

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Reform of the care delivery system is a significant component of the health policy agenda. The Korean health care system achieved several noteworthy results during the past four decades. For example, the National Health Insurance has been appraised highly for establishing universal health coverage in a short period of twelve years (1). The care delivery system, in contrast, has struggled and so far failed to meet people’s health care needs. There is no well-demarcated line between primary care and hospital care, so clinics and hospitals are now in competition for patients in their communities (2,3). This makes it difficult for diverse medical care providers to collaborate with each other in meeting people’s health care needs. As a result, patients’ care journeys are often fragmented and distorted, which leads to their discontent over care quality. Thus, care delivery system reform has been emphasized (4,5).
In this context, we believe that the ecology of medical care model proposed by White et al. (6), who was inspired by the Horders’ work (7), can contribute to productive discussions on health care reform in Korea. The medical care ecology model focuses on the pattern of people’s medical care utilization rather than that of their diseases (6). To put it another way, the model describes the association of people’s health-related behaviors and the medical care resources in a community, which leads to the view that the perspective of health service research should change from a clinically oriented and provider-centered one to a population-based and user-centered one. Since the seminal work by White et al. (6), and its revival by Green et al. (8), health service researchers have conducted similar studies (9-27) in countries including Japan (13,19,21) and China (23). However, little is known about the medical care ecology in Korea.
This study aimed to estimate the number of people aged 18 and over per 1,000 residents who had a health problem and/or medical care at a variety of care settings during an average month of 2012 in Korea.
MATERIALS AND METHODS
Data and study subjects
Data were derived from the Korea Health Panel (KHP) version 1.1 (2008–2012). Prepared under the auspices of the National Health Insurance Service and the Korea Institute for Health and Social Affairs, the KHP is a longitudinal data study providing sources for the analysis of medical utilization and expenditure in Korea. Survey data, health diaries, medical fee receipts, and health insurance claims data were collected to build an integrated dataset (28). The dataset for the year 2012 is the latest yearly dataset of the publicly released KHP; it includes data for characteristics of the panel members surveyed in 2012 and for medical utilization and expenditure during the same year.
A study population of 11,518 people aged 18 and over was drawn from the 15,872 total panel members who comprised the 2012 dataset. The panel members also responded to additional, individual survey questions included in the KHP, and the survey results provide detailed information on their health states, lifestyles, medical utilization and expenditure. The questionnaire changed slightly from year to year. We limited the study population to those who had responded to the individual survey because they were the only information source that enabled us to determine the health problem experience.
Variables
We defined having any health problem in an average month as having any mental health problem or being bed-ridden or being absent from work/school due to health problems during the past month or having any chronic disease. Having any mental health problem was defined as having any of the following five problems: physical and mental stress, frustration, unmet basic needs, job stress and anxiety about the future. Having chronic disease was defined as having any sorts of chronic disease diagnosed by a physician. The number of people who experienced any health problem in an average month was multiplied by the population weights, summed up, divided by the sum of the population weights (that is, the estimated population in 2012), and then multiplied by 1,000 to get the number of those who experienced any health problem per 1,000 people in an average month.
The number of those who used medical care per 1,000 people in an average month was calculated as follows. First, for each study participant we calculated the number of months in which he or she used each kind of medical care at least once. Ambulatory care was divided into four categories: ambulatory care at clinics, hospital outpatient departments (OPDs), and tertiary hospital OPDs, as well as Korean Oriental medical ambulatory care. The category of clinic included physician’s offices, public health centers and public health sub-centers. Korean Oriental medical ambulatory care included care at clinics, hospital OPDs and tertiary hospital OPDs when they provided Korean Oriental medical care. Inpatient care was classified into three groups only—in clinics, hospitals and tertiary hospitals—because the volume of inpatient Korean Oriental medical care was negligible. Emergency care was not divided into sub-groups. The number of months for each study participant was divided by 12, multiplied by the population weights, summed up, also divided by the sum of the population weights (that is, the estimated population in 2012), and then multiplied by 1,000 to finally get the number of those who used each kind of medical care per 1,000 people in an average month (8).
RESULTS
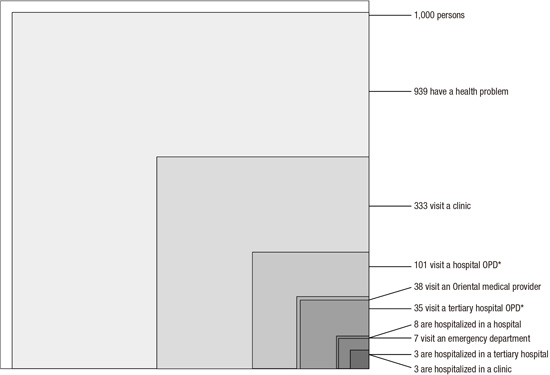
A total of 11,518 persons aged 18 and over were included in the study; 38.8% of them were aged 18–44 years, 35.8% of them 45–64 years, and 25.5% of them over 65 years. 53.5% of them were women. As depicted in Fig. 1, 939 (95% confidence interval [CI], 934–944) persons per 1,000 residents aged 18 and over experienced a health problem in an average month of 2012. The number of those who used ambulatory care at least once at a clinic in an average month was estimated to be 333 (95% CI, 327–339) per 1,000 residents. The estimated numbers of those who visited a hospital OPD, a tertiary hospital OPD and an Oriental medical care provider were 101 (95% CI, 97–104), 35 (95% CI, 33–37) and 38 (95% CI, 36–40) persons per 1,000 residents, respectively. While 7 (95% CI, 7–8) persons visited an emergency department in an average month, the numbers of those who were hospitalized in a clinic, a hospital and a tertiary hospital were estimated to be 3 (95% CI, 2–3), 8 (95% CI, 7–8) and 3 (95% CI, 2–3) persons per 1,000 people, respectively.
 | Fig. 1Estimated number of people per 1,000 residents aged 18 and over who had any health problem and/or medical care in the different care settings in an average month of 2012.
Each square does not necessarily represent a part of the larger square except for the largest one.
OPD = outpatient department.
|
DISCUSSION
This is the first study to describe the ecology of medical care in Korea. The ecology model (6) highlights the unique characteristics of health systems by showing the pattern of symptom experience and medical care utilization from the population-based and user-centered perspective. It also enables the study results to be compared with previous ones, and provides an opportunity to examine the common characteristics of diverse health systems.
There was a gap between the number of people experiencing any health problem and that of people receiving any medical care. The proportion of those who had any health problem in an average month of 2012 was 93.9% of people aged 18 and over, but only 33.3% of them received ambulatory care at a clinic. As noted in Table 1, this finding was consistent with the results of previous studies (8,13,20,26), though three studies (14,22,23) reported different patterns. According to a study conducted in Hong Kong (14), 15.9% of people having any kind of symptoms did self-management. In Korea, however, little was known about how they dealt with their health problems from the population-based perspective.
Table 1
Comparison of medical care ecology studies’ results
| Source (reference) | Country | Data year | Participants' age, yr | Estimated number of people per 1,000 residents | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Health problems | Ambulatory care | Emergency department | Inpatient care | ||||||||
| Clinic | Hospital | Tertiary hospital | CAM* provider | Hospital | Tertiary hospital | ||||||
| This study | Korea | 2012 | ≥ 18 | 939 | 333 | 101 | 35 | 38 | 7 | 8 | 3 |
| Shao et al. (23) | China | 2012 | ≥ 15 | 295 | 173 | 127 | - | 78 | - | 15 | - |
| Vo et al. (26) | Belgium | 2009 | All ages | 851 | 492 | 117 | - | - | - | 15 | - |
| Roncoletta et al. (22) | Brazil | 2008–2009 | ≥ 18 | 398 | 292 | - | - | 22 | 104 | 63 | 1 |
| Hansen et al. (20) | Norway | 2007–2008 | ≥ 30 | 901 | 214 | 91 | - | 55 | - | 14 | - |
| Shao et al. (18) | Taiwan | 2005 | All ages | - | 329 | 152 | 45 | 67 | 19 | 10 | 3 |
| Ferro and Kristiansson (17) | Sweden | 2006 | All ages | - | - | 44 | - | - | 20 | 12 | < 1 |
| Fukui et al. (13) | Japan | 2003 | All ages | 862 | 307 | 88 | 6 | 49 | 10 | 7 | < 1 |
| Leung et al. (14) | Hong Kong | 2002 | All ages | 567 | 440 | 68 | - | 54 | 16 | 7 | 1 |
| Green et al. (8) | US | 1996 | All ages | 800 | 217 | 21 | - | 65 | 13 | 8 | < 1 |
*CAM refers to complementary and/or alternative medicine, but it means Korean Oriental medicine in this study.
![]()
A large share of primary care in the health care system was observed in this study as well as in previous ones (8,13,14,18,20,22,26), as seen in Table 1. However, adequate attention has not been paid to primary care in Korea. Although the government has recently taken primary care initiatives, including the Community Based Primary Care project (29), primary care is still in a vulnerable state (2). As of the end of 2015, 34.3% of clinics were offices of primary care physicians (general physicians, family physicians, general internists and general pediatricians). Primary care physicians also comprised 41.3% of all physicians working at their offices (30). There is no integrated, systematic community training program for primary care physicians, and a lack of primary care curricula and clerkships in medical education (31). Additionally, there is no quality assurance program in primary care with the exception that the Health Insurance Review and Assessment Service periodically evaluates the quality of hypertension and diabetes treatment. The evidence basis for policy formulation is weak because of a lack of primary care research (32). Given this situation, it is necessary to make a turn toward strengthening primary care in policy areas of medical education, physician training, quality improvement, and research promotion.
A unique finding of this study was that tertiary hospitals had a larger share in Korea than in the other countries (8,13,14,17,22) listed in Table 1 except Taiwan (18). Only two studies, one for Taiwan (18) and the other for Japan (13), estimated the number of people using ambulatory care at academic medical centers. In addition, the Japanese study (13) reported that 6 per 1,000 people—much lower than in Korea and Taiwan—received ambulatory care at academic medical centers during the past month. The numbers of people hospitalized in tertiary hospitals were higher in Korea and Taiwan (18) than in the other countries listed in Table 1. Lee et al. (3) reported that the proportions of patients utilizing ambulatory care at hospitals, including tertiary hospitals, among those with an uncomplicated, single disease, were 18.7% for high blood pressure, 18.6% for diabetes and 31.6% for hyperlipidemia. They could successfully manage their chronic diseases at clinics. However, competition in the medical care market and functional failure of the care delivery system have led to a large share of tertiary hospitals in ambulatory care.
The first key strength of this study lay in the framework of medical care ecology, which made it possible to describe a pattern of health problem experience and medical care utilization with a population-based and user-centered perspective. Second, this study suggested that further studies were needed in health service research. For example, the gap between the number of people having any health problem and that of those who had medical care requires researchers to pay attention to understanding the dynamics of people’s symptom experiences and coping behaviors (33). It also puts a stress on self-management and the role of medical care, especially that of primary care, in helping people to self-care (34). Third, the KHP data used in the study had more strengths than other data sources used in previous research. It is a nationally representative dataset. Unlike datasets used in previous studies (9,13,20-23,26), it was less affected by seasonal variation in medical utilization because its survey had been conducted all year round. In addition, while some previous studies used health insurance claim data (16,18,24) or registry data (17), the KHP includes data on health states, such as mental health problems and absenteeism, derived from an additional, individual survey, which enabled us to define people’s health problem experiences. It was also validated by health diaries, medical fee receipts, and health insurance claim data (28).
This study has some limitations, mainly derived from the KHP data. Unlike some preceding research (8,13,14,17,18,26), we could not estimate the number of people aged less than 18 who experienced any health problem because an additional, individual survey was not conducted for this age group (28). There can be a dispute over the definition of health problem. In some previous studies (8,13,14,20,22,23,26), researchers asked people to respond to whether they had any symptom or health problem during the past month, but the KHP survey had no similar question. Therefore, we defined health problem experience by combining the variables of mental health problems, being bed-ridden and absenteeism during the past month and chronic disease. This practice, combined with the diversity of health care systems, made it hard to compare this study’s results with previous ones directly and to evaluate the biases of estimations in this study. The final weakness of the KHP was that it did not include non-traditional care settings. For example, some preceding studies (8,10,13,17,21,22) estimated the number of people having home health care, but the KHP did not yet cover such data. It will be desirable for the KHP to cover data on newly emerging care settings.
As far as we know, this is the first study applying the ecological perspective to medical care in Korea. The study showed that about 30% of people received medical care in an average month of 2012 while more than 90% experienced any health problem in an average month. It also showed that primary care had a large share in the health care system, which implied that primary care should be strengthened and supported now more than ever. What was interesting in this study was that many more people in Korea received ambulatory care at tertiary hospital OPDs as compared with people in other countries. This finding might reflect the functional failure of the care delivery system. We hope that this medical care ecology study contributes to seeing essential characteristics of health care systems and suggesting a new direction for health services research.
 XML Download
XML Download