

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Ebstein anomaly (EA) is a rare congenital heart malformation characterized by downward displacement of tricuspid valve leaflets into the right ventricle. It results “atrialization” of the proximal portion of the right ventricle (123). A wide spectrum of symptoms may present due to various degree of tricuspid regurgitation, right to left shunt by atrial septal defect, right ventricular dysfunction and arrhythmias (4). The clinical features and age at presentation are various with the severity of apical displacement of tricuspid annulus and associated anomalies (125).
Patients with mild EA can survive life-long without surgical intervention, but many patients need an operation eventually. In children, the surgery is recommended if the patient has severe dyspnea, cyanosis, paradoxical embolization, cardiomegaly or recurrent arrhythmia (6). However, adult patients often carries mild symptoms that results in a delay of the optimal timing of corrective surgery, which leads the patient’s condition to deteriorate with increasing risk of surgery, post-op arrhythmia and ventricular dysfunction. Yet, optimal timing and type of surgical intervention in the older patients remains unclear, specific criteria needs to be defined (789).
The objectives of this study were to assess the clinical outcomes of adults with EA who underwent medical or surgical therapeutic strategy and to compare outcomes of medical treatment, immediate surgical and delayed surgical intervention.
MATERIALS AND METHODS
Study design and patients
This is a single center retrospective study. We evaluated EA patients diagnosed at Samsung Medical Center (Seoul, Korea) between October 1994 and October 2014. The diagnosis of EA was based on apical displacement of septal tricuspid leaflet of > 8 mm/m2 body surface area from the AV valve ring measured in apical four chamber view on transthoracic echocardiography (TTE) (151011). Among them, patients with their age ≥ 18 years at the diagnosis were included in this study. Patients who underwent previous cardiac surgical intervention at their age ≥ 18 years also were included in this study. Patients who had combined complex anomaly such as transposition of the great arteries were excluded.
Patients were categorized into 3 groups according to their involved treatment strategy and timing of surgical intervention based on 6 months after diagnosis: non-operative (Group I), immediate operative (Group II) and delayed operative (Group III).
Data collection
Baseline clinical, electrocardiographic and echocardiographic data were obtained retrospectively from medical record. Demographic and clinical data included age at diagnosis, sex, associated anomaly, initial presentations, detailed surgical methods. From the modified Simpson’s method using two-dimensional transthoracic echocardiography (2D TTE), left ventricular functions were defined as normal (ejection fraction, EF ≥ 55%), mildly impaired (EF 45%–54%), moderately impaired (EF 30%–44%) or severely impaired (EF < 30%). Right ventricular function was qualitatively graded as normal or impaired by measuring of tricuspid annular plane systolic excursion (TAPSE), systolic tricuspid annular velocity (S') or right ventricular fractional area change (RVFAC) using the 2D TTE. Tricuspid regurgitation (TR) was assessed as mild, moderate or severe. Pulmonary hypertension as defined as estimated right ventricular systolic pressure > 40 mmHg by echocardiographic evaluation using simplified Bernoulli equation (1213). The cardiothoracic ratio (CTR) was measured in the initial chest radiograph and cardiomegaly was defined as CTR > 0.55 (1415).
Primary outcome
The primary outcome of this study was a composite of major adverse cardiac and cerebrovascular events (MACCE) defined as death, repeated surgery, re-hospitalization due to heart failure, myocardial infarction, stroke or major arrhythmias requiring treatment. Major arrhythmias include sustained ventricular tachycardia, ventricular fibrillation, advanced atrioventricular block and atrial fibrillation/flutter. For operative groups (Group II and III), MACCE were investigated only after operation.
Statistical analysis
Categorical variables were presented as frequencies and percentages. The χ2 test or Fisher’s exact test was performed appropriately to test the difference of categorical variables between three groups. Continuous variables were presented as mean ± standard deviations. Kruskal-Wallis test was performed to test the difference of continuous variables between three groups. The probability of freedom from MACCE of each groups were estimated by the Kaplan-Meier method and log-rank test. P values < 0.05 were considered as significant. In order to adjust for baseline characteristics when examining differences in outcomes among 3 groups, multivariable Cox proportional hazard regression analysis was performed. Data ware analyzed using SPSS statistical software (version 20.0 for Windows, SPSS, Inc., Chicago, IL, USA).
RESULTS
Study population and Baseline clinical characteristics
From October 1, 1994 to December 31, 2014, there were 60 adult patients with EA included in this study; 19 (31.7%) men and 41 (68.3%) women with the median age at diagnosis as 37 years (range, 18 years to 71 years). During the follow-up period with median follow-up duration of 38.9 months (range 0 to 229.4 months), 37 patients (61.7%) underwent surgical intervention in our institution. There were 23 patients in Group I, 27 in Group II, and 10 in Group III. Six patients had delayed operation despite recommendations from physician. Others underwent delayed operation because of progression of exertional dyspnea (n = 4), palpitations with dizziness or syncope (n = 3), stroke due to paradoxical embolization (n = 1), cyanosis with polycythemia (n = 1) and aggravated dyspnea due to combined coronary artery disease (n = 1).
The baseline characteristics of the each group were described in detail in Table 1. The clinical characteristics among the three groups were similar, but New York Heart Association (NYHA) functional class, TR grade, pulmonary hypertension and Right bundle branch block (RBBB) showed significant differences (Table 1).
Table 1
Distribution of baseline characteristics, clinical parameters, associated anomaly and clinical outcomes classified by treatment strategy (n = 60)

ASD = atrial septal defect, AV block = atrioventricular block, CTR = cardiothoracic ratio, CXR = chest X-ray, FU = follow up, HF = heart failure, Hx. = history, LA = left atrium, LV = left ventricle, MACCE = major adverse cardiovascular and cerebrovascular events, MI = myocardial infarction, NT-proBNP = N-terminal prohormone of brain natriuretic peptide, NYHA = New York Heart Association functional class, op. = operation, PFO = patent foramen ovale, PPM = permanent pacemaker, PSVT = paroxysmal supraventricular tachycardia, RBBB = right bundle branch block, RVFAC = right ventricular fractional area change, VF = ventricular fibrillation, VSD = ventricular septal defect, VT = ventricular tachycardia.
*Kruskal-Wallis or χ2-test for Non-op. vs. Immediate op. vs. Delayed op.; P value was calculated by Kruskal-Wallis test and Bonferroni multiple comparisons tests for continuous variables (P value < 0.05).
Clinical outcomes
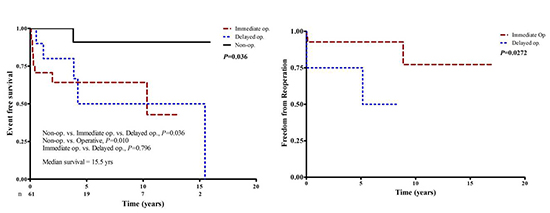
During the study period, MACCE occurred in 3 (13.0%) patients in Group I, 15 (55.6%) patients in Group II and 5 (50%) in Group III (Table 1). Overall event free survival was 64.6%, 46.3% and 26.5% at 5, 10 and 15 years, respectively. Event free survivals at 5 years were 90% in Group I, 52.7% in Group II, 50.0% in Group III. Kaplan-Meier event-free survival curves for MACCE among the three groups were statistically different (P = 0.011) (Fig. 1). In subgroup analysis, there was no significant difference between Group II and Group III (P = 0.274), however, Group I had better event free survivals than operative groups (P = 0.007).
Fig. 1
Cumulative Event free survival curves stratified by 3 treatment strategy groups. Event free survival for MACCE was not significantly different between immediate operative group and delayed operative group but it showed significant difference between overall surgical treatment group and medical treatment group (immediate op. vs. delayed op.: P = 0.274, non-operative vs. operative: P = 0.007).
MACCE = major adverse cardiovascular and cerebrovascular events, op. = operation.

Follow-up RV dysfunction (hazard ratio [HR], 3.63; 95% confidence interval [CI], 1.21–10.9), Kang pulmonary hypertension (HR, 3.23; CI, 1.36–7.68; P = 0.008) and cardiomegaly, CTR > 55% (HR, 3.20; CI, 1.15–8.87; P = 0.025) were demonstrated as significant predictors for MACCE in the univariate Cox proportional hazard regression analysis, but not in the multivariate analysis HR, 1.41 (CI, 0.41–4.79), HR 0.98 (CI, 0.28–3.39) and HR 0.93 (CI, 0.19–4.57), respectively (Table 2). However, immediate operative treatment strategy (HR, 6.39; CI, 1.21–33.7; P = 0.029) and ASD/PFO (HR, 3.57; CI, 1.02–12.6; P = 0.047) were independent predictors for MACCE in both of the univariate and the multiple Cox proportional hazard regression analysis.
Table 2
Univariate and multiple analysis for proportional hazard of adults with Ebstein anomaly for MACCE (major adverse cardiovascular and cerebrovascular events)
HR = hazard ratio, CI = confidence interval, ASD = atrial septal defect, CTR = cardiothoracic ratio, CXR = chest X-ray, FU = follow up, op. = operation, RBBB = right bundle branch block, RV = right ventricle, RVFAC = right ventricular fractional area change, LV = left ventricle, PFO = patent foramen ovale.
Arrhythmia
Among the total of 60 patients, 23 (38.3%) patients complained of palpitation at the time of diagnosis and 18 (30.0%) patients had major arrhythmic events during follow-up period. Documented tachyarrhythmia during follow-up were atrial fibrillation/flutter (n = 10), ventricular tachycardia (n = 3) and supraventricular tachycardia (n = 3). PPM implantation was performed due to high degree AV block for 3 patients, 1 in non-operative and 2 in delayed operative group.
Surgical ablation was performed for 20 patients; 15 (55.5%) patients of Group II and 5 (50%) patients of Group III. However, major arrhythmic events occurred more frequently in patients underwent surgical ablation; and the difference was statistically significant (surgical ablation vs. no surgical ablation, 10 [50.0%] vs. 8 [20.0%]; P = 0.034).
Death
During the follow-up period, there were two cardiac deaths. A 30 year-old women died early post-operatively of ventricular tachycardia and subsequent brain death complicated with extracorporeal membrane oxygenation (ECMO) after undergoing TAP (modified DeVega type), atrial septal defect (ASD) patch closure and Maze operation. A 65 year-old man in Group I died after 8 years from the diagnosis because of uncompensated heart failure and cardiac liver cirrhosis.
Heart failure
During the follow-up period, MACCE occurred in 23 patients, including 4 events of re-hospitalization due to heart failure, which were found only in the Group II (immediate operative). Interestingly, patients in Group II were more likely to assigned to NYHA functional class II and III compared to other groups and had severe tricuspid regurgitation and pulmonary hypertension and RBBB on baseline echocardiographic and electrocardiographic study.
DISCUSSION
Our study examined the early and long-term outcomes in adult patients with EA and evaluated outcomes according to their involved treatment strategy: non-operative treatment, immediate surgical and delayed surgical intervention. Event free survival rates were significantly different among 3 groups classified by their involved therapeutic approaches. Considering that the baseline characteristics of initially operative group and un-operative group were statistically different, treatment strategy should be different.
There are severe studies reporting the outcome and natural history of EA. Celermajer et al. (4) demonstrated survival for all live-born patients as 67% at 1 year and 59% at 10 years. However, they included fetal and neonatal subjects. In other study by Attie et al. (16), survival of un-operated adults were 89% at 1 year and 76% at 10 years. Elsewise, Attenhofer et al. (10) demonstrated post-operative outcome of patients older than 50 years of age. The survival was 71% at 10 years and 65% at 20 years.
The event free survival of our study is relatively lower than other studies because we included significant arrhythmic events in MACCE. Atrial fibrillation/flutter and supraventricular tachycardia were most frequently occurred significant arrhythmia. Interestingly, major arrhythmic events occurred frequently even after surgical ablation. Thus, the ablative procedure for arrhythmia in EA might have worse outcome than that of arrhythmias associated with other cardiac disease. It could be explained from that there were often multiple arrhythmias in a patient with EA and catheter ablation were also difficult in EA. Also, long period of stress on atrial wall would make it more arrhythmogenic in adults (17). Therefore careful intensive medical treatment and frequent follow-up would be required for EA patients even after surgical ablative procedures.
In our study, moderate to severe tricuspid regurgitation as well as pulmonary hypertension (PHT) and right bundle branch block were more frequently observed in Group II compared to Group I. Unsurprisingly, more patients in Group II were assigned to NYHA functional class III. Most patients with RV dysfunction developed progression of symptoms although they did not have any significant symptoms before, and eventually proceeded to undergo emergent surgery. These findings corresponded well to several established indications for surgery (2781819). Therefore attentive risk stratification with echocardiographic evaluation should be recommended for patients with TR, PHT and RV dysfunction.
Several studies have reported on prognostic value of severity of tricuspid regurgitation. Attie et al. (16) reported clinical outcome in 72 un-operated adult patients. Cardiomegaly, male sex, NYHA class III or IV, cyanosis, severe TR and early age at diagnosis were suggested for long-term predictors of cardiac death via univariate analysis. However these variables were not demonstrated to be clinical correlates in Cox regression model. In other studies, several variables, such as residual right ventricular function, left ventricular function, associated cardiac anomaly and cardiomegaly were demonstrated to be associated with the risk of cardiac death (42021). In current study, RV dysfunction, presence of pulmonary hypertension and presence of cardiomegaly on initial evaluation appeared as predictors for MACCE, but not in the multivariate analysis. Cyanosis was thought to be significant clinical predictor of EA especially in neonates, but it was not associated with the overall outcome in study with adult patients (22). Similarly in the current study, cyanosis was not shown to be a reliable predictor for MACCE. Instead, presence of ASD or PFO appeared to be significant independent predictors for MACCE. It suggests that the presence of ASD or PFO might have clinical significance for themselves, even without significant R to L intracardiac shunt to cause cyanosis.
In addition, our study demonstrated lower freedom from reoperation in Group III compared to Group II (75% vs. 92.7% at 5 years, P = 0.027). Most patients in Group III underwent urgent surgery because of progressive aggravation of clinical status, and it could be possible explanation for higher reoperation rate.
There are a number of strengths and limitations of this study. In this study, we demonstrated long-term clinical outcome of adults with Ebstein anomaly according to their involved treatment strategy. Taking into account of the fact that the patients who received surgery were a higher risk group than those with medical treatment, comparison of clinical outcome among each treatment group could not suggest which treatment strategy would be better. Instead, current study might give us an insight about clinical outcome when current treatment guideline applied to adult patients. There are few studies of long term outcome with or without surgery for adult patients with EA. In addition, differences in surgical techniques may have influenced on clinical outcome. However, this effect could be minimized considering the fact that all the surgeries were performed in one center by two surgeons. Lastly, only small number of patients had clinical event in current study even with 10 years’ period. It resulted in limited study power, therefore, it requires multicenter trial to have more robust results.
Considering all of above, decision of treatment strategy according to current indication appears to be reasonable in adult patients with Ebstein anomaly. However, the outcome of surgical ablation for arrhythmia appeared to be not enough so that concomitant medical treatment may be considered even in patients underwent antiarrhythmic operation. In addition, more earlier and active treatment strategy should be considered because delayed operation needed more reoperation.
 XML Download
XML Download