

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
In recent years, there has been increasing interest in emotional labour because of the shift of the economy from the manufacturing to the service sector. The service for customer industry has accounted for increasingly large proportions of total industry across the world; it accounted for 70.2% of world GDP in 2012, 59.3% of GDP in the Republic of Korea, 64% in the East Asia and Pacific area, 73% in Europe and Central Asia, 43% in the Middle East and North Africa, and 63% in Latin America and the Caribbean (The World Bank 2013, data available at http://data.worldbank.org/indicator/NV.SRV.TETC.ZS). These industry are frequently required to meet customers face-to-face to achieve their goals, such as selling products or solving customers’ complains. Naturally, this work involves a great deal of so-called ‘emotional labour’. This term was first defined by Hochschild as ‘the management of feeling to create a publicly observable facial and bodily display; emotional labor is sold for a wage and therefore has exchange value’ (1). Workers in jobs requiring emotional labour are often asked to submit to the emotional demands of controlling their inner feelings, or their outward expression, and displaying only appropriate emotion with their customers. Regardless of their inner feelings, service workers are expected to have a friendly relationship with customers by expressing positive emotions and hiding negative ones (2). This emotional dissonance could cause emotional stress and induce psychological damage leading to emotional burnout, exhaustion, and a low level of job satisfaction or performance (3), as well as serious mental health issues such as depression (4). Further, the suppression of emotion has been correlated with mortality from all causes (Hazard Ratio 1.35, 95% Confidence Interval 1.00–1.82) (5). However, very little is known about the effect of emotional demands at the workplace, including suppressed emotions, on health problems.
Sleep disturbance, especially insomnia, represents an enormous impact on the wellbeing of individuals and society as a whole. Many international studies have consistently showed a high prevalence of insomnia in the population of many countries (67). The prevalence of insomnia has a wide range (from 8 to 40%) depending on the criteria used to evaluate it (678). In Korea, the prevalence of insomnia has been estimated at 8.2% in individuals above the age of 20 (9).
Insomnia can cause various psychiatric and physical health problems. Several population-based studies have shown that insomnia is considered a strong risk factor for depression and anxiety (10). Insomnia has also been associated with congestive heart failure, obstructive airway disease (11), hypertension (12), and general mortality (13). Several studies have associated short sleep durations with chronic diseases such as coronary heart disease, stroke, and diabetes mellitus, (14) and cancer (15). The direct costs of insomnia were estimated at approximately 14 billion USD in the United States alone in 1999 (outpatient visits: 11.96 billion USD; medications: 1.97 billion USD) (16). Considering that insomnia is associated with a loss of productivity, absenteeism, and occupational accidents (17), it also results in considerable indirect costs on the economic dynamism of the society. In the US in 1994, the cost of absenteeism was 57 billion USD, with a loss of productivity of 41.1 billion (18) USD.
Possible risk factors found to be influencing insomnia are older age, being female, pre-existing medical or psychiatric disorders, and reduced physical activity (919). However, far too little attention has been paid to the relationship between insomnia and the stress of emotional demands. Previous studies (2021) showed that excessive work demands might also be a risk factor for insomnia. Researchers, however, did not attempt to differentiate emotional from physical demands, because emotional labour was not considered a significantly important factor in insomnia. Thus, although risk factors for insomnia have been extensively researched, no single study exists which appropriately considers the effects of emotional demand on insomnia.
Engaging complaining customers can increase the emotional demands on a service worker. Hence, we assumed that 1) engaging complaining customers and 2) suppressing emotions at a worksite would be crucial factors in potential excessive emotional demand in service workers. Therefore, this study set out to assess the association between sleep disturbance and emotional demands, including the influence of 1) and 2) above in a population-based study from a nationally representative sample of Korean workers, the Korean Working Condition Survey (KWCS) which has comprehensive questionnaires regarding the occupational information for almost fifty thousand workers in Korea.
MATERIALS AND METHODS
Study design and participants
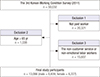
We used data from the 3rd Korean Working Condition Survey (KWCS) (2011) managed by the Korea Occupational Safety and Health Agency. A total of 50,031 working individuals were surveyed and interviewed by multi-area random sampling to ensure that the sample was representative of active Korean workers aged over 15 years. The KWCS is a national open database with safeguards to protect the subjects’ anonymity and privacy rights. Participants gave their consent to be included in the KWCS. For our study, we chose our subset using the following inclusion/exclusion criteria: 1) workers who were not paid were excluded from the total sample size (n = 20,321), and 2) 1,036 participants older than 65 were excluded to describe only the general below-retirement-age population, 3) to select customer service workers, we asked a question about occupational character: ‘Does your job include something like the following?’ with the inclusive answer ‘I directly dealt with individuals who are, for e.g. customers, passengers, students, or patients, not business partners’. The possible answers were always, almost always, 75% of their hours of duty, 50% of their hours of duty, 25% of their hours of duty, almost never, and never. We excluded participants who responded almost never and never as non-service workers. Thereafter, participants were asked about their working conditions using a question to select workers having emotional display rules ‘I worked with emotional involvement in job’. The possible answers were always, almost always, sometimes, almost never, and never. We again removed individuals who answered almost never or never. These 3 exclusion criteria excluded many subjects from the final analysis (n = 15,607). As mentioned before, there is little published research focusing on the outcomes of workplace emotional stress (e.g. sleep disturbance). However, existing research recognizes the critical role played by emotional labour in psychiatric complaints (21). Given this, we sought to investigate the health effects of emotional stress in customer service workers. After the necessary exclusions to limit our sample to those of interest, a total of 13,066 paid customer service workers (6,839 male, 6,227 female) were included in the current study. A schematic diagram of the study population is shown in Fig. 1.
Emotional demand
We used two questions to investigate the extent of the emotional demands of individuals’ workplace. The first question had ‘I manage upset customers or patients’ as an answer. The possible answers were the same as those listed previously. We re-grouped the responses into three categories; always and almost always into ‘Always’, responses of almost never and never into ‘Rarely’, and 25%–75% of their hours of duty into ‘Sometimes’. The second question was the participants’ level of agreement with the phrase ‘I have to suppress my emotions during work’. The possible answers for that question were always, almost always, sometimes, almost never, or never. As before, we regrouped the two positive and negative answers into ‘Always’ and ‘Rarely’ respectively, and left ‘Sometimes’ as the third category. The two forms of emotional demand were dubbed ‘Engaging complaining customers’ and ‘Suppressed emotion at workplace’ respectively.
We then defined nine groups in a 3 by 3 matrix of Rarely, Sometimes, or Always for ‘Engaging complaining customers’ and for ‘Suppressed emotion at workplace’. For example, group one was Rarely ‘Engaging complaining customers’ and Rarely ‘Suppressed emotion at workplace’, and group nine was Always ‘Engaging complaining customers’ and ‘Suppressed emotion at workplace’.
Sleep disturbance
To define sleep disturbance, we used a question regarding insomnia or sleep deprivation. The question was ‘Have you suffered from the following health problem during the past 12 months’, and one answer was ‘insomnia or sleep disturbance’. The response options were ‘ever’ and ‘never’. We defined respondents who answered ‘ever’ as having sleep disturbances and the others as not.
Other potentially confounding variables
Socio-economic status, including household income and education, is a basic and important confounding variable when investigating risk factors for sleep disturbance. The KWCS includes questions about household income per month and educational level. Monthly household income levels were < 1,000 USD, < 2,000 USD, < 3,000 USD, and ≥ 3,000 USD. We re-grouped individuals by their educational level: middle school or lower, high school, and college or higher.
Working conditions are well-known factors for workers’ health outcomes. Job satisfaction was estimated by the question ‘Generally, what do you think about your current job?’ The possible answers were not at all satisfied, not very satisfied, satisfied, and very satisfied. We re-grouped the four options into two categories: ‘satisfied’ and ‘unsatisfied’. Weekly working hours, without counting any breaks, were categorized as under 40, 40–49, and more than 50 hours per week. We used the questionnaire about job schedule to find shift-scheduled workers, because of a higher risk for sleep disturbance among shift workers. Job schedules are grouped into two categories in the KWCS; fixed and shift. In Korea, there is a kind of class or status or position of job which are permanent or temporary. The permanent working status is defined as a contract of employment for regular retirement, or pension for retirement. The temporary working status is defined as daily employed or temporary employed workers. Occupational classification are regrouped to three groups from 10 major groups of International Standard Classifications of occupations by skills and duties level; office workers (managers, professionals, and technicians and associate professionals), sales and service workers (clerical support workers and service and sales workers), manual workers (skilled agricultural, forestry and fishery workers, craft and related trades workers, plant and machine operators, and assemblers, and elementary occupations).
Statistical analysis
We used χ2 tests to compare the different socioeconomic characteristics and occupational status of those with and without sleep disturbance (Table 1). The odds ratio (OR) and 95% confidence intervals (95% CIs) for having a sleep disturbance were calculated using a fully adjusted multiple logistic regression model. The P values for interactions between ‘Engaging complaining customers’ and ‘Suppressed emotion at worksite’ were calculated in a logistic regression model. A P value below 0.05 was considered statistically significant.
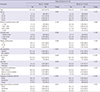
Table 1
Basic characteristics of study participants according to sleep disturbance and gender
Ethics statement
All KWCS participants provided written informed consent for voluntary participation of them. All identifiable information of participants was deleted before data analyses. This current analysis was approved by the institutional review board (IRB) of Yonsei University Graduate School of Public Health (IRB No. 2-1040939-AB-N-01-2015-309).
RESULTS
Table 1 presents the basic demographic characteristics of the study participants based on their sleep disturbance status and sex. There were 13,066 respondents in our research, consisting of 6,839 (52.3%) males and 6,227 (42.8%) females. The prevalence of sleep disturbance was 2.4% (n = 161) for male workers and 2.0% (n = 126) for female workers.
The association between sleep disturbance and the level of emotional demand is shown in Table 2. These ORs were adjusted for age, household income level, education level, current job satisfaction, and working hours per week. Those consistently exposed to working environments where they engaged complaining customers were at a significantly higher risk for sleep disturbance. Where ‘Rarely’ implied an OR of 1.00, men and women were both affected by their environments (Sometimes: OR, 1.45; 95% CI, 0.98–2.04; OR, 1.48; 95% CI 0.98–2.23, respectively; Always: OR, 5.46; 95% CI, 3.43–8.68; OR, 5.59; 95% CI, 3.30–9.46, respectively). The high levels of sleep disturbance in participants in the Always category were particularly striking. Participants suppressing their emotions at work were also more likely to have sleep disturbances. With rarely again as a reference OR of 1.00, men Always required to suppress their emotions had an OR of 1.78, and a 95% CI of 1.16–2.73, women in the same category had an OR of 1.63, and a 95% CI of 1.02–2.63. No significant differences were found between employees rarely suppressing their emotions and those sometimes suppressing them, in either sex.
Table 2
Results of odds ratio and 95% confidence intervals for sleep disturbance by multiple logistic regression model

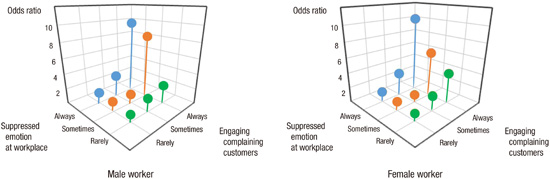
Fig. 2 summarizes the interaction effects between 1) engaging complaining customers and 2) suppressing emotions, and their effect on sleep disturbance. There were remarkable synergistic effects on sleep disturbance between the two factors. The results are presented with factor 1) first, followed by 2). OR references (rare-rare) were always 1.00. For men, the always-always OR was 9.66, with a 95% CI of 4.34–20.80; the always-sometimes interaction was an OR of 8.18, and a 95% CI of 3.97–16.24; and the sometimes-always OR was 2.86, with a 95% CI of 1.54–5.31. For women, these interactions were 10.17, 95% CI 4.46–22.07; OR 5.99, 95% CI 2.14–15.89; OR 3.09, 95% CI 1.47–6.10. Additionally, women had an always-rarely OR of 4.06, 95% CI 1.11–14.78.
Fig. 2
Interaction effect of suppressed emotion at workplace and facing complaining customers for sleep disturbance.

The very large OR values for always-always interactions in both men and women were statistically significant (P values for the interaction = 0.05 for both sexes).
DISCUSSION
This research extends our knowledge of the effects of excessive emotional demands on human health. This is the first study to undertake such a large cross-sectional study to reveal the association between sleep disturbance and emotional demands, construed as having to engage with complaining customers and suppressing one’s emotions during work.
The prevalence of sleep disturbance in our study (male: 2.4%; female 2.0%) was lower than reported in a previous study in Korea (8.2%) (9). Older age is a major risk factor for insomnia (919). As we were concerned with people of working age, we excluded respondents who were older than 65 in our study; this is a possible explanation for the decreased prevalence of insomnia we observed.
There was an increasing trend of association between sleep disturbances and engaging with complaining customers. The more frequently workers engaged with complaining customers, the more they had sleep disturbance. The level of suppressed emotion at work was also increasingly correlated with sleep disturbance in men. In women, workers who always suppressed their emotions had a significantly higher risk for sleep disturbance than who rarely suppressed their emotions. Moreover, engaging with complaining customers and suppressing emotions had synergistic effects on sleep disturbance in both male and female workers. The results of this study reveal that excessive emotional demands could be a risk factor for sleep disturbance.
There are many possible explanations for our results. The relationship between sleep disturbances, especially insomnia and stress from excessive emotional demands, could be explained physiologically. Hyperarousal is the most widely accepted explanation for insomnia. Hyperarousal is defined as a highly vigilant state during the day that could potentially interrupt the initiation and maintenance of sleep at night (22). There is a correlation between insomnia and the physiological activities of the stress system. The stress system itself is comprised of two primary systems: the neuroendocrine (hypothalamic-pituitary-adrenal [HPA]) system and the sympathetic nervous system. In the neuroendocrine system, overactivation of the HPA axis is the main mechanism explaining insomnia. Increased corticotropin releasing factor activity was proposed as a pathogenic cause of insomnia (23). Urinary free cortisol levels are positively associated with total wake time and night-time wakefulness (23). With respect to the sympathetic nervous system, several studies have showed increased activity of the sympathetic nervous system of individuals with insomnia. The signs of activation of the sympathetic nervous system include increased body temperature (24) and basal metabolic rate (25), both of which have been demonstrated in individuals with insomnia. In addition, it was reported that circulating norepinephrine level was high in individuals with insomnia (23). Consequently, continuous exposure to stress from excessive emotional demands might activate the stress system excessively, including the HPA axis and sympathetic nervous system, and thereby causing sleep disturbances, especially insomnia.
Furthermore, the stress from excessive emotional demands could cause psychiatric (depression or anxiety) and behavioural problems (alcohol use disorders or physical inactivity). Forty percent of those who suffered from insomnia had comorbid psychiatric disorders, most frequently depression (26). Depression could be both a risk factor and consequence of insomnia (27). The mean prevalence of insomnia in alcohol-dependent patients in nine studies was estimated at approximately 56% (range: 36%–91%) (28). In addition, as mentioned earlier, reduced physical activity is considered a risk factor for insomnia (29).
Finally, service workers usually deal with agitated customers or ill patients. By the nature of emotional labour, employees are frequently exposed to traumatic events such as violence or abusive language. It is a widely held view that post-traumatic stress disorder can also cause sleep disturbance, especially in the rapid eye movement sleep state (REM sleep) (30).
The primary strength of our study is that it is based on a well-established population-based survey. For this reason, our study has high statistical power. Additionally, we studied an ethnically homogenous group of Korean workers, which could remove the effect of racial differences on sleep disturbance.
Despite its strengths, this research has a number of limitations that need to be considered. First, our study was a cross-sectional study where causal relationships between sleep disturbance and excessive emotional demands could not be fully explained. A further longitudinal study will be necessary to assess the cause-and-effect relationship between excessive emotional demands and sleep disturbances. Second, the concept of emotional labour has not yet been precisely defined. From the first appearance of the term ‘emotional labor’, by Hochschild (1), there has been increasing interest in emotional labour due to the change of economic systems to more fully depend on service industries. Considering the importance of emotional labour in light of the increasing numbers of service workers, an exact definition of the term is necessary to conduct further studies. A previous study has claimed that emotional demands are, broadly, projecting positive emotions, and hiding negative ones (2). We, however, investigated only the latter factor of emotional demand. Assessing only one factor, however, might not sufficiently represent emotional demands as a whole. Further study is needed which will address both factors simultaneously. Third, adjustment for variables related to sleep disturbance was not performed. Possible confounding factors for insomnia such as pre-existing medical or psychiatric disorders and working night or rotating shifts were not evaluated in our study. Fourth, sleep disturbance was judged by self-assessment, not clinically diagnosed using clinical criteria or medical devices (e.g. polysomnography or actigraphy). For that reason, the correlation between excessive emotional demands and sleep disturbance could be underestimated. However, self-reported sleep problems remain important to consider, because one of the determining factors for a clinical diagnosis of insomnia is a self-reported sleep disturbance. Indeed, the feeling of discomfort from sleep disturbance is a main target of the management or treatment of insomnia.
This study found that engaging with complaining customers and suppressing emotion at work were significantly associated with sleep disturbance among Korean paid workers (< 65 years old). In addition, there were synergistic effects between each of these factors, which suggested that increased attention ought to be paid to emotional stresses in service workers in order to ensure their good health.
 XML Download
XML Download