 2013, 457 subjects were eligible; and 355 subjects were eligible in 2014. In 812 subjects, 53 were excluded because of missing value for epidemiological variables (n=37) and initial CD4 cell count (n=16). Finally 759 subjects (24.1% of 3,144 HIV-infected people living in Seoul) were included.
A total of 759 participants were aged 19-78 years at the time of HIV diagnosis (19-34 years, 42%; 35-49 years, 35%; ≥50 years, 23%). The median age was 37 years (IQR, 29-48 years), and 93% of all subjects were male. The proportions diagnosed in the intervals 1990-1999, 2000-2006, and 2007-2013 were 10%, 39%, and 51%, respectively. Of all subjects, 28.2% presented with advanced HIV disease (CD4 cell count <200/µL). The trend toward presentation with advanced HIV disease has significantly increased over time, from 20% in 1990-1999, to 24% in 2000-2006, and to 33% in 2007-2013 (P<0.01).
Differences in subject characteristics, by age group, among those presenting with advanced HIV disease (CD4 cell count <200/µL) are shown in Table 1. Of subjects aged 19-34 years, those of lower educational levels were more likely to present with advanced HIV disease (P=0.02). Of subjects aged 35-49 years and ≥50 years, those presenting with advanced HIV disease were more likely to exhibit clinical manifestations (P=0.01, P<0.01, respectively). Those ≥50 years of age presenting with advanced HIV disease were less likely to have been diagnosed during 2000-2006 (P<0.01).
Factors influencing presentation with advanced HIV disease according to age group
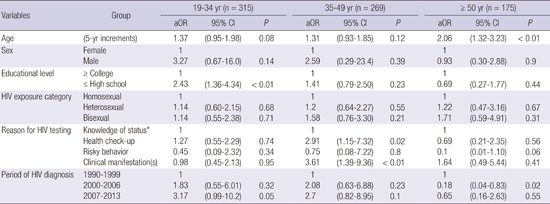
Table 2 presents the results of multivariate logistic regression of the factors influencing presentation with advanced HIV disease at the time of HIV diagnosis according to age group. Of subjects aged 19-34 years, presentation with advanced HIV disease was significantly more common among subjects with educational levels of high school or less (aOR, 2.43; 95% CI, 1.36-4.34); though failed to show statistical significance, those recently diagnosed with HIV were more likely to be presented with advanced HIV disease (aOR, 3.17; 95% CI, 0.99-10.2). Of subjects aged 35-49 years, presentation with advanced HIV disease was associated with the HIV diagnosis at the health check-up (aOR, 2.91; 95% CI, 1.15-7.32) or development of clinical manifestations (aOR, 3.61; 95% CI, 1.39-9.36). Among subjects aged ≥50 years, presentation with advanced HIV disease was significantly more common as age increased (aOR per increment of 5 years, 2.06; 95% CI, 1.32-3.23) and significantly less common among subjects diagnosed with HIV in the interval 2000-2006 (aOR, 0.18; 95% CI, 0.04-0.83). Hosmer-Lemeshow goodness-of-fit testing revealed that all three multivariate models were good fits (χ2=11.38, P=0.18; χ2=6.44, P=0.59; χ2=4.55, P=0.71, respectively).
DISCUSSION
We found that the factors positively influencing presentation with advanced HIV disease were lower educational level among adults aged 19-34 years; HIV testing during health check-ups, or after clinical manifestations developed, among adults aged 35-49 years; and older age among adults aged ≥50 years. We found that in subjects aged 19-34 years, presentation with advanced HIV disease was associated with a lower educational level. Previous studies showed that lower educational levels were negatively associated with a willingness to undergo HIV testing (1415). This explains why presentation with advanced HIV disease was more common among the individuals with lower educational level. Educational programs focusing on the importance of HIV testing should be implemented in high schools (thus prior to graduation).
We found that old age (≥50 years) was associated with presentation with advanced HIV disease, and recent diagnosis (in 2007-2013) were more likely to be presented with advanced HIV disease among adults aged 19-34 years. These results are partially consistent with those of previous studies on HIV-infected subjects; however, we found that the factors affecting late-stage presentation differed by age group (348). It is thought that in Korea, the numbers of undiagnosed HIV patients are larger than those of diagnosed patients (16). In addition, the proportion of advanced-stage HIV patients among newly diagnosed patients is increasing year by year (348), implying that the real numbers of HIV patients and the proportions of missed diagnoses are increasing much faster than the official statistics indicate. The fact that late-stage presentation was common among young adults diagnosed with HIV from 2007-2013 is a direct result of the epidemiological features mentioned above. If many HIV-infected subjects are not diagnosed in early stage of HIV infection, most will eventually be diagnosed in later life. This partially explains the finding that presentation with advanced HIV disease was common in those of older age. In addition, old subjects are less likely to request HIV testing, because they lack relevant knowledge and exhibit antipathy toward those who have HIV/AIDS (17). Being knowledgeable about HIV testing is associated with a willingness to undergo testing (18), and lack of information on HIV testing may be more common in old subjects (19).
Of adults aged 35-49 years, presentation with advanced HIV disease was associated with HIV testing during health check-ups and with development of clinical manifestations. In Korea, most HIV tests are performed in hospitals during routine health check-ups and as components of medical procedures unrelated to HIV infection; many individuals were diagnosed at the late stages of HIV infection (4). In other words, HIV-infected subjects who had been unaware of their serological status for a long time were diagnosed when they requested health check-ups or when clinical manifestations appeared.
We found that the risk of presentation with advanced HIV disease was lower among adults aged ≥50 years and in those diagnosed with HIV in the period 2000-2006. We cannot explain this finding in detail. However, the proportion of adults over 50 years of age seeking general health check-ups was higher in 2000-2006 compared with other periods for which data are available. We presume that old adults requesting general health check-ups are more likely to have their HIV status assessed.
This study has several limitations. First, we evaluated only HIV-infected adults living in Seoul, and our data may thus not be generalizable to Korea as a whole. However, the demographic and epidemiological characteristics of our study sample were similar to those of the National HIV Surveillance Survey. Second, our data on HIV exposure categories may be somewhat unreliable; study participants may not have disclosed their sexual preferences. However, the proportion of MSM (men who have sex with men - including bisexuals) was high compared with that of the national HIV surveillance study, suggesting that subjects answered our questions more frankly than those participating in the national survey (34). Third, we did not include data on the clinical features of AIDS or the nature of AIDS-defining illnesses present at the time of HIV diagnosis. Subjects with AIDS are more likely to request HIV tests. Thus, separation of subjects into late and not-late presenters may be associated with an element of bias.
Despite these limitations, we used city-wide representative samples to identify factors influencing the presentation with advanced HIV disease. The influence of age group on such presentations has not been assessed previously. Identification of such epidemiological features facilitates the development of effective strategies for early diagnosis of HIV infection.
In conclusion, the factors associated with presentation with advanced HIV disease differed by age group. Lower educational level in younger subjects and more advanced age in older subjects had a positive influence on presentation with advanced HIV.
 XML Download
XML Download