

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Since effective agents are available for liver transplantation (LT), medication adherence has become an important factor of successful treatment outcomes. The estimated rates of non-adherence to immunosuppressive regimens among solid organ transplant recipients ranges from 15%–55% (123). Non-adherence to the immunosuppressive regimen has been cited as a main cause for preventable late acute rejection and allograft loss, suggesting that interventions to improve adherence may improve patient outcomes (45).
Many studies have shown that less frequent dosing leads to a higher percentage of prescribed doses taken (67). Tacrolimus is one of the most frequently used immunosuppressants, and its twice-a-day formulation has a well documented efficacy and safety profile (89). Recently, a once-daily prolonged-release formulation of tacrolimus was developed. According to several studies, conversion from twice-daily to once-daily tacrolimus was well tolerated, and it was safely and conveniently used in stable patients after LT (1011). Despite the comparable pharmacokinetic properties between the standard dosing and extended-release tacrolimus formulations, some patients had adverse events, including abnormal liver function test (LFT) values after conversion. Consequently, they required reconversion to previous medications or an additional immunosuppressant.
Few studies have reported on the aforementioned topics; therefore, we addressed this issue by describing our experience with tacrolimus. We evaluated patient safety after conversion from twice-daily to once-daily tacrolimus, and we identified the risk factors for adverse events.
MATERIALS AND METHODS
Patients
This retrospective cohort study was approved by the institutional review board of Seoul National University Hospital (Seoul, Korea), and informed consent was not required. We screened 222 patients who underwent primary LT and were converted from twice-daily to once-daily tacrolimus between May 2011 and January 2014 at a single center. Inclusion criteria were patients who underwent LT from either a living or deceased donor at least 1 month before enrollment, and those who were consistently taking tacrolimus twice daily for at least 2 weeks before study entry. Patients were required to have stable renal (serum creatinine level, < 2.0 mg/dL) and liver function (serum aspartate aminotransferase and alanine aminotransferase levels were within normal range). Patients were excluded if they were receiving any drugs known to interfere with the pharmacokinetics of tacrolimus, had any history of rejection before study participation, or had an unstable medical condition. All patients were followed for at least 6 months, and the median follow-up was 18.0 months (range, 6.8–30.0 months).
Immunosuppression regimens
Immunosuppressive therapy after LT was based on the combination of calcineurin inhibitors (cyclosporine or tacrolimus), mycophenolate mofetil (MMF), and a corticosteroid. Two types of twice-daily tacrolimus were used before conversion: the reference tacrolimus product (Prograf®; Astellas Pharma, Tokyo, Japan) and the generic formulation of tacrolimus (Tacrobell®; Chong Kun Dang Pharma, Seoul, Korea). The corticosteroid was tapered to zero by 6 months after LT during the study period. Most patients were converted to once-daily tacrolimus (Advagraf®, Astellas Pharma, Inc., Deerfield, IL, USA) on a 1:1 mg basis for their total daily dose. However, some dose adjustments were permitted depending on the patient’s condition, and other immunosuppressants were used according to standard practice. The dosage ratio was defined as the once-daily tacrolimus dosage divided by the twice-daily tacrolimus dosage. Initially, the serum trough levels of tacrolimus and clinical assessments for safety and rejection were completed 1 week after conversion; thereafter, they were routinely evaluated according to the patient’s individual follow-up period. At baseline and during follow-up, subsequent tacrolimus doses were adjusted on an individual basis according to the serum trough level of tacrolimus.
Primary and secondary objectives
The primary study objective was to determine the safety of those who were converted from twice-daily to once-daily tacrolimus. All adverse events were recorded during the follow-up period, and these included gastrointestinal issues, an itching sensation, nephrotoxicity, headache, uncontrolled diabetes mellitus, poor compliance, and abnormal liver function (an aspartate aminotransferase or alanine aminotransferase level more than two times the upper limit of normal). Patients who had an LFT abnormality were classified according to their clinical course as follows: mild, LFT values only improved after increasing the once-daily tacrolimus dosage; moderate, LFT values improved after reconversion to a previous medication and/or improved after adding another immunosuppressant; and severe, an episode of acute cellular rejection.
Secondary objectives included the analysis of risk factors for adverse events, including abnormal LFT values after conversion. The following parameters were analyzed: age, sex, the type of LT, serum tacrolimus trough levels before and after conversion, immunosuppression regimen at conversion, treatment regimen (combined or tacrolimus only), and conversion time after LT.
Statistical analysis
For intergroup comparisons, the distribution of data was first evaluated for normality using the Shapiro-Wilk test. Normally distributed data are presented as a mean ± standard deviation, and the groups were compared using the Student t-test. Descriptive variables were analyzed using the χ2 or Fisher exact test, as appropriate. Multiple logistic regression analysis was used to determine the risk factors for adverse events after conversion. P values < 0.05 were considered statistically significant. Statistical analysis was conducted using SPSS, version 19.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Two hundred twenty-two patients who underwent LT were converted from twice-daily to once-daily tacrolimus, whereas 4 patients were excluded because they were lost to follow-up. Ultimately, 218 consecutive patients were enrolled. Detailed demographics of the study population are presented in Table 1. Patients’ mean age was 51.97 years (range, 10–78 years), and 71.1% were men (155 men and 63 women). Seventeen patients (7.8%) were aged < 18 years.
Table 1
Demographics of patients

![]()
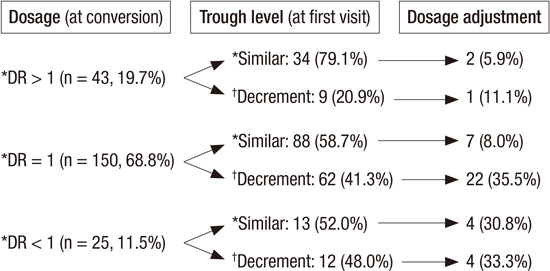
Hepatocellular carcinoma (45.9%) and hepatitis B virus-related liver cirrhosis (30.3%) were the common primary diseases for LT. Patients who underwent a deceased donor LT (66.5%) were more common than patients who underwent a living donor LT (33.5%). Before conversion, the generic formulation of tacrolimus (56.7%) was used slightly more than the reference tacrolimus (43.3%). The immunosuppression regimen of most patients at conversion was mostly based on monotherapy (79.9%: tacrolimus monotherapy [79.4%] and MMF monotherapy [0.5%]) and combined therapy (20.1%: tacrolimus and MMF [14.7%]; tacrolimus and a corticosteroid [4.1%]; and tacrolimus, MMF, and a corticosteroid [1.4%]). The median time from LT to enrollment was 69.0 months (range, 1.2–161.4 months). The mean baseline serum trough level of tacrolimus was 4.31 ± 2.00 ng/mL, followed by a significant decrease to 3.55 ± 2.13 ng/mL in 1 or 2 weeks after conversion (Table 1). Most patients were converted from twice-daily to once-daily tacrolimus with a 1:1 dosage ratio (68.8%). Among these patients, 58.7% and 41.3% had a similar (< 30% of a decrease) or decreased (> 30%) serum trough level of tacrolimus after conversion, respectively, and some required a dose adjustment. Compared to the group with a 1:1 dosage ratio, the group that was converted to a < 1 dosage ratio (11.5%) had a larger proportion of patients with a decreased (48.0%) tacrolimus serum trough level that consequently required a dose adjustment. However, the group with a > 1 dosage ratio (19.7%) also had some proportion of patients with a decreased (20.9%) tacrolimus serum trough level (Fig. 1).
 | Fig. 1Dosage vs. trough level after conversion.
DR = dosage ratio, Similar = < 30% decrease of tacrolimus level after conversion, Decrement = ≥ 30% decrease of tacrolimus trough level after conversion.
|
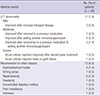
Of 218 patients, 30 (13.8%) had adverse events after conversion. An LFT abnormality was the most common adverse event (n = 17). Those with other adverse events required reconversion to a previous medication (Table 2).
Table 2
Adverse events after conversion
![]()
Patients who had an LFT abnormality were classified according to their clinical course, and most patients were mild or moderate and improved after adjustment. However, 2 patients had severe adverse events; acute cellular rejection in 1 patient improved after steroid pulse treatment, and the other had graft failure (Table 2).
The proportion of an LFT abnormality according to the conversion time after LT and the dosage ratio was analyzed. There were no patients with an LFT abnormality among those with a dosage ratio > 1. However, a proportion of patients who converted to the same dosage ratio or a dosage ratio < 1 had an LFT abnormality, especially within 5 years after LT (Fig. 2). In addition, 2 patients (20.0%) had an LFT abnormality with a conversion time of < 6 months. In patients with the same dosage ratio or a dosage ratio < 1, a conversion time within 5 years was the only significant risk factor for an LFT abnormality after conversion (odds ratio, 11.850; 95% confidence interval, 1.321–106.325, P = 0.027) (Table 3).
 | Fig. 2Proportion of LFT abnormality after conversion by conversion time and dosage ratio.
(A) LFT abnormality after conversion in patients who had DR > 1. There was no patient with LFT abnormality after conversion. (B) LFT abnormality after conversion in patients who had DR = 1. 7 (11.3%) patients in Group B and 4 (4.5%) patients in Group C had LFT abnormality after conversion. (C) LFT abnormality after conversion in patients who had DR < 1. 4 (33.3%) patients in Group B and 2 (15.4%) patients in Group C had LFT abnormality after conversion (P = 0.003).
Group A = LFT normal, Group B = LFT abnormality in patient with ≥ 30% decrease of tacrolimus level after conversion, Group C = LFT abnormality in patient with < 30% decrease tacrolimus level after conversion, LFT = liver function test, DR = dosage ratio.
|
Table 3
Risk factor analysis for LFT abnormality after conversion in patients with DR ≤ 1
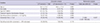
LFT normal and abnormal, less and more than two times of the upper limit of normal aspartate aminotransferase or alanine aminotransferase value.
LFT = liver function test, DR = dosage ratio, LT = liver transplantation, DDLT = deceased-donor liver transplantation.
![]()
DISCUSSION
The life-long intake of immunosuppressive medications in patients who have undergone LT is often complex, and it contributes to a high incidence of non-adherence to medication, which results in an increase in late acute rejection and late graft loss (8910). Drug adherence decreases over time in patients after LT, depending on the type of medication, number of drugs to be taken, and number of daily doses (1213). One study analyzed the risk factors for poor adherence to medication using electronic monitoring, and the average percentage of missed doses was increased more in the evening than in the day in the twice-daily group. In addition, more patients in the once-daily group significantly remained consistent with the treatment compared to the twice-daily group (14). Similar findings were demonstrated in several other studies, which suggest that reducing the dose frequency may be an important way to improve compliance; therefore, once-daily tacrolimus has potential advantages for improving long-term outcomes (101215). In the present study, children and adolescents showed a poorer adherence than older patients did; our study population included 17 young patients (7.8%).
According to previous reports, the safety and efficacy between once-daily and twice-daily tacrolimus were comparable (31617). Conversion from twice-daily to once-daily tacrolimus is associated with an equivalent exposure and a steady state and trough levels; however, there is a different pharmacokinetic profile with a substantially reduced bioavailability (817). The slower access of once-daily tacrolimus to CYP3A4 enzymes metabolism may prevent these enzymes from being overwhelmed by a high drug concentration and decreased daily peaks. Avoidance of high peak levels may lead to a lower incidence of cardiovascular disease, hyperglycemia, and adverse events from calcineurin inhibitor therapy (101819). The positive effect of once-daily tacrolimus on renal function, a significant cause of morbidity and mortality in patients after LT, was also tempered, and one study demonstrated an improvement in the creatinine clearance level after conversion (10). However, in the present study, an LFT abnormality was observed as the most common adverse event, and most patients improved after a dose adjustment or reconversion to a previous medication. Furthermore, 2 patients (0.9%) had an episode of acute rejection, which was diagnosed after graft biopsy.
Corticosteroids and anti-proliferative agents are frequently discontinued during the first or second post-transplant year, and approximately one-third to one-half of patients only receive a single immunosuppressant. The common immunosuppression regimen at conversion in the current study was tacrolimus monotherapy (79.4%). Among patients with tacrolimus monotherapy at conversion, 19 (11.0%) had an adverse event and 10 (5.7%) had an LFT abnormality, which was not very different among the total study population. The risk factors for an LFT abnormality after conversion in patients with a dose ratio ≤ 1 also considered the treatment regimen at conversion, and monotherapy or combination therapy did not cause an LFT abnormality after conversion. The median time of conversion after LT was 69.0 months, and although our patients had combined treatment, their immunosuppression was maintained using the minimum required regimen. Therefore, small changes in the immunosuppressive drug concentration after conversion can lead to an LFT abnormality.
In the current study, patients who were converted within > 5 years after LT had significantly fewer LFT abnormalities. The increased immune tolerance after 5 years may explain this. A previous study reported that 19% of patients achieved drug freedom 5 years after LT. Some patients in our study may have also experienced this phenomenon, but this was uncertain. Immune tolerance following LT may be defined as normal graft function without the features of graft rejection and the need for immunosuppressive drugs.
Many studies have shown that higher doses of once-daily tacrolimus are required to achieve similar tacrolimus exposure (818). Our study also showed similar findings; the mean serum trough level of tacrolimus decreased after conversion in proportion to the dosage ratio. To achieve similar exposure to twice-daily tacrolimus, the initial dose of once-daily tacrolimus needs to be higher. Interestingly, despite the decrease in the serum tacrolimus level by > 30% after conversion, none of the patients with a dosage ratio > 1 had an LFT abnormality. However, some patients who were converted to a similar dose or < 1 dosage ratio had an LFT abnormality even though they maintained a similar serum tacrolimus level after conversion. Contrary to previous reports that have shown comparable areas under the curve and a trough target level between two formulations (711), our study’s finding indicates the possibility that for drug level monitoring, a different recommended target trough level may be needed for both formulations to ensure the same efficacy. The reasons for the aforementioned differences are not yet fully understood, but once-daily tacrolimus has different dissolution properties and is delivered in a more distant area of the gastrointestinal tract compared to twice-daily tacrolimus. Differences in the cytochrome P450 metabolism between Asian and Western populations compared to other previous Western populations may also explain the different findings.
There are several limitations to this study. First, it was a retrospective study; thus, we had to rely on the accuracy of complete medical records for our analysis. Second, changes in the pharmacokinetics after conversion could not be investigated. Lastly, selection bias cannot be eliminated. Thus, further studies with prospectively randomized populations are warranted to confirm these promising findings.
In conclusion, considering the advantage of patients’ adherence to medication, converting from twice-daily to once-daily tacrolimus showed a comparable efficacy and safety; thus, it may be a useful option in stable patients after LT. However, some patients had adverse events after conversion with a similar dose or decrease in the dosage ratio at conversion, and conversion within 5 years after LT resulted in an LFT abnormality. Therefore, an initially higher dose of once-daily tacrolimus at conversion after LT should be considered. These new findings may help physicians achieve patient safety outcomes after conversion from twice-daily to once-daily tacrolimus.
 XML Download
XML Download