

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Today, a precise estimation of the age of majority, 18 years old in western countries and 19 years old in Korea, has become a crucial issue worldwide due to the growth of migrants and refugees led by globalization and international conflicts (1). In the criminal judicial system, the age of a living young individual without valid identification can be estimated based on the combination of a physical inspection of the body, together with skeletal maturation (23). A developmental assessment of the third molar tooth, the carpal and wrist bones helps in estimating the age of infants and children, but their usage is limited in adolescents and young adults because the third molar tooth, hand, and carpal bones can all be fully developed before reaching the age of majority.
The Study Group on Forensic Age Diagnostics (AGFAD) has recommended radiographic evaluation of the medial clavicular epiphysis using a conventional X-ray examination and/or a computed tomography for age estimation if the skeletal maturation of the carpal and wrist bones is completed (4). In human skeletons, the secondary ossification center of medial clavicular epiphysis is the last to be unified (i.e., approximately 20 years), along with the humeral head, scapular acromion process, and ischial tuberosity (5). The clavicles are always covered on chest radiographs, which is the most commonly taken X-ray examination in medicine, whereas other separate X-ray examinations are needed to specify body parts. Age estimation by evaluating the epiphyseal ossification of the medial clavicle using chest radiography has been attempted in several studies to assess whether a subject is 18 years of age in western countries (67891011). The results, however, cannot be applied to domestic young individuals because skeletal maturation may be affected by race, socioeconomic status and the age of majority being differently defined as 19 years old (8121314).
In Korea, domestic crimes conducted either by adolescents or targeting adolescents are an increasing trend. In addition, because the inflow of North Korean defectors is growing (15), a reference standard for judging whether young defectors are under the age of majority is lacking. An age assessment of young defectors depends only on their allegation. Thus, it is of importance to develop a method for identifying young Korean individuals under the age of majority based on domestic data on the epiphyseal ossification of the medial clavicle. The aim of our study was to evaluate the utility and diagnostic accuracy of the ossification grade of medial clavicular epiphysis on chest radiographs for identifying Korean adolescents and young adults under the age of majority.
MATERIALS AND METHODS
Study population
The study initially enrolled 1,183 consecutive patients (a) whose age ranged from 16 to 30 years old; (b) who did not have any systemic disease potentially affecting the ossification of the medial clavicular epiphysis; and (c) who underwent preoperative chest radiography for local treatment in the department of otorhinolaryngology, ophthalmology, and plastic surgery from 2009 through 2012. Among the patients, 13 were excluded for the following reasons: 1) post-operative changes or foreign object obscuring the medial clavicles or 2) abnormal findings in the lung parenchyma or mediastinum hindering the image analysis of the medial clavicles. Finally, a total of 1,170 patients (664 men, 506 women; 73 to 80 patients at each age) were included in this study (Table 1).
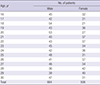
Image analysis
One chest and one musculoskeletal radiologist (S.H.Y. and H.J.Y.), each with 10 years of clinical experience, analyzed the chest radiographs of the included patients. The radiologists were blinded to patient clinical information, including sex and age.
The visibility and ossification grade of the medial clavicular epiphysis were separately assessed using a picture archiving and communication system workstation (Generation neXt viewer; INFINITT healthcare, Seoul, Korea) by the two readers. Because the optimum window level and width could differ on a case-by-case basis according to various factors affecting X-ray exposure, a fixed window setting was not applied. Once both the window level and width were lowered to enhance the opacity of bony structures, the readers were allowed to adjust the window settings for a few minutes to clarify the edge of the cortex and medulla at the medial end of the clavicle.
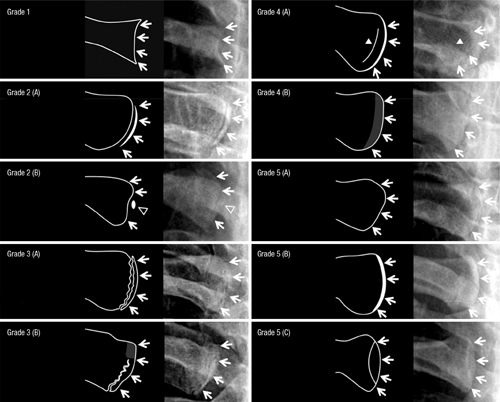
An attempt was made to visually distinguish the cortex and medulla at the medial end of the clavicle from adjacent bony and soft tissue structures, and the visibility of medial clavicle was categorized as inappropriate, possible, or appropriate for the image analysis (Table 2). The degree of ossification at the epiphyseal cartilage of medial clavicle was classified into five grades as follows (7): grade 1, invisible ossification center; grade 2, visible ossification center without any ossification of epiphyseal cartilage; grade 3, visible ossification center with partial ossification of epiphyseal cartilage; grade 4, complete ossification of epiphyseal cartilage with epiphyseal scar; or grade 5, complete ossification of epiphyseal cartilage without epiphyseal scar (Fig. 1).
Table 2
Categories and detailed descriptions for assessing the visibility of medial clavicular epiphysis on chest radiograph

Fig. 1
Representative images of each ossification grade.
White arrows indicate the cortical line at the medial end of clavicle. Grade 1 (invisible ossification center). The medial end of cortex is concave in shape and has an irregular margin with a thin cortical rim.; Grade 2 (visible ossification center without any ossification of epiphyseal cartilage). (A) The medial end of clavicle is convex in shape and has two layers of radiopaque cortical lines thicker than 1 mm at the full vertical length along with a full sharp radiolucent line with an even thickness which opens at both the top and bottom of the clavicle. (B) Epiphyseal ossification may be present as a less radiopaque density (empty arrow head) at the half of the vertical length; Grade 3 (visible ossification center with partial ossification of epiphyseal cartilage). The medial end of clavicle is convex or flat in shape and has two layers of radiopaque cortical lines thicker than 1 mm at a portion of the vertical length. The vertical radiolucent line has an irregular margin and thickness, which is interrupted (A) or closed by radiopaque area (B) either at the top or bottom; Grade 4 (complete ossification of epiphyseal cartilage with epiphyseal scar). (A) The medial end of clavicle is flat or convex in shape and has a broad cortical line 1-2 mm or thicker. There is no mach band phenomenon. Thin vertical line, epiphyseal scar (white arrow head) is visible adjacent to the cortical line. (B) The lateral margin may be amorphous and density of adjacent bone is mildly increased; Grade 5 (complete ossification of epiphyseal cartilage without epiphyseal scar). The medial end of clavicle is flat or convex in shape and has a thin even cortical line with an adjacent slit-like radiolucent line due to mach band phenomenon (A). The lateral margin of cortical line is even and sharp. The cortical line of medial clavicular end may be thicker up to 2 mm but evenness and sharpness are preserved at its full vertical length (B). Oblique positioning of the sternal facet at X-ray exposure may produce two layers of sharp radiopaque cortical lines thinner than 1 mm which are far apart at center and joined at the top and bottom resulting in a teardrop appearance (C).

Implementability
To facilitate implementation by less experienced radiologists and forensic doctors, practical instructional materials containing detailed descriptions and an image atlas were developed. Two radiologists (S.H.Y. and H.J.Y.) elaborated the detailed radiographic features of each ossification grade of the medial clavicular epiphysis and selected representative chest radiographs for the image atlas consensus (Table 2 and Fig. 1).
To evaluate the implementability of the instructional materials, one chest and one musculoskeletal radiologist (R.E.Y. and H.J.L.), who had 6 and 8 years of clinical experience, respectively, but were not experienced in classifying the ossification grade, reviewed one hundred chest radiographs from a subgroup of the patients. Two radiologists were first instructed on how to appropriately assess the visibility and ossification of the medial clavicular epiphysis. The subgroup was randomly selected from a total of the included patients while maintaining the age distribution within the subgroup. Then, the two readers independently categorized the visibility and ossification grade of the medial clavicular epiphysis.
Statistical analysis
The ossification grade at each age was expressed as a median and an interquartile range, and the distribution of ossification grades was skewed for ages ranging between 16 and 30 years. The age-ossification relationship was visually evaluated using a box-whisker plot and further explored by a regression curve-fitting analysis. The mean age in each grade was compared by sex using the Mann-Whitney U test and Student's t-test.
The percentage of agreement between the radiologists was calculated with regard to the assessment of visibility and ossification grade of medial clavicular epiphysis. The visibility of the medial clavicular epiphysis was dichotomized into inappropriate and possible/appropriate for the image analysis. Inter-observer agreement was evaluated using kappa statistics (16). A kappa value of less than 0.20 indicated poor agreement; a kappa value of 0.21–0.40, fair agreement; a kappa value of 0.41–0.60, moderate agreement; a kappa value of 0.61–0.80, good agreement; and a kappa value of more than 0.81, excellent agreement. To evaluate the variability of the medial clavicular epiphyseal ossification between the right and left clavicles, the averaged ossification scores of the two radiologists were separately calculated for the right and left clavicles; then, 95% limits of agreement were assessed by applying the mean ± 1.96 x the standard deviation of the difference between the right and left clavicles in addition to the correlation analysis using the Pearson correlation coefficient.
Receiver operating characteristic (ROC) analysis was used to analyze the diagnostic accuracy of ossification grade for determining whether the patient was under the age of majority. Because there may have been disagreement in the ossification grading of the observers, the ossification grades of two radiologists were averaged for the ROC curve, which plotted sensitivity on the y axis and its false positive rate (1-specificity) on the x axis, thus enabling an effective statistical analysis for assessing the performance of the diagnostic test (17). The actual age of the patients based on resident registration number was dichotomized into an age of 18 years old or younger (under the Korean age of majority) and an age of 19 years old or older (over the Korean age of majority), according to domestic law. The area under the curve (AUC) was calculated to quantify the diagnostic accuracy, and the cutoff averaged ossification grades that provided 95% specificity for identifying a person under the age of majority were assessed.
All statistical analyses were performed using the SPSS package (SPSS 22.0, Inc. Chicago, IL, USA) and the “pROC” package in the statistical software R. A P value less than 0.05 was considered to indicate statistical significance.
RESULTS
Among the 1,170 patients included in the image analysis, 19 of the patients were classified as inappropriate for chest X-ray image analysis by at least one radiologist (1.0% of included patients). Subsequently, the chest radiographs of 1,151 patients (99.0%) were evaluated for ossification grading.
Age-ossification relationship
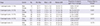
The median value of the averaged ossification grades increased with increasing age from 16 to 30 years (Fig. 2). The distribution of the averaged ossification grades for each age was similar between male and female. Additionally, the average age for each grade was not significantly different between sexes (Table 3). The trend was best fitted by a quadratic function (R-square, 0.978). The maximum and 3rd interquartile values of the averaged ossification grades reached 5.00 at age 18 and at age 22, respectively. The difference between the 1st and 3rd interquartile values of the averaged ossification grade within each age was larger than 1.0 between 18 and 21 years.

Table 3
Summary statistics in years by sex for ossification stages 1–5
Agreement on the visibility and ossification grade
In regard to the visibility of medial clavicular epiphysis, the percentages of agreement between the radiologists were 95.6% (1,118 of 1,170 cases) for the right side and 93.8% (1,098 of 1,170 cases) for the left side. The corresponding kappa values showed good agreement between the radiologists for both the right and left sides (i.e., 0.598 for the right and 0.735 for the left). With respect to the ossification grade of medial clavicular epiphysis, the inter-observer agreement was noted as 63.1% (726 of 1,151 cases) for the right side and 63.4% (730 of 1,151 cases) for the left side. The kappa values showed marginally moderate agreement between the radiologists for both sides (i.e., 0.420 for the right and 0.404 for the left). The 95% limits of agreement of averaged ossification grade for the right and left clavicles were between -0.95 and 0.96. The Pearson correlation coefficient between the averaged ossification grades for the right and left clavicle was 0.892 (P < 0.001).
Diagnostic accuracy
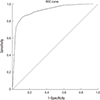
ROC analysis revealed that the diagnostic performance of the averaged ossification grade for determining whether the patient was under the age of majority (18 years old or younger versus 19 years old or older) was high, with a value of 0.922 (95% CI, 0.902-0.942), which was the best diagnostic value based on a sensitivity of 95.1% and a specificity of 74.9% at a cutoff value of 3.63 (Fig. 3). The sensitivities and specificities of the integer averaged ossification grade were 0.834 and 0.894 for grade 2, 0.726 and 0.958 for grade 3, and 0.443 and 0.977 for grade 4, respectively. A specificity of 95% was achieved for patients aged 18 or younger and for those aged older than 18 using averaged ossifications grades of 2.65 and 4.21, respectively.
Implementability
The percentages of agreement between the radiologists on the visibility and ossification grade of medial clavicular epiphysis were 91.5% (183 of 200 cases) and 56.5% (113 of 200 cases), respectively. The corresponding kappa values showed fair to good agreement between the radiologists (i.e., 0.450 and 0.318, respectively). An AUC of the averaged ossification grades of the inexperienced readers on a ROC curve was 0.860 (95% CI, 0.740-0.981).
DISCUSSION
In this study, we evaluated the ossification of the medial clavicular epiphysis in chest radiographs of Korean youth in terms of age distribution, inter-observer agreement, diagnostic accuracy, and implementability and developed practical instruction material. Between the ages of 16 and 30 years, the degree of epiphyseal ossification of the medial clavicle changed dynamically and a quadratic function showed that the averaged ossification grades increased with increasing age. These results are consistent with those of previous studies (67911).
Compared with the age ranges for each ossification stage presented in the literature (Table 4), the age minima in stages I to III are in accordance with the results of other studies (710181920212223242526). However, our age minima in stages IV and V were lower than the results presented in the literature, except for the study by Bassed et al. (22), although the proportion of subjects aged 20 years or younger was small, especially for stage V (Table 4). These differences in age minima for the complete fusion of the medial clavicle may originate from regional differences in skeletal maturation tempo, as Murata reported that skeletal maturation could progress 1 to 2 years earlier in East Asian populations than in others (27).
Table 4
Comparison of our result with previous studies dealing with the ossification of the medial clavicular epiphysis
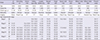
| Study | Jit (18) | Schmeling (7) | Schulz (19) | Kellinghaus (20) | Langley-Shirley (21) | Bassed (22) | Singh (23) | Garamendi (10) | Brown (24) | Wittschieber (25) | Wittschieber (26) | Present study | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Year | 1976 | 2004 | 2005 | 2010 | 2010 | 2011 | 2011 | 2011 | 2013 | 2014 | 2016 | 2016 | |
| Patient No. | 684 | 699 | 556 | 502 | 1289 | 674 | 343 | 123 | 1035 | 493 | 309 | 1,151 | |
| Patient age, yr | 11-30 | 16-30 | 15-30 | 10-35 | 11–33 | 15-24 | 17- | 5-75 | 16-32 | 10-40 | 15-30 | 16-30 | |
| Nationality | Indian | German | German | German | American | Australian | Indian | Spanish | Ghanaian | German | German | Korean | |
| Imaging | Gross | Chest X-ray | CT | CT | Gross | CT | Gross | Chest X-ray | Chest X-ray | CT | Clavicle X-ray | Chest X-ray | |
| Age range at each stage | |||||||||||||
| Stage I | M | 10.0–16.0 | ≤18 | 15-21 | 17-21 | 15.5–18.5 | 16–20 | 10.7–14.9 | 16-17 | ||||
| F | 10.1–15.9 | ≤19 | 15-19 | 17-21 | 16–19 | 12.1–15.4 | 16-17 | ||||||
| Stage II | M | 14-21 | 15.2??3.9 | 14.4–20.3 | 13–24 | 15-25 | 18-23 | 16–24 | 15.0–20.4 | 16-24 | |||
| F | 11-21 | 15.0??1.6 | 13.1–19.3 | 15–23 | 15-21 | 18-22 | 16–22 | 14.1–18.4 | 16-24 | ||||
| Stage III | M | 18-24 | 16.7–24.0 | 17.5??7.2 | 17.5–26.2 | 17–29 | 17-25 | 18-25 | 17.8–45.6 | 18–31 | 16.4–36.5 | 16.1–29.7 | 16-30 |
| F | 18-23 | 16.0–26.8 | 16.6??8.6 | 16.8–26.2 | 17–26 | 17-25 | 20-27 | 17–30 | 15.5–26.5 | 15.0–30.6 | 16-27 | ||
| Stage IV | M | 22-30 | 21.3–30.9 | 21.2??0.4 | 21.6–35.9 | 19–30 | 17-25 | 19-32 | 19.7–32.9 | 21–32 | 21.6–40.5 | 22.5–30.9 | 18-30 |
| F | 23-30 | 20.0-30.9 | 21.5??9.9 | 21.3–35.2 | 20–31 | 19-25 | 19-30 | 20–32 | 21.1–37.3 | 21.1–26.4 | 17-30 | ||
| Stage V | M | 26.0–30.4 | 22.4??0.9 | 26.4–35.8 | ≥19 | 17-25 | 22-32 | 20.6-75.4 | 25–32 | 26.6–40.0 | 26.0–30.9 | 18-30 | |
| F | 26.7–30.9 | 21.9??0.9 | 26.1–35.7 | ≥22 | 20-25 | 22-32 | 25–32 | 26.7–39.6 | 26.3–30.9 | 18-30 | |||
There was good inter-observer agreement in terms of the visibility of the medial clavicular epiphysis, and only 1% of the patients were classified as inappropriate for the image analysis, thus indicating that the chest radiograph may be generally used for ossification grading in a young population. In contrast, for the ossification grade, the percentages of agreement between readers were approximately 60%, with marginally moderate kappa values. It is impossible to identify the actual degree of epiphyseal ossification in practice, though computed tomographic examination or gross anatomy may be used as a reference standard. Thus, to minimize misinterpretation or potential subjective bias in the reading of a single reader (11), we averaged the ossification grades of two readers to determine whether a person is under the age of majority. Averaging the ossification grades subdivided the original ossification grades, which were expressed as integers, into grades with two decimal points, which helped achieve a higher AUC of 0.922 (95% CI, 0.902-0.942) and refine a cutoff value that provided 95% specificity for defining the age of majority (ossification grade, 2.65 for patients aged 18 or younger and 4.21 for those over 18).
We preliminarily validated the clinical implementability of the ossification grading at the medial clavicular epiphysis by inexperienced radiologists by introducing our instructive material. The instructive material allowed the inexperienced readers to promptly understand the grading method, which resulted in an AUC of 0.860 on the ROC curve with fair agreement between the readers based on kappa statistics. However, the inexperienced radiologists achieved not only lower inter-observer agreements but also lower diagnostic performance than did the experienced radiologists. Such limitations of the instruction material are expected to be improved by with learning time, given that the less experienced readers had experienced only one hundred ossification grades during the image analysis and the more experienced readers, who achieved an AUC of 0.922, had never experienced ossification grading prior to this study.
Although our instruction material contains detailed descriptions and the corresponding representative images for inexperienced readers, it is unknown whether it enables non-radiologist (i.e., forensic doctors) to properly classify the ossification grade. The medial end of the clavicle overlapped with adjacent soft tissue or bony structures in a substantial number of the patients, with their visibility classified as 'possible' or 'appropriate' for the image analysis. This implies that the reader should recognize the degree of epiphyseal ossification while visually separating the medial end of the clavicle from the overlapping opacity. It may be a difficult task for non-radiologists who are unfamiliar with X-ray film interpretation. Further investigation is needed to ascertain whether our instructional material is sufficiently understandable to non-radiologists. In that respect, when grading the epiphyseal ossification of the medial clavicle in practice, at least one radiologist is recommended to participate as an observer in the reader pairs.
The cutoffs for the averaged ossification grades for identifying a person under the age of majority were devised to provide 95% specificity but are not anticipated to be used as definite evidence in criminal judicature because 95% specificity literally excludes 5% of exceptional cases. Indeed, despite the high AUC of 0.922 on ROC analysis, considerable overlaps in the interquartile range (18 years, 2.5-4.00; 19 years, 2.75-4.00) and range (2.00-5.00, each) existed between 18 and 19 years of age. Epiphyseal ossification during skeletal maturation can be affected by socioeconomic and nutritional factors that were not incorporated in this study. Furthermore, in approximately 10% of the cases, the ossification grade of the medial clavicular epiphysis could be underestimated on the chest radiograph when an oblique radiograph of the clavicle served as the reference standard (28). Nevertheless, an assessment of medial clavicular ossification by chest radiograph along with the suggested cutoffs can be useful for the mass screening of young people with deceitful allegations for their age to select candidates for further evaluation (i.e., age estimation for young fugitives from North Korea in case of a sudden collapse) because chest radiographs are taken for all fugitives from North Korea to assess the presence of pulmonary tuberculosis.
There are several limitations to this study. First, the number of patients at each age was relatively small, and all were included from a single center. The effect of socioeconomic or nutrition status on the epiphyseal ossification was not evaluated (8), although an extremely low socioeconomic or nutrition status potentially affecting skeletal maturation is quite rare in the young Korean population. A lack of correlation with computed tomographic (192029) or anatomic evaluation (23) may be another limitation of our study, despite the impracticability of these methods in the general young population. In addition, it needs to be further validated whether the suggested cutoff of 95% specificity for defining the age of majority can be generalized to other radiologists who possess sufficient experience in ossification grading.
In conclusion, the age of majority of Korean adolescents and young adults may be estimated from chest radiographs with marginally moderate inter-observer agreement and high diagnostic accuracy. This age assessment method could potentially be implemented in practice after introducing the practical instructional material. Subsequent research of North Korean adolescents and young adults (i.e., North Korean defectors) will provide a scientific basis for the mass screening of young populations around the age of majority in preparation for a possible increase in demand for estimating the age of fugitives from North Korea in case of a sudden change.
 XML Download
XML Download