

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Acute gastrointestinal bleeding is a common cause of hospital admission and life-threatening medical emergency in many countries (12). Gastrointestinal bleeding can be classified into upper- or lower-gastrointestinal bleeding (UGIB or LGIB) on the basis of anatomical location (3456). Risk factors for clinical outcomes for patients with UGIB have been widely investigated (78910); however, little is known about the risk factors for clinical outcomes in patients with LGIB, despite a rising incidence (68).
In a Spanish population-based study (4), patients with LGIB had longer hospital stays and higher mortality rates compared to patients with UGIB. Furthermore, the patients with LGIB showed a significantly increasing trend of hospitalization due to lower-gastrointestinal events in comparison to a decreasing trend of hospitalization due to upper-gastrointestinal events in patients with UGIB. However, the authors of the study analyzed bleeding and perforation together, and therefore the clinical outcomes of LGIB alone remain to be determined. To date, no studies have compared the risk factors of clinical outcomes in patients with LGIB versus UGIB, especially in Asian population.
The aim of this study was to identify the clinical outcomes and the predictors of poor outcomes for patients with LGIB, compared to outcomes for patients with UGIB.
MATERIALS AND METHODS
Patients
We retrospectively studied patients with UGIB or LGIB, who underwent upper endoscopy and/or colonoscopy with or without intervention between July 2006 and February 2013 at the Kyung Hee University Hospital in Gangdong, Seoul, Korea. Patients were considered eligible for the study if they had upper endoscopy and/or colonoscopy with a history of hematemesis, melena, hematochezia, anal bleeding, occult bleeding, or a combination of these symptoms. Patients who initially visited another hospital for the bleeding episode and were subsequently transferred to our hospital were included as long as no intervention had been performed. Data regarding transfers to and from other institutions and readmission were also collected. Patients with esophagogastric variceal bleeding and obscure gastrointestinal bleeding were excluded from the database. We compared the risk factors of clinical outcomes for patients with LGIB to those for patients with UGIB. The database of eligible consecutive patients was reviewed for the following information: demographic data (age, sex), historical data (smoking, alcohol, presenting signs or symptoms, comorbidity, relevant medical history, date of endoscopy, and any concomitant intake of medications on presentation), physical examination findings, and laboratory data. The endoscopic report included the specialty of the endoscopist, identification of the bleeding lesion, methods of endoscopic hemostasis, and timing and outcomes of endoscopic intervention.
Patients with acute gastrointestinal bleeding were managed according to the guidelines of the American College of Gastroenterology and the American Society for Gastrointestinal Endoscopy (111213). According to guidelines for UGIB, high-dose proton pump inhibitor (pantoprazole 80 mg bolus followed by 8 mg/hr infusion) was routinely administered to most patients with UGIB. All patients were monitored from the time of hospital admission up to 30 days after the endoscopic procedure for 30-day rebleeding or mortality. The decision of whether to administer antithrombotic drugs was left to the discretion of the attending physician. In general, antithrombotic drugs were resumed as soon as possible after the endoscopic procedure for secondary prevention (within 1–3 days for most patients); however, antithrombotic drugs were not used for primary prevention. Uncontrolled bleeding despite endoscopic hemostasis was usually considered an indication for angiographic embolization or surgery.
Definition of variables
UGIB was defined as bleeding within the reach of an upper endoscopy, whereas LGIB was defined as bleeding distal to the reach of colonoscopy (1415). Endoscopic intervention was considered complete when endoscopic hemostasis at the bleeding site was successful, and active bleeding was stopped during the first endoscopic intervention.
Thirty-day rebleeding was defined by recurrent hematemesis, hematochezia, fresh anal bleeding or both, together with either the development of hemodynamic instability or a decrease in hemoglobin concentration at least 2 g/L following initial successful treatment and stabilization within 30 days of the initial bleeding episode. Thirty-day mortality was defined as any death occurring within 30 days of the initial bleeding episode. Major comorbidity was defined as liver cirrhosis, chronic renal failure, end-stage renal disease or malignancy, on the basis of a previous study (16). For risk stratification, the Glasgow–Blatchford score (GBS) and the clinical Rockall score were generally used as described previously (1718). The clinical Rockall score consists of pre-endoscopic variables: age, shock, and comorbidity (17). The GBS score includes the following five variables: blood urea levels, hemoglobin levels, systolic blood pressure, and other markers (heart rate, melena, syncope, hepatic disease, and cardiac failure) (18). We used a modified GBS score for patients with LGIB, substituting hematochezia instead of melena.
Statistical analyses
The primary outcome measures were 30-day rebleeding and mortality rates for patients with LGIB or UGIB. The secondary outcome measures were predictive factors for the 30-day rebleeding and mortality.
Categorical data are expressed as number (percentage), whereas continuous data are expressed as mean ± standard deviations. A two-tailed Student’s t-test was used for continuous variables, and a two-tailed χ2 test or a Fisher’s exact test was used for categorical data. Univariate logistic regression analysis was performed to determine independent risk factors of rebleeding or mortality, and odds ratios (ORs) and 95% confidence intervals (CIs) were calculated. All P values were two tailed, and a P value < 0.05 was considered statistically significant. Data analyses were conducted using SPSS software, version 21.0 (SPSS, Chicago, IL, USA).
Propensity score matching was used to improve the comparability between the LGIB and UGIB groups using the following variables: age, sex, major comorbidity, experience of the endoscopist, and ulcerogenic medications (such as nonsteroidal anti-inflammatory drugs [NSAIDs], anti-platelet agent, or anticoagulants), which can influence the outcomes of the patients (19). After estimating propensity scores, participants were matched based on a 2:1 nearest-neighbor algorithm by SPSS-R plugin software. This resulted in 303 matched pairs without significant imbalances (|d| > 0.25) in the covariates utilized.
RESULTS
Baseline patient characteristics
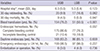
During the study period, a total of 837 patients with UGIB or LGIB were identified, and 236 patients were excluded due to insufficient medical records. Therefore, 601 patients with UGIB (n = 500) or LGIB (n = 101) were finally analyzed. After 2:1 propensity score matching, 202 patients with UGIB and 101 patients with LGIB were identified as matched pairs. The clinical and laboratory characteristics of these matched pairs are summarized in Table 1; the pairs are well balanced for the variables, including age, sex, comorbidity, experience of the endoscopist, and ulcerogenic medications. After matching, the modified GBS score was significantly lower in the LGIB group than in the UGIB group (P < 0.001); however, the Rockall score was only marginally lower in the LGIB group than in the UGIB group (P = 0.051). The patients with UGIB had significantly lower systolic/diastolic blood pressure, higher heart rate and lower hemoglobin levels than patients with LGIB.
Table 1
Clinical and laboratory characteristics of patients with lower or upper gastrointestinal bleeding before and after propensity score matching

UGIB, upper gastrointestinal bleeding; LGIB, lower gastrointestinal bleeding; GBS score, Glasgow–Blatchford score; SD, standard deviation; NSAID, nonsteroidal anti-inflammatory drug; SBP, systolic blood pressure; DBP, diastolic blood pressure; APC, argon plasma coagulation.
*Other endoscopic hemostasis included band ligation and beriplast injection.
![]()
Clinical outcomes
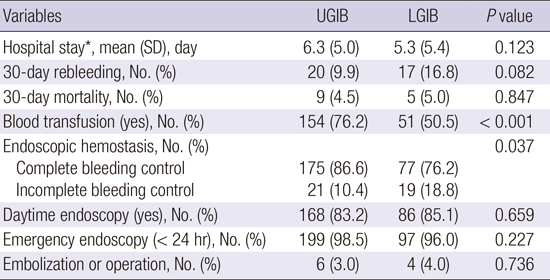
The mean duration of disease-related hospital stay was comparable in both groups (P = 0.123; Table 2). The most common causes of LGIB were postpolypectomy bleeding, diverticular bleeding, malignancy, Dieulafoy's lesion, and hemorrhoid, while, in UGIB, peptic ulcer, Mallory-Weiss tear, malignancy, Dieulafoy's lesion, and angiodysplasia were the most common causes in our center.
Table 2
Clinical outcomes of patients with upper or lower gastrointestinal bleeding
UGIB, upper gastrointestinal bleeding; LGIB, lower gastrointestinal bleeding; SD, Standard deviation.
*Twenty-six patients were excluded from this analysis as they experienced gastrointestinal bleeding during admission at another department, which affected the duration of hospital stay.
![]()
The 30-day rebleeding and mortality rate were 9.9% and 4.5% for the UGIB group and 16.8% and 5.0% for the LGIB group, respectively (Table 2). Although the 30-day rebleeeding rate was higher in the LGIB group than in the UGIB group, no statistically significant difference was found between the two groups for 30-day rebleeding or mortality rate. Successful endoscopic hemostasis was significantly higher in the UGIB group compared with the LGIB group (86.6% compared with 76.2%, P = 0.037). Hemoclip application was the most frequently used endoscopic hemostasis in patients with LGIB, whereas hemoclipping and a combination of hemostatic methods were used more frequently in patients with UGIB.
Risk factors for 30-day rebleeding and mortality
The results of univariate analyses of possible risk factors, including age, sex, major comorbidity, Rockall score, GBS/modified GBS score, hemoglobin, and C-reactive protein (CRP) levels, for 30-day rebleeding and mortality in patients with UGIB or LGIB are summarized in Table 3 (rebleeding) and Table 4 (mortality). For 30-day rebleeding, no risk factors were identified in the LGIB group; and only the GBS score correlated significantly with rebleeding in the UGIB group (OR = 1.231, 95% CI, 1.029–1.472; P = 0.023; Table 3). For 30-day mortality, the Rockall score (OR = 2.081, 95% CI, 1.170–3.700; P = 0.013) and CRP levels (OR = 1.174, 95% CI, 1.002–1.376; P = 0.047) were identified as risk factors in the LGIB group; however, the Rockall score, GBS score, hemoglobin, and CRP levels were all identified as risk factors in the UGIB group (Table 4).
Table 3
Predictable risk factors for 30-day rebleeding in patients with upper or lower gastrointestinal bleeding
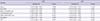
UGIB, upper gastrointestinal bleeding; LGIB, lower gastrointestinal bleeding; OR, odds ratio; CI, confidence interval; GBS score, Glasgow–Blatchford score; CRP, C-reactive protein.
![]()
Table 4
Predictable risk factors for 30-day mortality in patients with upper or lower gastrointestinal bleeding
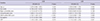
UGIB, upper gastrointestinal bleeding; LGIB, lower gastrointestinal bleeding; OR, odd ratio; CI, confidence interval; CRP, C-reactive protein.
![]()
DISCUSSION
Patients with acute gastrointestinal bleeding have significant medical problems, including morbidity, rebleeding and mortality. Previous studies have found that age, sex, comorbid conditions, and NSAIDs use were significant predictors of rebleeding and mortality for LGIB (20212223), but they have lacked the power to clarify. Compared to outcomes for patients with UGIB, little attention had previously been paid to outcomes for patients with LGIB, and risk factors for rebleeding and mortality were unknown. In this study, the duration of hospital stay and 30-day mortality rate of patients with LGIB were similar to those of patients with UGIB. Furthermore, the 30-day rebleeding rate of the LGIB group was higher than that of the UGIB group (16.8% compared with 9.9%), although statistical significance was not reached (P = 0.082). Therefore, the clinical outcomes for patients with LGIB are no better than the clinical outcomes for patients with UGIB. Our findings may be explained by the lower rate of successful endoscopic hemostasis in patients with LGIB than in patients with UGIB (76.2% compared with 86.6%, P = 0.037). In the management of LGIB successful endoscopic hemostasis is more difficult because of the low diagnostic rate of the definite source of bleeding (24). More careful risk stratification is necessary for patients with LGIB as they have poor clinical outcomes despite more stable vital signs compared to patients with UGIB; the LGIB group had higher blood pressures, stable heart rates, higher hemoglobin levels, lower clinical Rockall scores, and lower modified GBS scores.
To date, many risk stratification models for predicting clinical outcomes in patients with UGIB have been suggested (791025); however, only a few studies have investigated patients with LGIB, and the results are inconsistent (6202627). The accurate identification of high-risk patients during the assessment of patients with LGIB has therefore been difficult. The BLEED classification tool (28), developed and validated in the United States, has been used to predict poor prognosis for patients with LGIB or UGIB (28); however, it is too complex to be applied practically in a clinical setting. The Rockall score (17) and the GBS score (18) are used most widely to predict risk, especially of rebleeding and mortality, for patients with UGIB (2930). It has been suggested that the same variables included in both the Rockall and GBS models for UGIB (9101718) could be included in a risk-prediction model for LGIB (272831). So, it might make sense to apply these scoring systems to the prediction of high-risk patients with LGIB, even though neither system has been evaluated in patients with LGIB. In this study, the clinical Rockall score predicted mortality, but not rebleeding, in patients with LGIB. This might be because the Rockall score was originally developed to predict mortality in patients with UGIB (17). The modified GBS score failed to predict rebleeding or mortality in patients with LGIB. This study suggests, therefore, that the role of the clinical Rockall score can be extended to predict mortality in patients with LGIB.
An interesting finding was that high CRP levels were associated with high mortality in patients with LGIB in this study. High CRP levels were previously associated with the risk of rebleeding and mortality in patients with UGIB (1632), and the CRP level was similarly associated with the risk of mortality in patients with UGIB or LGIB in our study. So, patients with LGIB and high CRP levels should be subjected to close monitoring. As CRP is a marker of systemic diseases and represents a severe comorbidity, it may be a surrogate marker of severe comorbidity associated with poor outcomes in patients with LGIB as well as in patients with UGIB.
Our study has several advantages and limitations. This is the first study to compare clinical outcomes and risk factors of rebleeding and mortality by direct comparison of patients with LGIB to patients with UGIB in an Asian population. This study suggested a possible role for the clinical Rockall score and serum CRP levels as risk stratification markers in patients with LGIB, although this should be validated with further studies. In addition, the data collected in this study are of high quality, despite the retrospective study design, because only one physician (Y. J. Han) reviewed all medical records and entered information into the database. All possible and relevant risk factors associated with rebleeding and mortality in patients with UGIB or LGIB were simultaneously assessed in our study. This study suffers from some limitations. First, this is a retrospective, single-center study, which might limit the generalization of our findings. Second, this study was conducted with a limited number of patients. To overcome this limitation, we performed propensity score matching and minimized the risk of selection bias. However, we still need further prospective, large scale, multi-center studies. The retrospective nature of our study design also limited the data that could be collected.
In conclusion, the clinical outcomes of patients with LGIB are no better than the clinical outcomes of patients with UGIB. The clinical Rockall score and serum CRP levels can be used to predict 30-day mortality in patients with LGIB.
 XML Download
XML Download