

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Lung cancer is the most common cause of cancer-related mortality worldwide (1). The best available prognostic index for non-small cell lung cancer (NSCLC) is the TNM staging. However, there are wide variations in prognosis within the same stage group. This indicates that other factors may account for prognostic heterogeneity.
Angiogenesis is crucial for development, growth, and metastasis of tumors and a variety of growth factors have been shown to stimulate tumor angiogenesis (2). Among them, vascular endothelial growth factor (VEGF) is the most important mediator of angiogenesis. High VEGF expression has been associated with poor prognosis in many cancers (345). In NSCLC, higher VEGF expression was reported in tumor tissue than their adjacent normal lung tissue (67), and high VEGF expression has been closely associated with poor survival outcome after surgery (68910). In these studies (67), tumoral VEGF expression level was different according to histology: adenocarcinomas (ACs) showed higher VEGF expression than squamous cell carcinomas (SCCs).
VEGF expression may be influenced by single nucleotide polymorphisms (SNPs) in VEGF gene. Several studies have reported the association between VEGF polymorphisms and survival outcomes in various carcinomas including NSCLC, and suggested that DNA sequence variations in VEGF may modulate the prognosis of tumors by altering VEGF expression (111213). Among the potentially functional VEGF SNPs, the rs833061 T>C, rs2010963G>C, and rs3025039C>T are important polymorphisms located in the promotor region, 5′-untranslated region, and 3′-untranslated region, respectively, and have been most commonly investigated in relation to lung cancer prognosis (141516). However, there were no clear conclusions due to inconsistent results in each study.
Hypoxia is a common feature in most of the solid tumors including lung cancer, and hypoxic condition is the most important stimulating factor for the expression of VEGF (171819). Eilertsen et al. (20) reported that AC and SCC of the lung exhibited different VEGF response to hypoxia. In AC, VEGF expression was significantly higher in hypoxic condition compared to normoxic condition. In contrast, SCC showed no significant change of VEGF expression in response to hypoxia. Difference in VEGF expression between SCC and AC of the lung suggests that VEGF may exert differential effect on the prognosis of SCC and AC. Therefore, it is possible that VEGF polymorphisms may affect the prognosis of NSCLC differentially depending on tumor histology. Nevertheless, no studies have categorized tumor histology when evaluating this relationship.
In the current study, we analyzed the association between the three VEGF SNPs (rs833061 T>C, rs2010963G>C, and rs3025039C>T) and survival outcome of surgically resected NSCLC patients. In addition, we evaluated the effect of VEGF SNPs on the prognosis of NSCLC patients according to tumor histology.
MATERIALS AND METHODS
Study population
This study included 782 patients with stage I, II, or IIIA NSCLC who underwent surgical resection; 354 patients at Kyungpook National University Hospital (KNUH, Daegu, Republic of Korea) from December 1997 to January 2010 and 428 patients at Seoul National University Hospital (Seoul, Korea) from June 2006 to May 2012. The histologic types of lung cancers were as follows: 341 SCCs (43.6%), 425 ACs (54.3%) and 16 large cell carcinomas (2%). The pathologic staging of the tumors, which was determined according to the International System for Staging Lung Cancer (21), was as follows: stage I (n = 378, 48.3%) and stage II + IIIA (n = 404, 51.6%). All of the patients included in this study were ethnic Koreans.
VEGF genotyping
The three SNPs (rs833061T>C, rs2010963G>C, and rs3025039C>T) were genotyped using a polymerase chain reaction (PCR)-restriction fragment length polymorphism assay. The primer sequences and annealing temperature for the PCR analysis and the restriction enzymes are shown in Supplementary Table 1. Genotyping analysis was performed blind with respect to the subjects. Approximately 5% of the samples were randomly selected to be genotyped again by a different investigator, and the results were found to be 100% concordant.
Statistical analysis
Demographic and clinical information were compared using chi-square tests for categorical variables. The Hardy-Weinberg equilibrium was tested by comparing the observed and expected genotype frequencies using a goodness-of-fit χ2 test. The primary outcomes used for the present study were overall survival (OS) and disease-free survival (DFS). OS was measured from the day of surgery until the date of death or to the date of the last follow-up. DFS was calculated from the day of surgery until recurrence or death from any cause. The differences in OS and DFS across different genotypes were compared using the log-rank test. Hazard ratios (HRs), 95% confidence intervals (CIs) and corresponding P values were calculated using multivariate Cox proportional hazard models, adjusted for age (≤ 65 years vs. > 65 years), gender (female vs. male), smoking status (never-smokers vs. ever-smoker), tumor histology (squamous vs. non-squamous), pathologic stage (I vs. II-IIIA), and adjuvant therapy (yes vs. no). A homogeneity test was performed to compare the difference between genotype-related HRs of the different group. All analyses were performed using Statistical Analysis System for Windows, version 9.2 (SAS Institute, Cary, NC, USA).
RESULTS
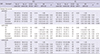
The clinical and pathologic characteristics of the patients and their association with OS and DFS are shown in Table 1. There were total 208 deaths (26.5%) and the estimated 5-year OS and DFS for all patients were 62% (95% CI = 0.57–0.68) and 45% (95% CI = 0.40–0.49), respectively. Pathologic stage was significantly associated with both OS and DFS. Age, gender and smoking status were significantly associated with OS, but not with DFS in univariate analysis. There were no significant differences in survival outcome by histologic type and adjuvant therapy.
Table 1
Univariate analysis for overall survival and disease-free survival by age, gender, smoking status, histological type, pathologic stage, and adjuvant therapy
*Row percentage; †Five year-overall survival rate (5Y-OSR) and 5 year-disease free survival rate (5Y-DFSR), proportion of survival derived from Kaplan-Meier analysis; ‡In ever-smokers; §In pathologic stage II + IIIA : 182 cases received p aclitaxel-cisplatin, 11 cases received radiotherapy, and 27 cases received chemotherapy and radiotherapy.
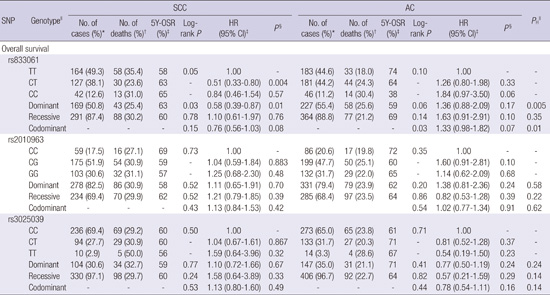
In overall patients’ analyses, the rs833061T>C, rs2010963G>C, and rs3025039C>T were not significantly associated with OS and DFS (Table 2). Interestingly, however, when the patients were stratified by tumor histology, the rs833061 T>C had a significantly different effect on survival outcomes between SCC and AC (Tables 3 and 4). The rs833061 T>C was associated with better OS in SCC and worse OS in AC under a codominant model, although marginally significant (adjusted HR [aHR] = 0.76, 95% CI = 0.56–1.03 in SCC; aHR = 1.33, 95% CI = 0.98–1.82 in AC; P for heterogeneity = 0.01). In addition, the rs833061T>C was significantly associated with better DFS in SCC and worse DFS in AC under a codominant model (aHR = 0.75, 95% CI = 0.58–0.97 in SCC; aHR = 1.26, 95% CI = 1.00–1.60 in AC; P for heterogeneity = 0.004).
Table 2
Overall survival and disease-free survival according to genotypes in patients with non-small cell lung cancer
SNP = single nucleotide polymorphism
*Column percentage; †Row percentage; ‡Five year-overall survival rate (5Y-OSR) and 5 year-disease free survival rate (5Y-DFSR), proportion of survival derived from Kaplan-Meier analysis; §Hazard ratios (HRs), 95% confidence intervals (CIs) and corresponding P values were calculated using multivariate Cox proportional hazard models, adjusted for age, gender, smoking status, tumor histology, pathologic stage and adjuvant therapy; ∥Genotype failure: 23 cases for the rs833061, 12 cases for the rs2010963 and 6 cases for the rs3025039.
Table 3
Overall Survival according to the rs833061, rs2010963 and rs3025039 genotypes by tumor histology
SNP = single nucleotide polymorphism, SCC = squamous cell carcinoma, AC = adenocarcinoma.
*Column percentage; †Row percentage; ‡Five year-overall survival rate (5Y-OSR) and 5 year-disease free survival rate (5Y-DFSR), proportion of survival derived from Kaplan-Meier analysis; §Hazard ratios (HRs), 95% confidence intervals (CIs) and corresponding P values were calculated using multivariate Cox proportional hazard models, adjusted for age, gender, smoking status, tumor histology, pathologic stage and adjuvant therapy; ∥
P value of test for homogeneity.
Table 4
Disease-Free Survival according to the rs833061, rs2010963 and rs3025039 genotypes by tumor histology
SCC = squamous cell carcinoma, AC = adenocarcinoma.
*Column percentage; †Five year-overall survival rate (5Y-OSR) and 5 year-disease free survival rate (5Y-DFSR), proportion of survival derived from Kaplan-Meier analysis; ‡Hazard ratios (HRs), 95% confidence intervals (CIs) and corresponding P values were calculated using multivariate Cox proportional hazard models, adjusted for age, gender, smoking status, tumor histology, pathologic stage and adjuvant therapy; §
P value of test for homogeneity.
DISCUSSION
In the present study, we evaluated the association between potentially functional VEGF polymorphisms (rs833061T>C, rs2010963G>C, and rs3025039C>T) and survival outcomes of NSCLC patients after surgery in a Korean population. Although none of the three genetic variants were significantly associated with OS and DFS in overall patient population, the rs833061T>C showed differential effect on the prognosis of patients when the subjects were stratified by tumor histology. The SNP was associated with worse OS and DFS in AC, whereas it was associated with better OS and DFS in SCC. Our results suggest that the prognostic role of VEGF rs833061T>C may differ depending on tumor histology.
This is the first study evaluating the relationship between VEGF polymorphisms and prognosis of NSCLC patients according to tumor histology. Several studies have evaluated the relationship between potentially functional VEGF polymorphisms and the outcome of NSCLC patients, but the results were inconsistent (141516). For instance, Heist et al. (14) evaluated the relationship between VEGF SNPs and OS among patients with stage I and II NSCLC treated with surgical resection and reported that the rs833061T>C was not significantly associated with OS. Guan et al. (15) reported rs833061 TC or CC genotypes were associated with better survival among Caucasian patients with locally advanced NSCLC. In contrast, Masago et al. (16) found that the rs833061T>C was associated with worse survival in Japanese NSCLC patients.
The VEGF gene is located on chromosome 6p21.3 and consists of 8 exons and 7 introns (22). Previous studies found that this gene has at least 30 SNPs (23). Among them, rs833061T>C, rs2010963G>C, and rs3025039C>T are putatively functional SNPs which may influence levels of VEGF expression. It has been reported that the rs833061T>C may be associated with increased VEGF promoter activity and plasma levels (2425).
In our study, the rs833061 T>C was associated with better survival outcomes in SCC but worse survival outcomes in AC. The reason for this finding remains unclear, but our results may be explained by a different VEGF expression and angiogenesis depending on tumor histology. Hypoxia is an important feature of tumors and induces hypoxia-inducible factor-1 which regulates various mediators including VEGF, activating angiogenesis (26). In addition, hypoxia induces variant tumor cells which adapt to survive and to proliferate under hypoxic condition by various mechanisms (1516). These variant tumor cells are selected through clonal expansion and aggravate tumor hypoxia by increasing the structurally and functionally disturbed angiogenesis (1516). This vicious cycle contributes to the poor outcome including development of aggressive phenotype with high metastatic rate, resistance to treatment, and higher tumor recurrence rates (171819). In previous studies, the degree of VEGF expression and tumor angiogenesis in response to hypoxia was different according to tumor histology: AC showed more prominent VEGF expression and microvessel formation than SCC (6202728). Taken together, it is possible that VEGF mediated tumor angiogenesis is a more important determinant of the prognosis in AC compared to SCC. This may partially explain the different prognostic effect of VEGF rs833061T>C according to tumor histology. In this study, the rs833061T>C, associated with increased VEGF expression (2425), could predict worse prognosis only in AC. However, the VEGF may not have a critical role in determining the prognosis in SCC. Instead, a possible alternative explanation is that another angiogenic factor might contribute to the angiogenesis and prognosis in SCC. Recent advances in the molecular biology of lung cancer have led to the understanding that NSCLC is a heterogeneous disease: different pathogenesis and clinical features, as well as markedly different genetic alterations between SCC and AC (2930). Further research is warranted on the mechanism of different prognostic role of VEGF rs833061T>C between SCC and AC, which may lead to better understanding of the pathogenesis of lung cancer.
Antiangiogenic drugs such as bevacizumab, a monoclonal antibody to VEGF, are currently available in selected patients with advanced stage AC (31). Several clinical studies have investigated the benefit of bevacizumab as an adjuvant or a neoadjuvant therapy in early stage AC (323334). In early stage NSCLC, adjuvant therapy is considered for patients who have risk factors for poor outcome (e.g. vascular invasion, tumors > 4 cm, visceral pleural involvement) (35). In addition to these factors, the rs833062T>C may help select AC patients with poor prognosis who may benefit from adjuvant antiangiogenic drug therapy.
In conclusion, the rs833061T>C may be a useful prognostic marker for patients with surgically resected NSCLC, which has dissimilar roles in different tumor histology. Consequently, testing for the presence of the rs833061T>C may help identify patients with high risk of poor disease outcome, thereby helping to refine therapeutic decisions. However, because this study is the first trial to investigate the association between VEGF polymorphisms and survival outcome according to NSCLC tumor histology, additional studies are required to confirm the findings in diverse ethnic populations.
 XML Download
XML Download