

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dementia is a growing public health problem and results in cognitive decline and behavioral problems that lead to impairment in activities of daily living. The prevalence of dementia increases with age, at 24% of persons in the seventh decade of life, and up to 40% of those older than 90 years of age (1).
Early detection of dementia can offer a higher quality of life to both patients with dementia and their families (2). Timely recognition of dementia can give the opportunity to evaluate the reversible causes of memory loss promptly. And it helps patients by allowing treatment in the early stages of dementia, when the cause of dementia is suspected to be a degenerative disease. In case of chronic and progressive disease, early pharmacologic intervention may slow cognitive decline and, by extension, control the worldwide impact of the disease (1).
Many factors associated with a patient's lifestyle factors including socioeconomic status (SES) may disrupt timely access to dementia diagnosis and management (34). As lifestyle factors can have a big impact on disease management and are often modifiable - although it is hard to change, investigation of these factors is important. However, previous studies regarding the association between SES and dementia are inconsistent, and there is currently a paucity of studies (13567). This limited information might result from the use of heterogeneous definitions and measures of SES. Ethnic, racial and cultural diversity may also interfere with an exact assessment of SES (48). Furthermore, the majority of literature only evaluates SES to a certain degree, using education, occupation and income, and excluding social lifestyle characteristics such as living conditions and religious beliefs. An integrated analysis including all lifestyle factors which affect the time of initial dementia diagnosis is needed.
The Seoul Metropolitan Government of South Korea started the Seoul Dementia Management Project to approach the issue of dementia beyond the fragmentary facility care level by setting up the Seoul Metropolitan Center for Dementia in December 2006. The Seoul Dementia Management Project is an integrative management system of dementia and provides greater awareness of the disease, in-advance preventive programs, early diagnosis and proper medical and welfare services according to the stage of dementia (http://www.seouldementia.or.kr/eng). The Seoul Metropolitan Center for Dementia is the general body of the project and provides support for regional centers that administer the actual programs, such as dementia screening tests, registration and memory enhancement programs, in each of the 25 districts in Seoul. Among the project, the Dementia screening test project is a routine population screening project. Through this opportunistic screening program, a Seoulite over 60 years old can be screened for dementia by the Mini-Mental State Examination (MMSE) for free.
The aim of this study was to compare characteristics of lifestyle at the time of initial evaluation for dementia at a single ethnic, racial and cultural environment in urban elderly across degrees of dementia, and to identify risk factors relating to late detection of dementia in order to understand the various lifestyle factors including SES to timely recognition of the disease.
MATERIALS AND METHODS
Participants
The Gwangjin-gu Center for dementia (GCD) is one of the 25 regional Centers for Dementia, which is managed by the Neurology Department of Konkuk University Medical Center. Among many activities of GCD, the early dementia detection project screens at-risk elderly populations within the community and aims at preventing the development of serious dementia by means of effective diagnosis and management of the disease at its early stages. The early dementia detection team of GCD administers large scale screening services targeting approximately 54,715 elderly (older than 65 years) among 380,000 inhabitants.
From May 2009 to November 2013, 35,723 inhabitants were screened. Patients were referred by themselves or by their family members or recruited by the staff of the regional public health center. Additional efforts to include vulnerable patients were made through increased screenings at the GCD. The MMSE was used as the screening tool (9). A total of 1,742 patients were diagnosed with dementia. Diagnosis of dementia was based on the Diagnostic and Statistical Manual of Mental Disorders (4th edition) (10). Assessment included all available patient information, including basic demographic characteristics (e.g., age, sex), SES information, lifestyle information (history of smoking, drinking, physical activity, religious activity and living condition) and global cognitive assessments (Clinical Dementia Rating Scale [CDR] scores). All data were collected during the first visit, on the same day and before screening using the MMSE. Excluded were 333 patients with missing lifestyle information. Therefore, medical records of 1,409 subjects were completely evaluated. Dementia severity was divided into 3 degrees of severity using CDR scores: CDR 0.5 Group; CDR 1 Group; and CDR 2 or 3 Group. In total, 429 mild dementia, 426 moderate dementia and 554 severe dementia patients were included in this study.
Assessment of lifestyle factors and dementia severity
When assessing the SES, education, income and occupation comprised the majority of the evaluation. However, we excluded occupation in this study because less than 5% of our participants had an occupation. Years of education and income were evaluated based on a previous study that revealed that low levels of income and education are due to higher risk behaviors (3). Further factors related to lifestyle characteristics, such as smoking, heavy drinking, physical activity, religion and living conditions were also evaluated.
Information on years of education was ascertained through questionnaires. Years of education was recorded as the highest number of years of schooling and treated as a continuous variable. Information of income was based on the National Health Insurance Contribution, because individual's National Health Insurance Contribution is automatically positioned by the household's whole income in Korea. The low income group was defined as patients who earn 0 through 603,403 KRW for 1 person; 0 through 1,027,417 KRW for 2 persons; 0 through 1,329,118 KRW for 3 persons; 0 through 1,630,820 KRW for 4 persons and 0 through 1,932,522 KRW for 5 persons, as this is the cut-off amount below 40% of median value of Korean's income. The high income group included all the other incomes. Smoking was coded as 'never' smoked or 'past or current' smokers based on self-reporting. Heavy drinking was based on self-reporting of the daily consumption of more than 3 glasses of any alcoholic beverage and grouped into 2 categories: 'never' or 'past or current' drinking. Physical activity was categorized as a physically inactive group, which consisted of patients who did not do either 20 minutes of vigorous activity on 3 or more days or 30 minutes of moderate activity on 5 or more days per week, or a physically active group. Religion was categorized as an active religious group that believed in some type of religion and attended a place of worship more than once per week and a non-religious group that included atheists or religious believers who did not participate in any religious activities. Living conditions were grouped into 3 categories: alone; with spouse; with family other than spouse.
Statistical methods
The Spearman correlation analysis was used to examine the relationship between factors. The statistical significance of differences of group means was determined by one-way analysis of variance (ANOVA) with post hoc analysis by Tukey's multiple comparison test. For non-parametric variables, group comparisons were done using the Kruskall-Wallis test and the Mann-Whitney U test. SPSS (version 17.0, SPSS Inc., Chicago, IL, USA) was used and P < 0.05 was considered as the threshold of significance.
We used a multiple logistic regression model to identify risk factors associated with lifestyle factors relating to late detection of dementia. Although this is a cross-sectional study, the lifestyle factors usually precede the dementia and risk factors of dementia. So we regarded the lifestyle factors as independent variables and the severe dementia as a dependent variable. For the logistic model, we combined the CDR 0.5 Group and CDR 1 Group as a non-severe dementia group and compared this group with the CDR 2 or 3 Group. As CDR 2 states 'severe memory loss; only highly learned material retained; severely impaired in handling problems, and social judgement', we defined the patients CDR 2 and over at the time of initial evaluation as 'severe' dementia group (SG) in the logistic model; the representative group for late detection.
RESULTS
Demographics and clinical characteristics
The prevalence of dementia in Gwangjin-gu district was 4.8%. There were significant differences in age, sex and lifestyle factors (except for income) between the 3 groups (Table 1). There was a significantly greater proportion of individuals who were old age, female, less educated, who had never smoked or drank heavily, without physical activity, without religious activity and living with family other than spouse in the CDR 2 or 3 Group (P < 0.001). Income did not influence severity at the first time of diagnosis (P = 0.098), although post-hoc analyses found a significant difference when comparing only the CDR 0.5 Group and CDR 2 or 3 Group (P = 0.049). In comparison with the CDR 0.5 group, all variables were significantly different in the CDR 2 or 3 Group.
Table 1
Demographics and socioeconomic and lifestyle characteristics

Values are mean (standard deviation) and numbers (%) in continuous and categorical variables, respectively.
CDR, clinical dementia rating.
![]()
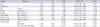
Age, years of education, history of heavy drinking, physical activity, religious activity and living condition were variables that were appropriate to a logistic model for the SG (Table 2). Odds ratios (OR) of severe dementia were 1.045 (95% confidence interval [CI], 1.026-1.064) for age and 0.956 (95% CI, 0.926-0.986) for years of education. The risk of severe dementia at initial diagnosis was decreased for those who had history of drinking (OR, 0.507; 95% CI, 0.310-0.830) or who were physically (OR, 0.271; 95% CI, 0.182-0.405) or religiously active (OR, 0.454; 95% CI, 0.348-0.592). Patients who lived with a spouse (OR = 2.044; 95% CI, 1.251-3.340) or family other than a spouse (OR = 3.549; 95% CI, 2.291-5.493) had a higher risk of diagnosis for severe dementia at the initial evaluation than those who lived alone.
Table 2
Results from logistic regression final model: correlates of severe dementia at initial presentation (method 'enter')
![]()
DISCUSSION
In the present study, there were significant differences in all lifestyle factors except income between the three groups. The differences in these characteristics between the 3 groups were prominent and more noticeable when the CDR 0.5 Group was compared to the CDR 2 or 3 Group. The impact of various lifestyle factors on the initial clinical presentation was also examined. An older age, low education, history of never drinking, physical inactivity, no religious practices and living with a spouse or family other than a spouse were much more common in the late detection group represented as SG at the time of first screening of urban elderly.
While previous literature reported that the prevalence of dementia is higher among individuals with older age and low educational years (61112131415), our study identified the impact of aging and education on screening test. We found an inverse relationship between dementia severity and education, consistent with a previous study that reported decreasing education was associated with greater severity of disease at presentation (15). This is because individuals with less education may be less likely to be involved in cognitive tasks or occupational roles where subtle changes in cognitive functions could be detected and lead to an earlier diagnosis (1516). Moreover, the low self-perception of the dementia could be the cause of late detection in less-educated people.
Our findings are inconsistent with a previous study, in that an economic barrier was the only category to correlate with a delayed diagnosis (4). As income information was based on the Korean medical insurance system, which supports medical expenses for certain low-income brackets through the National Health Insurance Corporation and, operated by the Ministry of Health and Welfare in Korea, it is regarded the accuracy of the reports as good. The impact of income might be much attenuated in our study because the purpose of the Seoul Dementia Management Project is 'screening' to detect patients in early stages of dementia. So we can only interpret that low income is not a screening barrier among Seoul elderly, or 'screening' project of GCD is working well.
Factors which are associated with being a social outsider, such as non-drinking, physical inactivity and religious inactivity were the barriers to timely access to healthcare services. The roles of smoking and alcohol on the development of dementia remain controversial (171819). Moreover, the relationship between alcohol consumption and dementia 'detection' is rarely evaluated. Our study showed a reduced risk of late detection in patients who were past or current heavy drinker. Drinking could be interpreted as a surrogate marker of social interactions. Social interaction is significantly correlated with alcohol use measures, even after controlling for SES and demographic variables (20). Drinking is the indicator of social interaction which is more strongly associated than classical SES (21). As activities of drinking can include certain cognitive tasks and social interactions, patients who never drank may have had a delay in medical attention until the disease had progressed to dementia. More detailed investigations about drinking patterns, such as beverage preferences, place where people drink, alcohol consumption periods or change of social, occupational, and recreational pursuit due to alcohols, are required. The non-smoking, however, was not a factor of late detection. Smokers usually smoke alone, so the social networking is much weak in smoking or smoking is related with less neighbourhood social capital.
The finding that patients with dynamic religious activity had a lesser chance of being diagnosed with severe dementia than patients who are non-religious continues in the same vein with social interaction. Participating in religious activities requires social interaction and strategies that involve executive functioning (2223). Religious activity could be one of another social interaction marker, so absence of this religious activity might make the people alienated, and leads the dementia symptoms concealed.
Our finding of an inverse relationship between physical activity and the severity of dementia is consistent with many previous studies (242526). As physical inactivity increased the risk of daily activity limitations, dementia patients with physical inactivity may not seek medical attention until the disease has progressed.
Living conditions (including marital status) showed interesting findings. Patients who lived alone had a much lesser risk of late detection than those who live with family. Previous reports showed that the loss of insight that accompanies dementia could result in patients who lived alone being diagnosed late (2728). However, we considered that daily activity impairment, which accompanies dementia, may put patients who lived alone in a clinically challenging situation. As patients who live alone have to do their all daily activity by themselves, subtle cognitive decline could be detected early. Moreover, elderly who live with family are used to being dependent even simple daily activity on others and take these offers for granted, owing to the Korean tradition of Confucianism. This trend is intensified when there is no spouse and only other family. Limited daily duty is connected to the delayed attention for medical services.
A limitation of the present study includes some investigation based on self-reporting, although the contents were well-constructed and standardized. Another limitation is the limited diversity, in that the study was performed at single ethnic, racial and cultural environment of the urban elderly. There were ethno-racial and cultural differences in clinical characteristics (48). We could not reflect these characteristics; however, this is rather strength of the present study as the lifestyle factors could be investigated more precisely. The cross-sectional design of this study could be another limitation. Regarding the lifestyle factors as independent could be problem, because severe dementia makes the patients' lifestyle inactive. However, we think the categorizing factors as 'never' or 'past or current' can compensate the defect. The older age of the the CDR 2 or 3 Group could make us think about the survival bias. Furthermore, this result could only be applicable to the 'screening' target, not to the patients who visit the memory clinic voluntarily. Finally, much more female patients than male in our study could create bias which can alleviate the effect of the sex.
Recent reports from the United States Preventive Services Task Force doubt the value of universal screening using formal screening instruments for community-dwelling adults, over age 65 years, in the general primary care population who have no signs or symptoms of cognitive impairment, although the risk versus benefit of screening cannot as yet be determined (2930). However, the screening test is an indispensable tool in the diagnosis of dementia. Also, timely diagnosis of dementia can improve the quality of life for both patient and caregivers (214). Costs of care for patients with mild dementia are significantly lower than for those with moderate dementia (31), and the effect of cognitive enhancers are better when given during mild to moderate stages of dementia compared with severe stages (143233).
In a Korean report analysing the cost-effectiveness of nationwide opportunistic screening program for dementia, the screening project of the Seoul Metropolitan Government did not lead to cost savings for the present (34). Among the several factors, screening all individuals over 65 years who want the test, not targeted to the patients with high risk, was thought to be the main factor. That is, to find out the vulnerable stratum to dementia screening is a cost-effective way to promote health of urban elderly. In the present study, the differences in lifestyle characteristics according to dementia severity and variables related to severe dementia on initial clinical presentation when screening test were examined. Our results suggest that certain lifestyle factors; aging, lower education, less social interactions (drinking, religious activity), less physical activity or living with family who serve the elderly's daily activity are associated with late disease detection. The “severe-stage-at-the-time-of-first-evaluation” means patients were in a “blind spot” in the healthcare system. We can define this group as the vulnerable stratum to dementia evaluation, including screening. Health policy or community health services might find ways to better engage patients in this vulnerable stratum to dementia.
This study provides evidence of the significant societal cost of dementia. The study also provides a rich body of information on the health services and cost of dementia that is essential for policy analysis and formulation as well as the basis for future planning for services of elderly population.
 XML Download
XML Download