

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Intensity-modulated radiation therapy (IMRT) and volumetric-modulated arc therapy (VMAT) treatments utilizing a linear accelerator (LINAC) with dynamic multileaf collimators (MLCs) are extremely complex for both treatment planning and delivery. In the newest VMAT technique, the beam aperture rotating on a gantry changes continuously and dose rate and gantry speed can also be varied (1). The technique is widely used in the treatment of carcinomas in various sites of cancer, including head and neck, lung, prostate, and rectum.
To ensure accurate radiation delivery before IMRT and VMAT treatments, pretreatment verification prior to clinical implementation must be adequately tested in the form of delivery quality assurance (DQA) to identify any potential errors in the treatment planning process and in machine deliverability (23). Various two-dimensional (2D) array quality assurance (QA) systems have been used for DQA of IMRT and VMAT in previous researches (45678).
Recently, the TrueBeamⓇ STx accelerator (Varian Medical Systems, Palo Alto, CA, USA) with flattening-filter (FF) and flattening-filter-free (FFF) beams was introduced in clinical operations. Removing the flattening filter has two advantages: first, fast delivery time because of the increased dose rates that allows faster beam delivery in stereotactic body radiotherapy (SBRT) with higher-fraction doses and second, reduction of the out-of-field dose as a result of reduced head scatter and leakage, which leads to reduced exposure of normal tissue to scattered doses outside the target field (9101112).
There is an increasing interest in SBRT-VMAT using FFF beams because of the improved delivery efficiency and reduced treatment time with comparable dose distribution to conventional FF beams (1314). Most of previous studies are published on DQA of IMRT and VMAT using FF beams (1516). The multicenter studies provided the comparison of pretreatment DQA data for various QA systems.
In this study, pretreatment verification was evaluated with different 2D QA systems (film, I’mRT MatriXX, and MapCHECK) based on the SBRT-VMAT plan using FFF beams for various treatment sites. The aim of this study was to compare the gamma agreement of the commercial QA systems for the pretreatment plan of the SBRT-VMAT technique using FFF beams.
MATERIALS AND METHODS
Stereotactic body radiotherapy planning
For this retrospective study, we selected 20 patients having different disease cancers (seven lung, six spine, and seven prostate cancers) that had previously been treated in our department from September 2013 to December 2015. All SBRT treatment plans were generated using the Eclipse™ treatment planning system Ver. 11.0.34 (TPS, Varian Medical Systems). Table 1 shows the characteristics of the SBRT-VMAT plans for all patients. Depending on the plan, 6 and 10 MV FFF beams were used. Dose computations were calculated using Acuros XB (AXB, version 11) and 2.5 mm isotropic dose grid. For the SBRT-VMAT plan of each case, one or two arcs were used in treatment planning. The verification plans were created using the actual planned gantry and collimator angles, included the treatment couch. All verification plans were delivered on a Varian TrueBeamⓇ accelerator equipped with a high-definition multileaf collimator (HD MLC; 2.5 mm central 32 leaf pairs spanning 8 cm and 5.0 mm leaf pairs in the periphery). To clarity the dependency of DQA result on the different QA systems, the verification of pretreatment was carried out using three QA systems for the same patient plan. Here we made pretreatment plans using identical beam setup and same number of MU as in the treatment plans. All CT data for pretreatment plan were acquired at 0.2 cm slice spacing using orthopedic metal artifact reduction function (O-MAR) to remove the metal artifact in 2D QA systems such as I’mRT MatriXX and MapCHECK.
Table 1
Characteristics of SBRT-VMAT plans for 20 patients
![]()
Quality assurance systems
EBT3 film dosimetry using home-made cylindrical phantom
A film of dimension 20 × 25.4 cm2 (Gafchromic EBT3; ISP, Ashland) was used in a custom in-house built cylindrical acrylic phantom to measure the axial plane, as shown in Fig. 1A. For film dosimetry, a net-optical density (netOD) curve for the 6-MV FFF beam obtained in a 10 × 10 cm2 field. Doses ranging from 0 to 15 Gy were used to convert the film optical density to dose from the same film batch. All films were processed and analyzed after irradiated least 24 hours. Films were scanned using a flatbed scanner (Epson Expression 11000 XL, Epson America Inc., Long Beach, CA, USA) with a 75 dpi resolution for analyzing the measured central axis dose and dose distribution. The Radiological Imaging Technology 113 software (Ver. 6.4, Colorado Springs, CO, USA) was used to analysis dose distributions for the measured films.

I’mRT MatriXX array using MultiCube phantom
The ion chamber array (I’mRT MatriXX array; IBA dosimetry, GmbH, Schwarzenbruck, Germany) system contained 1,024 parallel-plate ion chambers arranged in a 32 × 32 grid with 7.5 mm of separation between the centers of the adjacent chambers. Each ion chamber has a diameter, height, and volume of 4.5 mm, 5.0 mm, and 0.08 mL, respectively, with an equivalent water thickness on the front side of the detectors of 3.6 mm. The bias voltage and sampling time required for the 2D array system are 500 ± 30 V and 500 ms, respectively, which is set by the manufacturer. The 2D array system underwent a 30-min warm-up time before each measurement. The system was calibrated based on the measurement values obtained from the four center chambers of the 2D array system for the absolute dose measurements according to the manufacturer recommended procedures (1718). All verification plans were delivered to the MatriXX, which was inserted into the MultiCube (31.4 × 34 × 34 cm3) virtual water phantom. shows the setup of the I’mRT MatriXX system using a MultiCube phantom for measuring verification plans.
MapCHECK array using MapPHAN phantom
The diode array (MapCHECK) system consists of 445 N-type solid-state diodes that are in a 22 × 22 cm2 2D array. The inner 221 diodes cover the central 10 × 10 cm2 that are arranged in a zigzag pattern so that the diagonal spacing between diodes is 0.707 cm (1920). In addition, the outer 224 detectors are arranged in a similar pattern, but with a diagonal spacing between diodes of 1.414 cm. The active area of each diode is 0.8 × 0.8 cm2. The MapPHAN (10 cm in thickness), along with the MapCHECK, was scanned on a Brilliance Big Bore CT scanner (Philips Medical Systems, Cleveland, OH, USA) with a slice thickness of 2 mm and transferred to the Eclipse treatment planning system (TPS) for verification planning. All verification plans were delivered to the MapCHECK, which was inserted into the MapPHAN (30 × 31 × 10 cm) phantom. Fig. 1C shows set up of the MapCHECK system using the MapPHAN phantom for measuring verification plans.
Gamma agreement analysis
To quantify the differences between the calculated and measured dose distributions, we performed the gamma analysis to determine the agreement scores using a 2% dose differences and a 2 mm distance to agreement (denoted as “2%/2 mm”, from now on) as well as 3%/3 mm for the criteria. The pixels (threshold value: 10) that received less than 10% of the maximum dose were not considered from the gamma evaluation. Each arc for all plans was analyzed separately and the average value was obtained. The passing rate via gamma analysis was calculated with gamma points less than 1 (γ < 1) that indicates that the points lie within the dose value difference and distance to agreement passing criteria.
RESULTS
Pretreatment plans were presented to verify the SBRT treatment plan using FFF beams for three treatment sites. For the SBRT-VMAT plans with prescription dose of 6.1–12 Gy per fraction, the monitor units and the dose rate were scaled down for all DQA measurements for accurate measurement without saturating the dose of the three QA systems. Fig. 2 shows examples of gamma evaluation results for the three 2D QA systems i.e., Film, I’mRT MatriXX, and MapCHECK. A summary of the passing rate via gamma analysis between the three QA systems is shown in Table 2 for both criteria of 2%/2 mm and 3%/3 mm. The mean and standard deviation of the passing rate for all the QA systems were 93.4% ± 2.5% for the 2%/2 mm criteria and 97.9% ± 1.7% for the 3%/3 mm criteria, respectively. Table 3 and 4 indicate the mean and standard deviation of the passing rate on all the QA systems for delivery beam energy and treatment site as the determined mean passing rates based on the gamma evaluation is relative to the calculated dose distribution by TPS. All treatment sites and QA systems showed comparatively good mean passing rates for the 3%/3 mm criteria, while a slightly lower passing rate is observed for the 2%/2 mm criteria. However, the mean passing rate achieved an acceptable passing rate of at least 90% in all pixels for all treatment sites and QA systems. For the 3%/3 mm criteria, similar results between the three QA systems were observed. For the film, the passing rate ranged from 95.8% to 99.5% and the mean passing rate was 96.6%. For the MatriXX system, the passing rate ranged from 97.1 to 100% and the mean passing rate was 98.2%. For the MapCHECK system, the passing rate ranged from 97.9% to 100% and the mean passing rate was 98.9%
 | Fig. 2Example of gamma evaluation results between the three QA systems and TPS. The measured dose distribution, the calculated dose distribution and the gamma evaluation image for (A) EBT3 film, (B) I’mRT MatriXX, and (C) MapCHECK.
|
Table 3
Mean and standard deviation of passing rate via gamma analysis between the three 2D QA systems and the TPS for three treatment sites

![]()
Table 4
Mean and standard deviation of passing rate via gamma analysis between the three 2D QA systems and the TPS for both delivery beam energies

![]()
For each treatment site, the mean and standard deviation passing rate of the film was 92.9% ± 2.1%, 94.0% ± 1.8%, and 93.2% ± 1.4% on the lung, spine, and prostate cancer cases, respectively, for the 2%/2 mm criteria. The corresponding values for the 3%/3 mm criteria were 97.5% ± 17%, 98.3% ± 1.2%, and 97.8% ± 1.2% on the lung, spine, and prostate cancer cases, respectively. The mean passing rate for the 2%/2 mm criteria are lower than that for the 3%/3 mm criteria on all the treatment sites. Furthermore, the spine cancer cases had the highest mean passing rate, while the lung cancer cases had the lowest mean passing rate.
For both delivery energies, there is no consistently correlation between the mean passing rate and delivery energy. The highest passing rate (99.1% for 3%/3 mm) was observed on the MapCHECK system for a 6-MV FFF beam. The lowest passing rate was obtained on film for a 6-MV FFF beam.
DISCUSSION
Many studies were performed for performance comparison of the different commercial QA systems and sensitivity assessment for IMRT and VMAT treatments (212223242526272829), but few studies are performed on the performance comparison for the SBRT-VMAT treatment using FFF beams (1316). In this study, the various QA systems such as MapCHECK, I’mRT MatriXX, and EBT3 film were used to verify the delivery of SBRT-VMAT treatment plans using FFF beams. To quantify the performance of MapCHECK and I’mRT MatriXX system, the basic dosimetric tests with different field size and various dose rates were carried out. The gamma passing rates of both systems for 5 × 5 cm2 and 10 × 10 cm2 static field of 6-MV FFF beam were found to be independent for dose rates between 400 MU/min to 1400 MU/min as shown in Fig. 3. These results were comparable with those of nominal beam reported in the previous study (30).
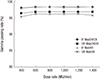 | Fig. 3Gamma passing rate of MapCHECK and MatriXX for static field of 6-MV FFF beam with various dose rates and different field sizes.
|
Dosimetric verification results for the QA systems were different. For the 2%/2 mm and 3%/3 mm criteria, the passing rates of gamma analysis for the MapCHECK system were higher than those of film and MatriXX system. However, the passing rates between MapCHECK and MatriXX system has a smaller difference (within 2%). The lowest passing rate was recorded on film measurement. The passing rate of the film system was decreased by approximately 2% to 5% as compared to that of other systems (Table 2). This is because the QA systems used for the measurements had different resolutions. The previous studies on comparison between film measurement and the different QA systems reported similar results as that of our study (1531). They reported that from an average passing rate three dosimetric methods, such as MapCHECK, I’mRT MatriXX, and electron portal imaging device (EPID), show slightly better agreement between the calculated and measured doses than the film.
Table 2
Mean passing rate via gamma analysis between the three 2D QA systems for the 2%/ 2 mm and 3%/ 3 mm criteria

![]()
In general, film dosimetry is a well-established method for verifying SBRT-VMAT dose distributions with small fields due to its high spatial resolution. Therefore, the passing rate based on film measurement was a little lower than that of other 2D array QA systems, such as MapCHECK and MatriXX. Furthermore, the film dosimetry is a time- and material-consuming method that requires well-controlled calibration. It depends on photon energy and dose rate as well as the daily output variation. In contrast, these 2D QA systems provide an improved efficiency with minimal calibration process and user friendly applications for pretreatment verification. In addition, the 2D QA systems could perform daily output correction before measurements.
Prior to the QA systems measurements, we performed the pretreatment verification after checking routine dynamic MLC quality control using the EPID to improve accuracy. The MLC tests include the picket fence, weeping gap, and MLC speed test. Previously, Vieillevigne et al. (1) reported that dose distributions were more sensitive to MLC errors than to collimator, couch, or gantry errors.
We also evaluated the results of pretreatment verification for three treatment sites. The highest mean passing rate (95.9% for the 2%/2 mm criteria) was observed on the MapCHECK system for the spinal cancer case, whereas the lowest mean passing rate (90.2% for the 2%/2 mm criteria) was observed on the film for the lung case, which included the different density media. Compared to spinal and prostate cancer, lung cancer included the heterogeneous tissue, such as air cavity and low-density lung tissue. The heterogeneous region is one of the factors which influence an uncertainty of the dose computation. It required complex beam modulation for proper target coverage and normal tissue sparing. We used AXB algorithm to perform accurate dose calculation. However, it caused increment of the gamma disagreement in the region, because measured dose was much affected with geometric error by sensitivity of its algorithm.
Current study limitation is that there are no dose volume histograms (DVH) based on QA data associated with a gamma analysis. This study focused mainly on ability test of different commercial QA systems in SBRT-VMAT pretreatment using FFF beams. Therefore, in the future, a gamma method specific for structure are required to evaluate the clinically relevant DVH based QA for SBRT-VMAT.
In conclusion, the pretreatment verification of the SBRT-VMAT for the different treatment sites was evaluated using different QA systems. Overall, this study confirmed that all the QA systems perform well in terms of delivery errors. However, the film measurement had the lowest passing rate among all the QA systems. As it is a time- and material-consuming method, it requires well-controlled calibration. However, excellent agreement (more than 90%) between the measured and calculated dose distributions for the both criteria was evident for all QA systems. Therefore, the results of this study suggest that the three commercial QA systems are reliable verification systems for SBRT-VMAT pretreatment.
 XML Download
XML Download