

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Modern society is interested in quality of life (QOL); that is, people have now turned their attention from mere survival to their physical, psychological, and social well-being (1). Factors associated with QOL include sex, education, age, and income (2). Psychological factors also impact one's QOL in addition to socioeconomic factors (3). Health affects an individual's physical, psychological, and social performance, which all influence an individual's QOL. Therefore, health is the most important factor that needs to be considered to improve one's QOL (4).
Health can be categorized into subjective and objective health (5). Objective health can be expressed in measurable indexes (e.g., chronic diseases, physiological symptoms, physical pain, bone fracture, structural anomaly, etc.) (6). Subjective health is one's perceived level of physical, physiological, psychological, and social health (7), and it is influenced by objective health (8). Subjective health has a significant impact on an individual's behavior and psychology (9). One study reported that poor subjective health influences suicidal behavior in individuals (10). Subjective health also has a direct impact on QOL (1112). Many factors influence subjective health, which include physical factors such as sex, age, and objective health (91314) as well as socioeconomic factors such as educational attainment and economic status (1516).
Socioeconomic status (SES) directly affects an individual's health and can cause health inequalities (17). It affects health behaviors such as tobacco use, alcohol use, and exercise (18192021) as well as one's access to medical care (22232425). Additionally, SES significantly impacts an individual's psychology, and its impact on health, in particular, is well-known (2627). According to the latest research, perceived SES is strongly associated with health (28).
However, the link between industrial accident patients' perceived SES and health recovery has not been well established. Therefore, we conducted a study to investigate the impact that perceived SES has on industrial accident victims' health recovery.
MATERIALS AND METHODS
Study design
Our cross-sectional study used data collected from the first Panel Study of Worker's Compensation Insurance (PSWCI). The initial PSWCI survey was drafted by the Korea Labor Institute from September to December 2012. The final draft was created after incorporating expert opinions and input from the Korea Worker's Compensation and Welfare Service. For the PSWCI, surveyors visited the panel members for one-on-one, in-person interviews. As a rule, the panel members answered the questions themselves using computer-assisted personal interviewing.
Participant sampling
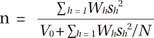
We screened 89,921 industrial accident patients who had completed their official recovery between January 2012 and December 2012. A total of 79 patients whose addresses were unknown were excluded. Also excluded were 7,350 immigrants and Jeju island residents, and 5 patients with disability ratings of 1-3 who were not using rehabilitation services. The remained 82,493 participants were included in the study. Using nine administrative zones, six disability ratings, and the rehabilitation services utilization status as stratification variables, we selected a sample of 2,000 participants for the study. A post-stratification estimator was calculated using the multiplicative inverse of the sampling ratio on the basis of the nine administrative zones, disability ratings, and the rehabilitation services utilization status. The sample size was calculated using the following equation and an allowable target error for a confidence level was considered. V0 is the size of distribution calculated from the target error, and Wh and Sh2 are the ratio and distribution of the h layer. The sample size of a layer was allocated by its size and it was calculated as 2,000, considering the limited research budget and statistical utilization.
The sample was extracted using the Bellwether sampling method rather than using a quota sampling method, and it was based on sex, age, and the duration of recuperation. Therefore, a weighted value was calculated post hoc to compensate.
Measurement of perceived SES
The perceived SES was measured using the question that appeared in the "Health, Daily Life and Quality of Life" section of the first PSWIC: "How do you rate your current QOL considering your income, occupation, educational attainment, and assets?" The following multiple choice answers were provided: 1, high; 2, mid to high; 3, mid to low; and 4, low. Participants who selected high were categorized into the perceived upper SES; those who selected mid to high, into the upper middle SES; those who selected mid to low, into the lower middle SES; and those who selected low, into the lower SES.
Measurement of health recovery
Participants' health recovery status was evaluated using the three questions that appeared in the "Health Status" section of the PSWIC. The first question was "How do you rate your current health compared with your health before the accident?", and it was accompanied by the following multiple choice answers: "1, much better", "2, a bit better", "3, about the same", "4, a bit worse", and "5, much worse". The second question, "How do you rate your health recovery from the accident?" was accompanied with the following multiple choice answers "1, fully recovered", "2, more time needed for a full recovery", and "3, have not recovered at all". The third question, "How often do you feel accident related pain?" was accompanied with the following multiple choice answers, "1, never", "2, once in a while", "3, several times a day", "4, almost everyday", and "5, constantly". Patients who answered the first question with "1, much better", "2, a bit better", and "3, about the same', those who answered the second question with "1, fully recovered", and those who answered the third question with "1, never, 2, once in a while" were considered to have achieved health recovery, whereas the rest did not.
Covariant factors
Participants were divided into several groups according to sociodemographic characteristics, which were described follows: sex (two groups), male and female; age (five groups), 29 years and younger, 30-39, 40-49, 50-59, and 60 years and older; educational attainment (two groups), less than high school (no education, elementary school, middle school, and high school), college and more (community college, college, graduate school, and post-graduate school); tobacco use (three groups), yes, quitted, and no; alcohol use (three groups), yes, quitted, and no; subjective health before the accident (two groups), fairly healthy (if answered, "1, very healthy" or "2, fairly healthy" to the question, "How do you rate your general health before the accident or disease?"), and the rest (if answered, "3, average" or "4, fairly unhealthy"); employment duration (three groups): less than 1 year, 1-10 years, and over 10 years; recuperation period (three groups), less than 6 months, 6 months-1 year, and over 1 year; accident type (two groups), accident, and disease; disability status (two groups), disabled, and not disabled; and economic participation (two groups), employed, and unemployed.
Statistical analysis
We performed a χ2 test for the general characteristics based on perceived SES. We also performed a χ2 test for the general characteristics based on participants' health recovery status. We performed multivariate regression analysis to obtain the odds ratio (OR) for the health recovery of patients with a perceived lower SES and patients with a perceived lower middle SES, with a 95% confidence interval (CI). We also performed a multivariate regression analysis to obtain the OR for the health recovery of patients with a perceived lower SES and patients with a perceived upper middle SES, with a 95% CI. SAS 9.2 was used to perform the statistical analyses, and all statistical significance was set at P<0.05.
RESULTS
General characteristics of participants based on perceived SES
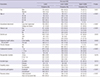
Classification of participants based on perceived SES indicated that 0 patients belonged in the upper class, 96 belonged in the upper middle class, 1,013 belonged in the lower middle class, and 891 belonged in the lower class (Table 1). The upper middle class consisted of 79 men and 17 women, the lower middle class consisted of 854 men and 159 women, and lower class consisted of 753 men and 138 women. In terms of age-related characteristics, participants in their 50s accounted for most of the upper middle class, lower middle class, and lower class, (29 participants, 354, and 322, respectively). Regarding educational characteristics, 49.0% of the upper middle class participants, 20.9% of the lower middle class, and 10.9% of the lower class had college degrees. These three groups had statistically significant differences (P<0.001). Regarding tobacco use, 35.4% of the upper middle class participants, 46.4% of the lower middle class, and 52.9% of the lower class were smokers, which was statistically significant (P<0.001). Regarding pre-accident subjective health, 89.6% of the upper middle class participants, 84.1% of the lower middle class, and 78.9% of the lower class responded as being fairly healthy, which was statistically significant (P=0.002). As for chronic diseases, 7.3% of the upper middle class participants, 14.9% of the lower middle class, and 19.5% of the lower class reported having a chronic disease; this was statistically significant (P=0.001). In terms of employment duration, 38.5% of the upper middle class participants, 59.2% of the lower middle class, and 75.8% of the lower class worked for <1 year, which was statistically significant (P<0.001). With regard to disability status, 72.9% of the upper middle class participants, 82.4% of the lower middle class, and 83.6% of the lower class reported disabilities, which was statistically significant (P=0.032). In terms of economic participation, 86.5% of the upper middle class participants, 77.6% of the lower middle class, and 60.9% of the lower class were currently employed, and this was statistically significant (P<0.001). As for health recovery, 33.3% of the upper middle class participants, 17.8% of the lower middle class, and 9.8% of the lower class reported being fully recovered, which was statistically significant (P<0.001).
Participants' general characteristics based on their health recovery
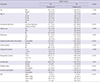
Of all participants, 299 belonged to the health recovery group, and 1,701 belonged to the not recovered group—250 men reported a full recovery, whereas 1,436 men did not (Table 2). Meanwhile, 49 women reported a full recovery, whereas 265 women did not. In terms of age, 22.0% of the participants in their 20s, 22.1% in their 30s, 18.0% in their 40s, 11.9% in their 50s, and 8.3% in their 60s reported a full recovery; this was statistically significant (P<0.001). Regarding educational attainment, 23.0% of participants who had a college education or more and 13.2% with a high school education or less reported a full recovery, which was statistically significant (P<0.001). A full recovery was reported in 16.7% of the participants with a fair pre-accident subjective health and in 7.0% with a poor pre-accident subjective health, and this was statistically significant (P<0.001). Of participants with and without chronic diseases, 9.9% and 15.9%, respectively, reported a fully recovery, and this was statistically significant (P=0.007). Regarding employment duration, a full recovery was reported in 13.3% of participants with an employment duration of <1 year, in 17.1% with an employment duration between 1-10 years, and in 21.9% with an employment duration of >10 years; this was statistically significant (P=0.005). In terms of the recovery period, 21.1% of participants had a recovery period <6 months, 7.6% had between 6-12 months, and 3.9% had >1 year, which was statistically significant (P<0.001). Of the participants, 15.8% who had an accident and 6.0% who had a disease reported a full recovery; this was statistically significant (P=0.001). Of those with and without disabilities, 10.7% and 34.9%, respectively, reported a full recovery, and this was statistically significant (P<0.001). Lastly, 18.6% of participants who were employed and 6.1% who were unemployed reported a full recovery, and this was statistically significant (P<0.001).
Health recovery status based on the participants' perceived SES
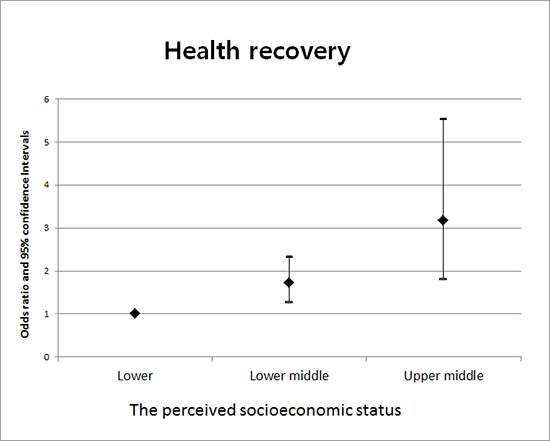
Model 1 in Table 3 shows the ORs (95% CIs) for participants' health recovery according to their perceived SES. The odds of participants with a perceived lower middle SES to full recovery was 1.997 (CI, 1.519-2.625) times greater than that of those with a perceived lower SES. The odds of participants with a perceived upper middle SES was 4.621 (CI, 2.864-7.457) times greater than that of those with a perceived lower SES. Model 2 in Table 3 displays the ORs (95% CIs) for participants' health recovery based on their perceived SES while controlling for sex, age, educational attainment, tobacco use, alcohol use, subjective health prior to the accident, disability status, and economic participation. The odds of participants with a perceived lower middle SES to full recovery was 1.707 (CI, 1.264-2.305) times greater than that of those with a perceived lower SES. The odds of participants with a perceived upper middle SES to full recovery was 3.124 (CI, 1.795-5.438) times greater than that of those with a perceived lower SES.
DISCUSSION
Participants were divided into four socioeconomic classes: upper, upper middle, lower middle, and lower classes. None of the participants reported belonging to the upper class, whereas 96 reported belonging to the upper middle class, which accounted for a mere 5% of the total participants. Therefore, industrial accident victims are socioeconomically disadvantaged in general. Occupations with an elevated risk of industrial accidents generally offer lower wages and provide hazardous working environments. In addition, interrupted participation in the economic activities resulting from an industrial accident generally worsened an individual's socioeconomically disadvantaged status. The proportion of participants with a college education or more increased as participants' perceived SES increased, which was attributed to the fact that one's educational attainment affects one's perceived SES (29). Health risk behaviors such as tobacco and alcohol use have an inverse relationship with the perceived SES. The perceived SES reflects the SES; thus, the lower the SES, the more health risk behaviors people are engaged in (182030). Participants' subjective health prior to the accident also increased as the perceived SES increased, which was congruent with many previous findings (1627). Chronic diseases became more prevalent as the perceived SES decreased. This was thought to be due to the fact that a lower SES discourages people from engaging in more positive health behaviors and makes it challenging for them to take good care of their health (22). The lower the perceived SES, the more prevalent the occupational accidents were in comparison to the occupational diseases. We considered this to be due to the prevalence of people with a lower SES in occupations with a higher risk of occupational accidents.
Our findings also indicated that younger patients tended to achieve full recovery, which proves that age has a significant effect on health recovery. Higher levels of educational attainment also contributed to health recovery. This can be explained by the prevalence of less educated people in workplaces that have a higher risk of occupational accidents, which would affect the individuals' objective health in case of an actual accident/disease (29). Participants with a fair pre-accident subjective health also showed a greater rate of recovery, which may be because health recovery and the pre-accident subjective health are based on participants' subjective opinions. Thus, it is likely that a person with a positive pre-accident subjective health will report a full recovery after the accident. More participants without any chronic diseases reported a full recovery as well, which may be because one's poor objective health is likely to negatively affect one's subjective health. Participants who had an accident, as opposed to a disease, showed a greater rate of recovery. This may be due to the fact that participants' disabilities due to of accidents were temporary, whereas diseases had a more permanent effect, which subsequently affected their subjective health. Participants without disabilities showed a greater rate of recovery. Similarly, participants with lower disability ratings showed a greater rate of recovery. This is thought to be due to the fact that a lingering disability affects one's subjective health. Participants who were employed had a greater rate of recovery compared to their unemployed counterparts, which may be attributed to the potentially positive effects that employment has on one's subjective health, and that people with good objective health tend to participate in economic activities.
The odds of upper middle class participants' recovery were greater than those of the lower middle class and lower class participants. Such findings were consistent when sex, age, educational attainment, tobacco use, alcohol use, pre-accident subjective health, chronic diseases, employment duration, recovery period, accident type, disability status, and economic participation were controlled, indicating that perceived SES affects health recovery.
Our study's strength was that it was a large-scale epidemiological study conducted using 2,000 industrial accident victims. In addition, it is important that the participants were grouped into four classes of perceived SES to examine the relevant characteristics. Additionally, by using ORs for the three socioeconomic classes in which the participants were categorized, the study showed a strong association between the perceived SES and health recovery.
However, our study has several limitations. First, it was a cross-sectional study, and as such, a certain level of recall bias may be present when compared to prospective studies. Second, classification of the participants' perceived SES relied on a single questionnaire, which in itself was based on participant's subjective opinions. Nevertheless, many previous studies have classified participants into SES groups using questionnaires (222831). Furthermore, we considered that the number of participants in our study tempered the limitation. Third, the definition of health recovery in our study was created by the authors. Health recovery is a subjective concept based on an individual's self-perception; thus, it lacks objectivity. Lastly, the definition of health recovery was also based on three questionnaires. However, most research on health relies on questionnaires, because it is the best available research method.
In our study, we verified the association between industrial accident, patients' perceived SES, and recovery. We found that disparity in the perceived SES is associated with disparity in the health recovery of industrial accident patients. Therefore, welfare measures are greatly needed to diminish the perceived socioeconomic disparity and its subsequent impact on health recovery and QOL.
 XML Download
XML Download