

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Acute inflammatory gallbladder (GB) diseases without gallstone, including acute acalculous cholecystitis (AAC), are relatively uncommon in pediatric patients. Therefore, they are not initially considered in children who complain of gastrointestinal (GI) symptoms such as abdominal pain and vomiting (123). However, the incidence of acute inflammatory GB diseases has been increasing as diagnostic technology develops and medical concern over such diseases increases (123).
While most acute inflammatory GB diseases in adult patients involve calculus cholecystitis, acute acalculous GB diseases are more common in pediatric patients, accounting for approximately 30%–50% of cases, which is much higher than in adults (1456). Although the prognosis of acute acalculous GB diseases is relatively good in most cases, early and accurate diagnosis is important. Surgical correction may be required in some cases and serious medical complications, including septic shock or death, may develop in patients with underlying disease or when misdiagnosis occurs (17).
Furthermore, the diagnosis of acute GB diseases in the early stage is difficult because the symptoms are nonspecific and Murphy’s sign, a clinical manifestation of the presence of cholecystitis, is difficult to detect, especially in the pediatric population. Thus, abdominal ultrasonography (USG) is considered the most accurate diagnostic modality because it is cost-effective, free of radiation hazard, and highly specific to the biliary system (38). Acute acalculous inflammatory GB diseases on abdominal USG have been found in association with a variety of conditions such as structural abnormality, systemic disease, and systemic infection in the pediatric population (39). Therefore, it is often critical that clinicians diagnose the underlying disease in acute inflammatory GB diseases without gallstone because it may cause abnormal GB findings on USG and affect the clinical outcome of acute acalculous inflammatory GB disease.
To date, most studies on acute acalculous GB disease have been done in adults, and there are only a few studies on pediatric patients. In these studies on children, individual conditions such as Kawasaki disease, Epstein-Barr virus (EBV) infection, and nephrotic syndrome were merely discussed rather than a comprehensive analysis of acute acalculous inflammatory GB disease and its underlying causes (10111213141516).
Predisposing diseases of acute inflammatory GB disease in pediatric patients are very different from those in adults. However, to our knowledge, there has been no study on the relationship between clinical features, predisposing diseases, and ultrasonographic findings and the clinical outcome of acute acalculous inflammatory GB disease in a pediatric population to date.
Therefore, in this study we evaluated clinical factors such as age, gender, predisposing diseases, and ultrasonographic findings that might determine clinical outcome of acute acalculous inflammatory gallbladder diseases in children.
MATERIALS AND METHODS
Patient selection and data extraction
A total of 131 children hospitalized with hepatobiliary symptoms such as abdominal pain, jaundice, and abnormal liver function tests and diagnosed with acute acalculous inflammatory GB disease by USG between March 2004 and February 2014 at Seoul National University Bundang Hospital were included in the study. Clinical symptoms, predisposing diseases, and ultrasonographic findings were retrospectively reviewed and analyzed. Patients who had other chronic diseases of the hepatobiliary or GI system were excluded. In order to eliminate possible total parenteral nutrition-induced cholestasis, patients receiving intravenous nutrition were also excluded from the study.
The patients were categorized into four groups according to the age stages developed by the Eunice Kennedy Shriver National Institute of Child Health and Human Development: infancy (0–2 years of age), early childhood (2–5 years of age), middle childhood (6–11 years of age), and early adolescence (12–18 years of age) (17).
Predisposing diseases
Predisposing diseases were divided into six categories: 1) noninfectious hepatobiliary disease; 2) systemic infectious disease including sepsis, viral or bacterial infection; 3) abdominal disease related to GI tract; 4) extra-GI tract disease of the kidney, lung, or heart; 5) noninfectious systemic disease such as Kawasaki disease; and 6) malignancy (Table 1).
Table 1
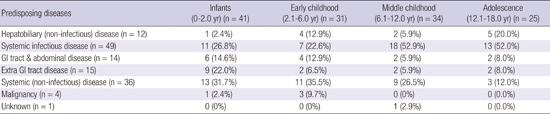
Predisposing diseases of acute inflammatory gallbladder disease without gallstone in children and adolescents

Predisposing diseases were determined based on patient medical records. Clinical symptoms, physical examinations findings, and diagnostic test results such as serologic tests, urinalysis, blood and urine cultures, polymerase chain reaction, computed tomography, and abdominal USG were thoroughly reviewed retrospectively for all study participants.
Ultrasonographic diagnosis of acute acalculous inflammatory GB disease
Abdominal USG was performed by expert pediatric radiologists on children with hepatobiliary symptoms during the acute disease stage. Initial ultrasonographic findings and interpretations were reviewed by another expert pediatric radiologist and an expert pediatric gastrointestinal hepatologist. The diagnosis of acalculous GB disease by USG was made according to 4 criteria 1) GB distention, 2) GB wall thickness > 3.5 mm, 3) nonshadowing echogenic sludge, and 4) pericholecystic fluid collections (8).
RESULTS
Predisposing diseases of acute inflammatory GB disease without gallstone in pediatric patients are listed in Table 1. Systemic infectious diseases such as EBV infection were the most common etiology of acute acalculous inflammatory GB disease and were identified in 50 patients (38.2%). Noninfectious systemic diseases including Kawasaki disease were also a common etiology and were identified in 35 patients (26.7%). Kawasaki disease was the most common predisposing disease in children with acute acalculous GB disease and was diagnosed in 28 out of 131 patients (21.4%). In one patient, a specific etiology could not be identified despite abnormal GI findings on USG compatible with acute acalculous GB disease.
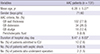
Clinical and ultrasonographic features of pediatric patients (mean age, 6.28 ± 5.27 years; 71 boys and 60 girls) with acute acalculous GB disease are described in Table 2. Of the ultrasonographic criteria for the diagnosis of acute acalculous inflammatory GB disease, significantly thickened GB wall was found in 102 of 131 patients (77.9%); GB distension, GB sludge, and pericholecystic fluid were identified in 34 (26.0%), 16 (12.4%), and 9 (6.9%) patients, respectively. Of the 131 patients, 10 (7.6%) were admitted to the intensive care unit (ICU), and the mean length of ICU stay was 0.63 ± 3.40 days. The primary reason for ICU admission was septic shock complicated by acute inflammatory GB disease, which occurred in 6 patients without a predominant gender represented. Two of 131 (1.5%) children underwent laparoscopic cholecystectomy for acute acalculous GB disease. The one patient was later diagnosed with EBV associated cholecystitis and the other was not found specific etiology of acute acalculous inflammatory GB disease.
Table 2
Clinical and ultrasonographic features of pediatric patients with acute acalculous gallbladder disease
Analysis of the age distribution of pediatric patients revealed that acute acalculous GB disease was most prevalent in infants aged ≤ 1 year and the number of patients diagnosed with acute acalculous GB disease was decreasing as age increased (Fig. 1). The age groups were associated with significantly different predisposing diseases of acute acalculous GB disease; noninfectious systemic diseases were the most prevalent etiology in infancy and early childhood, whereas systemic infectious diseases were the most prevalent in middle childhood and adolescence (P = 0.001) (Table 3).
Fig. 1
Age distribution of pediatric patients with acute acalculous inflammatory gallbladder disease. Acute acalculous gallbladder disease is most prevalent in infants aged ≤ 1 year. The number of patients diagnosed with acute acalculous gallbladder disease is decreasing as age increased.
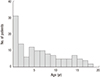
Table 3
Predisposing diseases according to the age group in pediatric patients with acute acalculous gallbladder disease

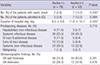
Clinical manifestations and ultrasonographic findings of each underlying disease of acute acalculous GB disease are described and compared in Table 4. There was a significant gender difference among the diseases predisposing to acute acalculous GB disease in children, with a male predominance found in extra-GI diseases (86.7%) and noninfectious systemic disease (65.7%) (P = 0.026). There was no statistically significant difference in the duration of hospitalization, the number of patients admitted to the ICU, or the duration of ICU stay (P = 0.212, 0.964, and 0.748, respectively); however, malignancy was associated with the longest hospital and ICU stay among predisposing diseases. Thickened GB wall was more commonly found in cases of acute acalculous GB disease caused by malignancy (100%) and systemic infection (94.0%) compared to other causes (P = 0.002) (Table 4). Conversely, GB distension on ultrasound was most frequently seen in acute acalculous GB disease caused by noninfectious systemic diseases such as Kawasaki disease (60%), but it was uncommon in cases caused by systemic infection (6.0%) and malignancy (0%) (P = 0.000).
Table 4
Comparison of clinical manifestations and ultrasonographic findings according to predisposing disease in children and adolescents with acute acalculous gallbladder disease

There were no significant differences in the number of patients admitted to the ICU, those who developed septic shock, and those who underwent surgery according to ultrasonographic GB abnormalities (P = 0.719, P = 0.237, and P = 0.572, respectively).
Ascites was noted in addition to GB abnormality on USG in 53 (40.5%) patients. Septic shock and transfer to the ICU, which are indicative of a poor clinical course, were more common when ascites was present on USG (13.2% vs. 2.6%, P = 0.030 and 13.2% vs. 3.8%, P = 0.089), and the duration of hospitalization was longer in patients with ascites on USG (11.6 ± 10.7 vs. 8.0 ± 6.6 days, P = 0.020). However, there were no significant differences in predisposing diseases according to the presence of ascites on USG (P = 0.715) (Table 5).
Table 5
Clinical outcomes, predisposing diseases, and ultrasonographic findings according to the presence of ascites in pediatric patients with acute acalculous gallbladder disease
DISCUSSION
Most research on acute acalculous GB disease has been conducted on adult patients to date, and the studies that have been done on pediatric patients only discuss individual diseases and have small sample sizes (10111213141516). The present study included 131 pediatric patients with acute acalculous GB disease and evaluated not only predisposing diseases in children and adolescents but also the differences of the predisposing diseases by age group. Clinical aspects and ultrasonographic findings of each predisposing disease and classification of clinical characteristics according to abnormalities found on USG of the GB were also identified for the first time in this study.
Systemic infection was the most common predisposing disease of acute acalculous GB disease in children and adolescents in our study. EBV infection was the most prevalent infectious disease followed by hepatitis A virus infection. To date, several case reports on EBV-associated acute acalculous GB disease have been published (131415). EBV-associated cholecystitis appears to be more prevalent in children than in adults because EBV infection rarely develops in patients > 25 years of age (18). In this study, we identified acute acalculous GB disease cases caused by 7 different viral infections in patients with no other predisposing causes; these require further research using diagnostic tests such as polymerase chain reaction.
In our study, there were 28 cases of Kawasaki disease, which was the most prevalent predisposing disease. Kawasaki disease with GB distension is associated with an increased risk of coronary artery complications as discussed in our previous report (12). Therefore, an aggressive diagnostic and treatment plan should be considered when the diagnosis of acute acalculous GB disease is confirmed by USG in pediatric patients manifesting with atypical symptoms of Kawasaki disease (12).
In previous studies, GB perforation has been found predominantly in men (1920); however, in the present study, 4 patients, all female, were treated surgically for acute acalculous disease without perforation. Female dominance of type III perforation, which develops mainly in patients < 50 years of age, has previously been reported (1920). Nevertheless, it has not yet been established whether this indicates that clinical manifestations of acute acalculous GB disease differ by gender or it is merely a coincidental finding. Further research should be considered as more cases are found.
Analysis of predisposing diseases by age group in the present study revealed that systemic noninfectious diseases including Kawasaki disease predominate in infancy and early childhood. This is consistent with previous reports that Kawasaki disease occurs mainly in early childhood (21). Systemic infectious disease was the most common predisposing disease in middle childhood and adolescence in our study. Bacterial or viral infection such as EBV and hepatitis A virus that invade the hepatobiliary system are most commonly found in these age groups (18).
Unlike calculus cholecystitis, acute acalculous GB disease is known to occur slightly more frequently in males, which corresponds with our findings (522). However, female predominance was noted in the cases related to noninfectious hepatobiliary disease and systemic infectious disease in our study. Similar results have been reported in previous studies on EBV-associated cholecystitis; however, it has not yet been determined why this occurs (1418).
In the present study, the prognosis of cholecystitis was relatively good regardless of the predisposing disease. Only one patient underwent surgery, which was performed by a surgeon who was contacted in the emergency room at night, although the clinical signs and symptoms were not severe. The patient was later diagnosed with acalculous cholestatic hepatitis due to EBV infection. As reported by Arya et al. (14), excellent recovery without surgical treatment is generally expected in patients with EBV-associated cholecystitis. Therefore, determination of the appropriate treatment approach may depend on an accurate diagnosis of the predisposing disease in cases of acute acalculous GB disease in children.
The prognosis of acalculous GB disease associated with other predisposing diseases was also good, and clinical signs and symptoms improved with appropriate, nonsurgical medical treatment in most cases. Our previous study on Kawasaki disease-associated AAC also found that a good prognosis is expected with medical treatment (10). Huang and Yang (1) also commented that they treated all of their AAC patients medically despite a higher mortality rate in patients with septic shock and hypofibrinogenemia. Complications, including spontaneous perforation within 72 hours, can occur as acute acalculous GB disease develops as described by Karkera et al. (19). However, the incidence of complications is negligible, especially in the pediatric population. Unlike adults with AAC or calculus cholecystitis, a nonsurgical approach should be the primary consideration in pediatric patients with acute acalculous inflammatory GB disease. Further studies are required to confirm this.
Ultrasonographic findings of GB differed according to predisposing disease in our study. Increased GB wall thickness was noted in most patients (77.9%) in our study. It is not coincidental that systemic infection was the most common predisposing disease in our patients and that most of them had thickened GB wall. In systemic viral infections, it is hypothesized that viral antigens invade the GB wall directly, which leads to its thickening. According to Mourani et al. (23), immunohistochemical methods revealed viral antigen in the walls of GB removed from patients diagnosed with hepatitis A virus-associated cholecystitis. The pathogenic mechanism in EBV and other viral infections is thought to be direct invasion of vial antigen into GB walls (182324).
Interestingly, in our study, approximately 60% of the patients diagnosed with a systemic noninfectious disease, including Kawasaki disease, as the predisposing disease were found to have GB distension on abdominal USG. Although the underlying cause of this finding is not certain, hypertrophied inflamed nodes may cause obstruction and reactive inflammation of the cystic duct, which leads to acalculous GB distension (25).
In systemic diseases, factors such as ileus, and dehydration can worsen serositis of the GB and accompanying bile stasis, which frequently leads to GB wall distension (26). Thus, many patients (54.4%) with systemic disease were found to have thickened GB wall on abdominal USG in our study. It has been suggested that elevated portal and systemic venous pressure or decreased intravascular osmotic pressure may be the cause of this finding, although the pathophysiologic mechanism remains unclear (2627).
Although there were no significant differences in clinical outcome according to sonographic GB abnormality in our study, the occurrence of septic shock and transfer to the ICU suggestive of poor clinical courses were significantly associated with the presence of ascites on USG. Additionally, the total duration of hospitalization was significantly longer when ascites was found on USG in our study. Therefore, it may be prudent to look for other findings on abdominal USG, especially the presence of ascites in addition to a GB abnormality in pediatric patients.
The results of the present study, despite its limitations, revealed for the first time that age group, predisposing diseases, and ultrasonographic findings affect the clinical outcome of acute inflammatory GB disease without gallstone in children. Our results indicate that acute acalculous GB disease is more prevalent in infancy and that acute acalculous GB disease in middle childhood or adolescence is most often accompanied by systemic infection that manifests as increased GB wall thickness on USG.
In conclusion, acute acalculous GB disease without gallstone is more common in pediatric patients than has been previously reported, and its incidence in infancy is higher than previously thought. The predisposing cause differs by age group, and abdominal ultrasonographic findings vary depending on the predisposing disease. Simultaneous consideration of age, predisposing diseases, and the presence of ascites as well as abnormal GB findings on abdominal USG at initial diagnosis would be helpful to avoid unnecessary medical complications or surgical treatment, which are all preventable with proper management. Furthermore, a serial USG examination is important to assess acute acalculous GB diseases associated with severe illness for better clinical outcomes. In children with acute acalculous GB disease, medical treatment should be considered the treatment of choice before surgical approaches because its associated prognosis is generally good in all pediatric age groups. Applying this new systematized strategy may lead to improved prognosis in children and adolescents with acute inflammatory GB disease without gallstone.
 XML Download
XML Download